
Abstract
Objective
To determine whether there are differences in symptomatic knee cartilage defects and rates of tobacco use among age-matched athletes versus nonathletes undergoing initial arthroscopic knee surgery who meet demographic and radiographic criteria for cartilage restoration surgery.
Design
Age-matched athletes (n = 186) and nonathletes (n = 159) age 40 or less with a body mass index (BMI) of 35 kg/m2 or less (mean 26.8 SD 4.1) and <50% joint space narrowing on weight-bearing radiographs were included. All patients had a symptomatic Outerbridge grade 2 or higher cartilage defect visualized during knee arthroscopy. Relationship between athletic status and chronicity of knee symptoms prior to surgery and tobacco use status, cartilage defect Outerbridge grade, size, and location at time of surgery were characterized.
Results
Nonathletes were more likely to smoke (P < 0.001) and had higher BMI (P = 0.005). Duration of symptoms prior to surgery was shorter among athletes (P < 0.001). Grade 4 defects were equally prevalent (P = 0.96) as were multicompartment grade 3-4 lesions (P = 0.12). Mean grade 3-4 defect size was similar in lateral (P = 0.96) and medial compartments (P = 0.82). There was a trend toward larger anterior compartment defects in nonathletes (P = 0.07).
Conclusions
Among age-matched athletes and nonathletes with symptomatic cartilage defects who meet demographic criteria for cartilage restoration, nonathletes were more likely to smoke and have a longer duration of symptoms prior to treatment. Athletes tended to present earlier but with similar size defects compared to nonathletes, supporting accelerated treatment of defects in athletes and caution toward allowing continued athletic participation in patients with known cartilage defects.
Introduction
Hyaline cartilage in the knee joint permits frictionless articulation within the joint, as well as permitting highly effective shock-absorption, which is especially important in the athlete. Articular cartilage injuries of the knee are encountered quite commonly by orthopedic surgeons, with approximately 200,000 to 300,000 cartilage defect procedures being performed annually in the United States. 1 Patients presenting with symptomatic defects will typically display long-standing activity-related swelling accompanied by knee pain, which can be highly debilitating, 2 and in younger patients, full-thickness defects have been shown to produce a quality of life similar to those with severe knee osteoarthritis awaiting arthroplasty. 3 Given the limited regenerative capacity of cartilage due to its avascular nature, cartilage injury may lead to early-onset arthritis.4,5 Existing cartilage damage is associated with accelerated local cartilage damage6-11 and can increase risk of subsequent cartilage damage in other subregions of the knee. 12
While focal knee cartilage defects cause significant pain and functional limitations in the general population, they are also prevalent in athletic populations. A systematic review from Flanigan et al. found a 36% prevalence of full-thickness focal cartilage defects in athletes, with 14% being asymptomatic at time of diagnosis. 13 Given the varying demographics and functional demands on the knee joint between athletic and sedentary populations, these populations may display unique patterns of cartilage lesion when presenting with persistent knee symptoms. It is unknown whether cartilage defect size or location differs significantly between symptomatic athletes and nonathletes. Perhaps more important, it is unclear whether arthroscopically assessed symptomatic knee cartilage defect characteristics differ among athletes and nonathletes who meet demographic (age under 40 years and body mass index [BMI] under 35) and radiographic (<50% joint space narrowing on weight-bearing radiographs) criteria for cartilage restoration surgery. Similarly, though tobacco use has a likely negative effect on cartilage restoration outcomes, 14 it is unclear whether tobacco use rates differ between athletes and nonathletes that meet cartilage restoration criteria.
The purpose of the current study is to determine whether there are differences in symptomatic knee cartilage defect chronicity, size, grade, or location as well as rates of tobacco use among age-matched athletes versus nonathletes undergoing initial arthroscopic knee surgery who meet demographic and radiographic criteria for cartilage restoration surgery. We hypothesize that athletes will have lower tobacco use rates and have a tendency to present for treatment earlier and with smaller, lower grade defects than nonathletes.
Methods
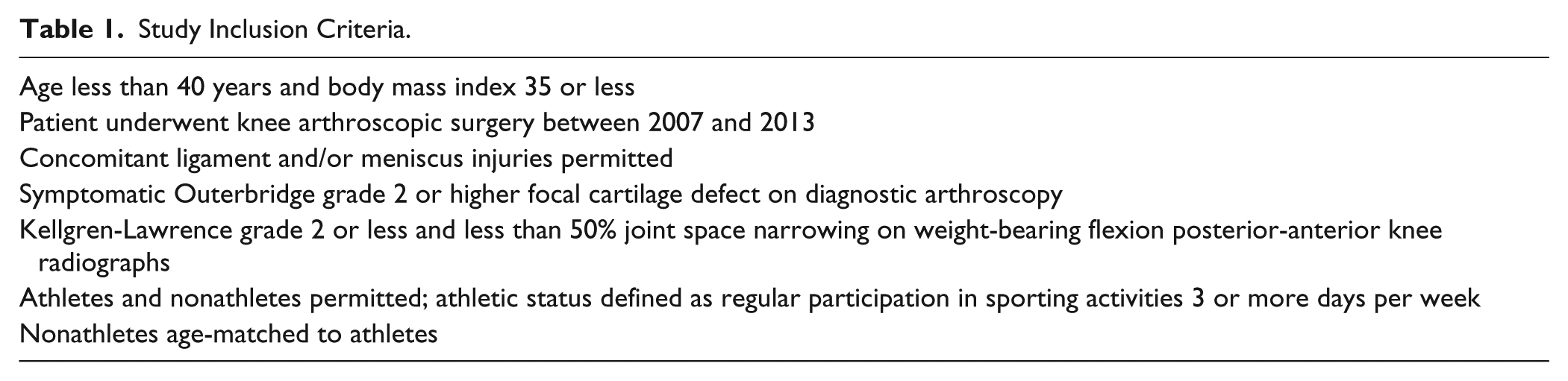
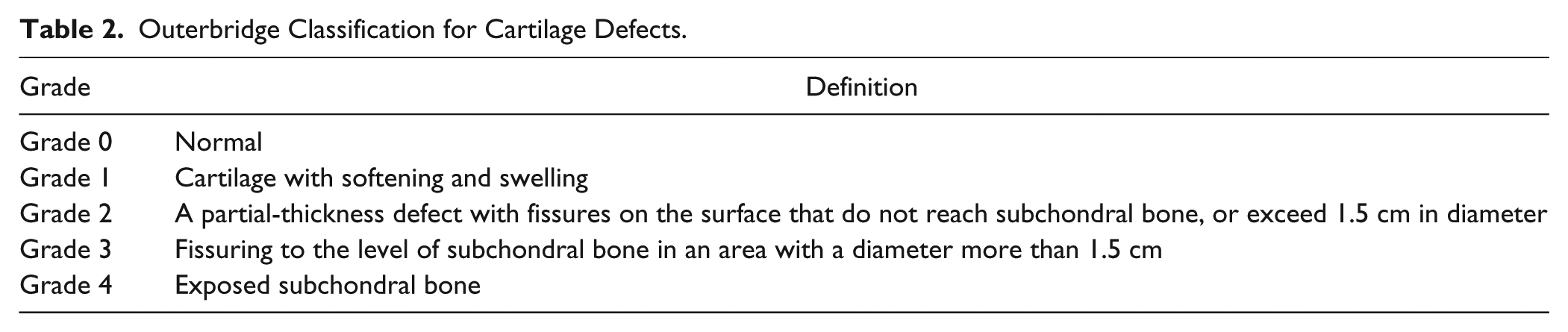
Patients (476 athletes, 511 nonathletes) who underwent arthroscopic knee surgery at a single institution between 2006 and 2013 were reviewed ( Table 1 ). Consecutive cases were reviewed and patients were excluded if they were over 40 years of age, had a BMI over 35 kg/m2, or had significant existing osteoarthritis (defined as Kellgren-Lawrence grade 3 or higher or greater than 50% joint space narrowing on weight-bearing flexion posterior-anterior radiographs) 15 ; these demographic and radiologic exclusion criteria are commonly utilized for consideration for cartilage restoration or replacement surgery.16,17 All patients had at least one focal Outerbridge grade 2 or higher cartilage defect ( Table 2 ). 18 Patient age is strongly correlated with prevalence and grade of cartilage damage. 19 Therefore, athletes were age-matched to nonathletes in the current study. After application of these criteria, a total of 186 athletes (mean age 30.0 years SD 7.1) and 159 nonathletes (mean age 29.0 SD 6.1) (n = 345 total) were included in the study analysis. An a priori power analysis was performed and the study sample size was determined to be adequate to detect a mean 12% difference in prevalence of tobacco use, a mean 50-day difference symptom duration, and a mean 0.7 cm2 difference in mean grade 3-4 defect size with 80% power and alpha = 0.05.
Study Inclusion Criteria.
Outerbridge Classification for Cartilage Defects.
Cartilage lesion size, Outerbridge grade, 18 and number of lesions were documented by direct visualization during the diagnostic arthroscopic portion of the planned knee procedure. Clinical data including activity level, concomitant injuries, tobacco use status, and history of prior knee injuries or surgeries were obtained via medical record review. Symptom duration was defined as the time from symptom onset to day of surgery.
Statistical Analysis
Statistical analysis was performed with a standard software package (STATA 13.0, College Station, TX). Descriptive statistics were first generated for the entire sample after stratification by athletic status. Differences in categorical variables were assessed by chi-square test and differences in ordinal variables were assessed by Cochrane Armitage test. Differences in continuous variables were assessed via Student’s t test or Wilcoxon rank sum for variables with normal versus nonnormal distributions, respectively. Multivariate regression was used to determine whether athletic status was independently predictive of grade 3-4 defect size and presence of multicompartment grade 3-4 cartilage defects after adjustment for symptom duration and prior history of ipsilateral knee surgery; these covariates were selected a priori due to clinically significant differences in these variables at baseline between athletes and nonathletes. Though age and BMI likely affect cartilage defect size, these covariates were not included in the multivariate analysis as athletes and nonathletes had clinically insignificant differences in mean age or BMI. For the multivariate analyses, a Johnson’s Su transformation was first performed for symptom duration to achieve a normal distribution; these transformed values for symptom duration were then used in a linear regression model. A linear regression model without any transformations was used to model defect size, and a logistic regression model was used for model presence of multicompartment defects.
Results
Demographic and Clinical Differences between Athletes and Nonathletes
The primary sport among athletic patients, in descending order, was American football (19%), basketball (17%), soccer (17%), running (12%), baseball or softball (5%), volleyball (4%), and cycling (3%); the remaining primary sports each represented <3% of all athletes in the study sample. Compared to athletes, nonathletes were more likely to smoke tobacco (31% vs. 12%, P < 0.001) and had a slightly higher BMI (27.6 kg/m2 SD 4.4 vs. 26.2 SD 3.6; P = 0.005), which was statistically significant but not of clinical significance ( Table 3 ). There was a nearly 6-month difference in median duration of symptoms prior to arthroscopic knee surgery, with a median duration of 104 days among athletes and 282 days among nonathletes (P < 0.001). Nonathletes were more likely to have a history of previous ipsilateral knee surgery (42%) compared to athletes (26%) (P = 0.002). Athletes were more likely to present with a concomitant ligamentous injury, and the rate of concurrent ACL (anterior cruciate ligament) reconstruction at time of knee arthroscopy was 37% for athletes and 21% for nonathletes (P = 0.002).
Patient Demographics.
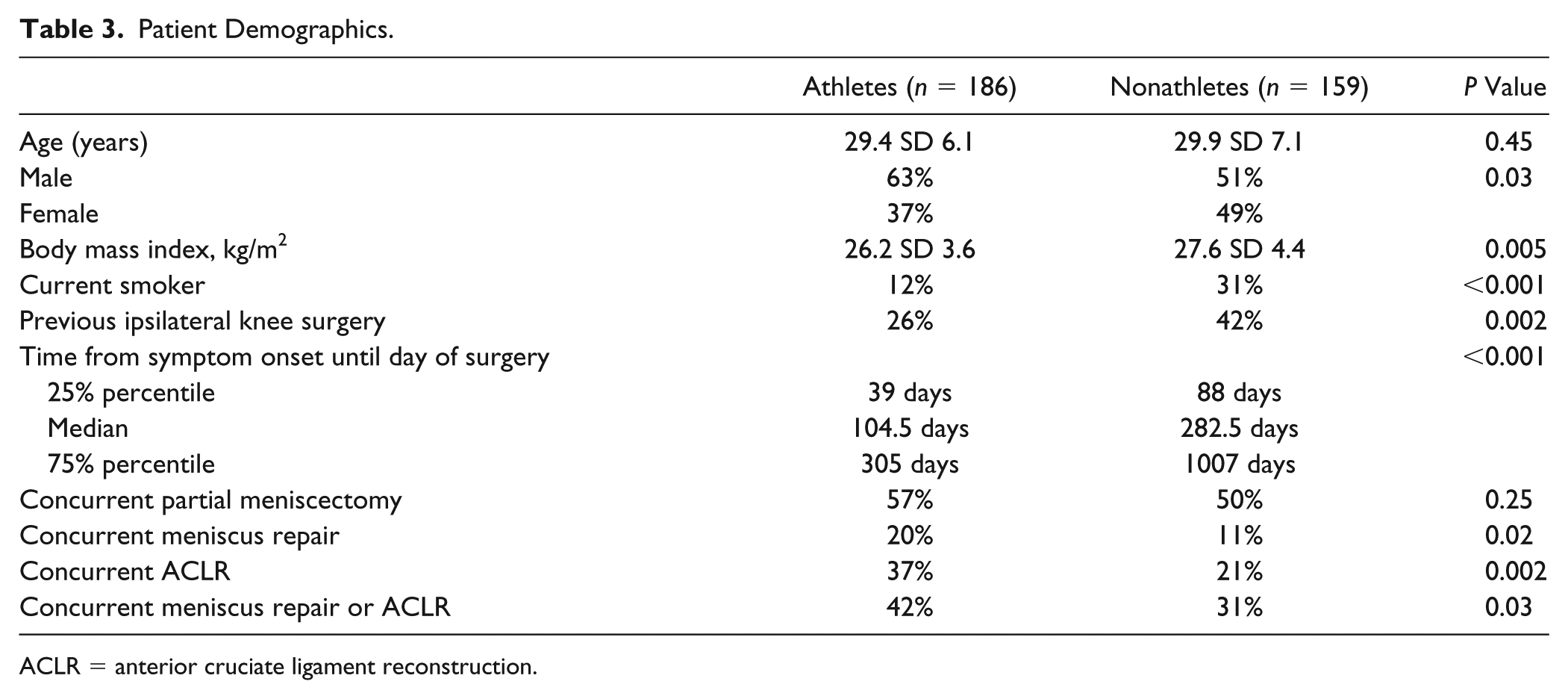
ACLR = anterior cruciate ligament reconstruction.
Cartilage defect characteristics among athletes and non-athletes
Grade 4 defects were equally prevalent among athletes (35%) and nonathletes (35%) (P = 0.96), and there was no association between athletic status and the highest grade defect visualized during knee arthroscopy (P = 0.31, Cochrane Armitage trend test) ( Table 4 ). In the unadjusted analyses, the prevalence of multicompartment grade 3-4 defects were similar in both groups (14% nonathletes, 9% athletes, P = 0.12) ( Table 4 ). Mean grade 3-4 defect size was similar in the lateral (mean 3.0 cm2 SD 3.2 nonathletes, 2.9 SD 3.1 athletes, P = 0.96) and medial compartments (3.6 cm2 SD 2.9 athletes, 3.3 SD 4.2 nonathletes, P = 0.82) but there was a trend toward larger anterior compartment defects in nonathletes (4.4 cm2 SD 5.5) versus athletes (2.8 SD 2.3; P = 0.07) ( Table 4 ).
Cartilage Defect Characteristics.
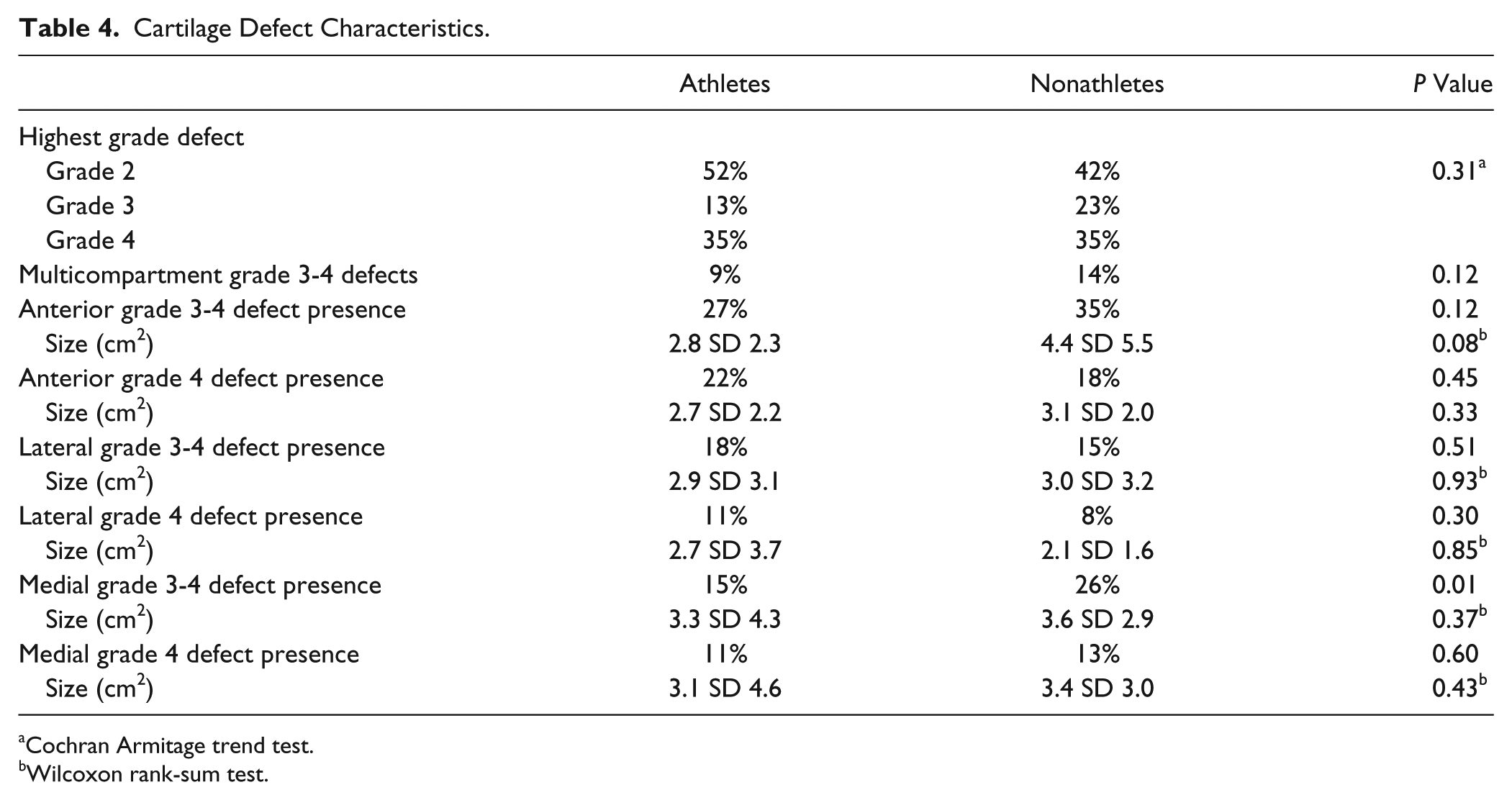
Cochran Armitage trend test.
Wilcoxon rank-sum test.
Independent Association between Athletic Status, High-Grade Cartilage Defect Size, and Likelihood of Multicompartment High-Grade Cartilage Defects
In the multivariate analysis, after adjusting for symptom duration and history of ipsilateral knee surgery, nonathletes still had a trend toward larger anterior compartment grade 3-4 defects when present (adjusted mean size 4.7 cm2 SE 0.7 nonathletes; adjusted mean 2.6 SE 0.8 athletes; P = 0.05) ( Table 5 ). There was no difference in the mean adjusted medial (P = 0.80) or lateral (P = 0.95) grade 3-4 defect size when present among athletes or nonathletes in the multivariate analysis ( Table 5 ). Finally, after adjusting for surgical history and symptom duration, there was no increased odds of multicompartment high-grade (grade 3-4) defect present among nonathletes compared to athletes (adjusted odds ratio = 1.32, 95% confidence interval = 0.61, 2.89; P = 0.48) ( Table 6 ). However, increased symptom duration was independently associated with a higher likelihood of high-grade defects in multiple compartments (P = 0.01) ( Table 6 ).
Adjusted Association between Athletic Status and Defect Size.
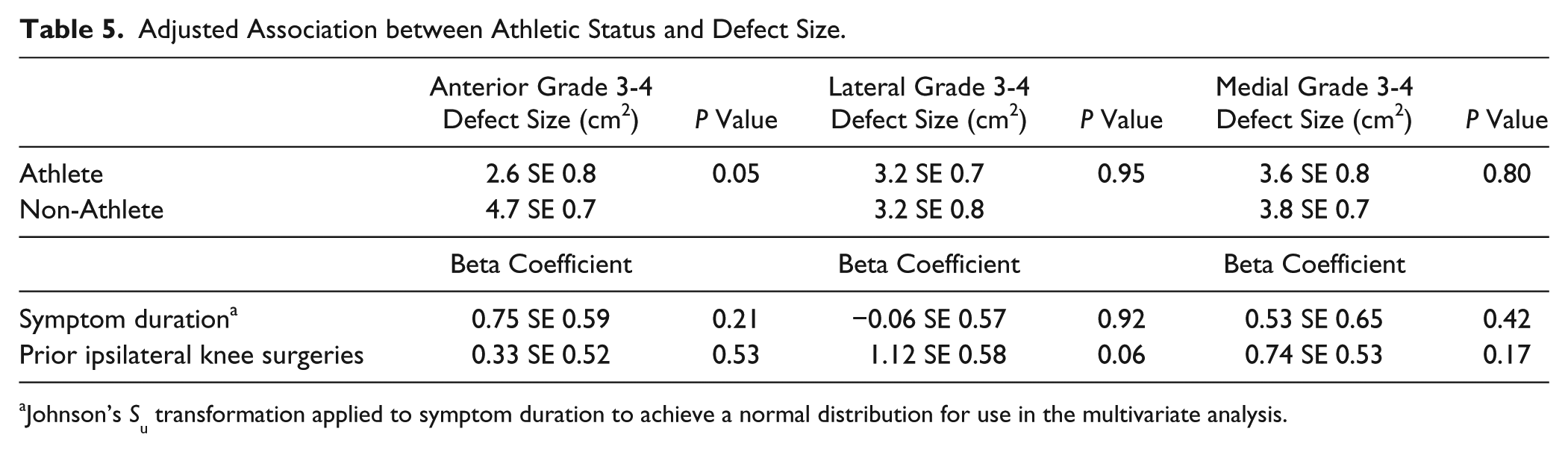
Johnson’s Su transformation applied to symptom duration to achieve a normal distribution for use in the multivariate analysis.
Adjusted Risk of Multicompartment Grade 3-4 Chondral Defects.
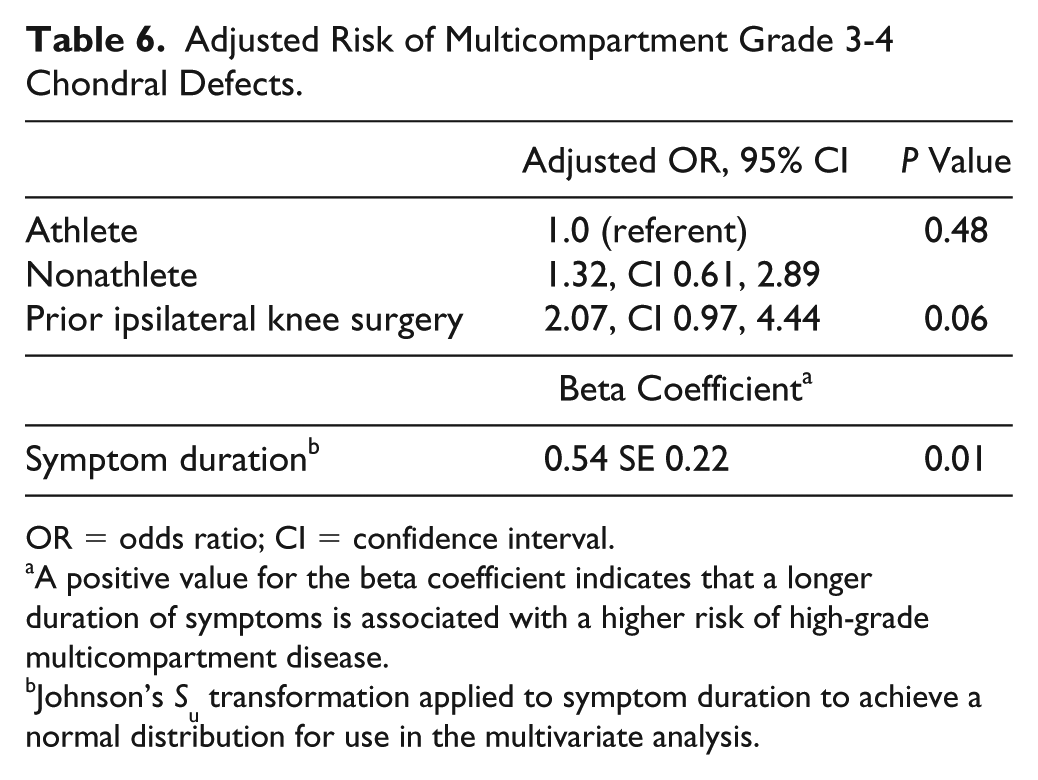
OR = odds ratio; CI = confidence interval.
A positive value for the beta coefficient indicates that a longer duration of symptoms is associated with a higher risk of high-grade multicompartment disease.
Johnson’s Su transformation applied to symptom duration to achieve a normal distribution for use in the multivariate analysis.
Discussion
Articular cartilage injuries in the knee are common in both athletes and nonathletes, producing significant pain and functional limitations, although they may present differently among these populations. In the current study, among athletic and nonathletic patients who meet demographic and radiographic criteria for cartilage restoration, nonathletes were substantially more likely to smoke tobacco and have a longer duration of symptoms prior to knee arthroscopy. The current study findings have important implications in the interpretation of cartilage treatment outcome studies, as differences in tobacco use and symptom duration by activity level may correspondingly result in differences in treatment outcomes.
There are several potential reasons that athletes had a shorter average duration of symptoms than nonathletes. A larger proportion of athletes had concomitant ACL tears that would lead to earlier presentation for treatment. In the case of isolated cartilage defects, the higher functional demands associated with athletic activity may also exacerbate symptoms that may have otherwise gone undetected. It has been shown that proprioceptive acuity in athletes is correlated with sport competition level achieved, highlighting the importance of proprioception in athletic performance. 20 This increased proprioceptive ability may permit a greater ability to sense injury presence within the body, especially when the chondral injuries are present while the athlete is participating in athletic activities. It is possible that nonathletes may tolerate chondral injuries longer than athletes due to a lack of rapid stop-start movements, as return to rapid stop-start movements following cartilage restoration is not as well tolerated as return to lower intensity activities. 21 Furthermore, the finding that while size of defects among athletes and nonathletes was not significantly different, though duration of symptomology among athletes was significantly shorter compared to nonathletes, seems to suggest that even a relatively short duration of symptoms in athletes can indicate rapid increase in cartilage defect size in comparison to non-athletes with similar symptoms. This may support more expedited treatment of athlete cartilage defects.
The longer median symptom duration in nonathletes is a risk factor for worse outcomes following treatment, as there is ample evidence to indicate chronic lesion respond less well to cartilage therapies. 1 Greater symptom chronicity is associated with worse outcomes following cartilage defect treatment in athletes,1,22 even in adolescent populations. 23 Biant et al. report a 26% failure rate at a mean 5.7 years following autologous chondrocyte implantation (ACI) for chronic cartilage lesions, 24 and Vanlauwe et al. found that characterized chondrocyte implantation (CCI) resulted in better Knee Injury and Osteoarthritis Outcome Scores (KOOS) than microfracture only if the patient had <3 years of preoperative symptoms. 25 In a study of microfracture versus ACI for chronic isolated femoral condylar defects, Knutsen et al. found high failure rates both ACI and microfracture as well a 57% (ACI) and 48% (microfracture) prevalence of early osteoarthritis among patients without failure at 14- to 15-year follow-up. 26 Additionally, existing cartilage damage can increase risk of subsequent cartilage damage in other subregions of the knee, 12 and longer symptom duration was independently associated with increased risk of high-grade multicompartment disease in the current study. Thus, earlier diagnosis and treatment of cartilage lesions among athletes and nonathletes alike is paramount to treatment success and resolution of symptoms.
The prevalence of tobacco use among nonathletes in the current study is unexpectedly high (31%), as the prevalence of tobacco use among adults in our state is estimated at 22.5%. 27 In addition, the tobacco use among athletes was 12%, which also was surprisingly high. Reported rates of tobacco use among athletes range from 4.1% to 9.4%. 28 However, other studies report rates of tobacco use (smoking and smokeless) among athletes of between 0.8% and 15%. 29 The higher rate of tobacco use in nonathletes could adversely affect outcomes following ACI in particular. Schmal et al. demonstrated in a controlled laboratory study that the synovial fluid of microfracture and ACI subjects had lower cytokine expression related to cartilage metabolism. 30 Jaiswal et al. found in a study of 128 patients treated with ACI that smokers had lower mean Modified Cincinnati Knee scores at 2 years follow-up and a strong negative correlation between symptom scores and number of cigarettes smoked; they also noted that smokers had lower proportion of excellent or good results per International Cartilage Repair Society arthroscopic assessment. 31 Niemeyer found a trend toward lower Lysholm scores (P = 0.06) among tobacco users following treatment of retropatellar cartilage defects with ACI. 32 The reported effect of smoking following microfracture is mixed. Balain et al. found no effect of smoking in a study of 53 patients tread with microfracture for isolated full-thickness defects 33 ; however, Spahn et al. found a significant negative effect of smoking on KOOS scores in a study of 156 patients treated with microfracture or chondroplasty with medial unicompartmental osteoarthritis at 47- to 54-month follow up. 34 Finally, there is currently no demonstrated effect of smoking on procedures involving transfer of osteoarticular autograft; Ollat et al. found no effect of smoking on outcomes following mosaicplasty of osteochondral defects in 142 patients at mean 96 month follow-up. 35
Smaller defects tend to have better outcomes following cartilage therapies. 1 Other than a trend toward larger high-grade anterior compartment defect size among nonathletes, no difference in size, location, or severity was observed among age-matched athletes and nonathletes in the current study. Nonathletes may present with larger high-grade defects of the anterior compartment as our data suggest nonathletes tend to present at later stages of disease in general. Interestingly, symptom duration was not significantly correlated with high-grade defect size in the current study, though prior reports have indicated that cartilage defects can accelerate local cartilage damage.6-11 The prevalence of full-thickness defects among athletes in the current study (35%) is consistent with the prevalence of full-thickness defects reported in a review by Flanigan et al. (36%) among athletes with a mean age of 33 years. 13 In contrast, Curl et al. describes a full-thickness defect prevalence of 19.5% in 31,516 knee arthroscopies of patients with a mean age of 43 years. 36 The mean high-grade defect sizes in the current study correspond with Arøen et al., who found in a series of 993 consecutive knee arthroscopies, that 55% of full-thickness defects were greater than 2 cm2 in size. 37
Limitations
The study has several strengths and limitations. The current study was restricted to symptomatic patients who meet age, BMI, and radiographic criteria for cartilage restoration, improving the applicability of results to cartilage restoration outcomes research. Use of age-matching eliminated a known potential source of bias when comparing athletes to nonathletes as age is strongly correlated with prevalence and grade of cartilage damage 19 and is also correlated with tobacco use rates. 38 The study was adequately powered to detect clinically meaningful differences in symptom duration, rates of tobacco use, and high-grade defect size. Arthroscopic evaluation of symptomatic cartilage defects remains superior to magnetic resonance imaging, as magnetic resonance imaging has lower sensitivity 39 and tends to underestimate lesion size. 40 The study findings are not applicable to an asymptomatic population as the characteristics of symptomatic defects may differ from asymptomatic defects. In addition, the frequency of athletic participation among each sporting group is unavailable in our dataset, limiting the understanding of the level of participation among included athletes. Our data also do not include analysis or presentation of types of ipsilateral previous knee surgeries among athletes and nonathletes. Additionally, the tobacco use rates identified in the current study may not be applicable to populations outside of the United States as there is substantial variation by country in tobacco use rates. 41
Conclusion
Among age-matched athletes and nonathletes with symptomatic cartilage defects who meet demographic criteria for cartilage restoration, nonathletes were more likely to smoke tobacco and have a significantly longer duration of symptoms prior to treatment. High-grade anterior defects may be larger in nonathletes though defect size, grade, and likelihood of multicompartment defects are otherwise similar between groups. These differences may in part explain the discrepancy in outcomes noted between athletic and nonathletic populations following cartilage procedures.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Flanigan receives funding from Depuy Mitek, Inc., Smith & Nephew, Vericel, Ceterix Orthopaedics, Conmed, Histogenics Corporation, and Zimmer Inc. The other authors have no conflicts of interest to disclose.
Ethical Approval
This project was approved by the Biomedical Institutional Research Board of The Ohio State University No. 2013H0066.
Informed Consent
Written informed consent was obtained from all subjects before the study.