
Abstract
Objective
The etiology of osteochondritis dissecans (OCD) is still uncertain. Recently, it has been hypothesized that instability of the anterior horn of the meniscus is an important cause for the development of a nontraumatic OCD in adolescents with good results after surgical stabilization. This case series aims to evaluate the treatment results after meniscus stabilization in adults with nontraumatic OCD.
Design
Ten patients with magnetic resonance imaging (MRI)-confirmed OCD of the knee joint, meniscal instability, and closed epiphyseal plates were enrolled in this study. The instable meniscus was stabilized by direct suturing of the anterior horn of the meniscus. MRI examinations were performed preoperative and 6 and 12 months postoperative. The OCD was classified arthroscopically according to Guhl and according to Hughes in the MRI. The overall knee function was evaluated by the Lysholm score before treatment and 12 months postoperative.
Results
Four women and 6 men with a mean age of 20.6 ± 1.9 years were included in this study. Preoperatively 60% of the patients showed a grade II or III lesion arthroscopically and 70% a grade III or IVa lesion in the MRI examination. After arthroscopic meniscus stabilization the Lysholm score increased in average from 48.1 ± 14.12 before treatment to 97.5 ± 3.1 postoperative. At final follow-up after 12 months, an improvement of the OCD in the MRI could be demonstrated in all patients (100%). In 80% of the patients a complete healing of the OCD could be noted.
Conclusion
The clinical concept of an instable anterior horn of the meniscus as a cause for the development of a nontraumatic OCD seems to be transferable to adults and arthroscopic stabilization can lead to a sufficient healing of this knee pathology.
Introduction
Osteochondritis dissecans (OCD) of the knee joint is frequent.1,2 It is responsible for long sport absences and persisting pain during weight-bearing, especially in adolescents and young adults.1,3 However, the etiology of this knee joint pathology as well as adequate and consistent treatment strategies are still uncertain.4,5 OCD is mostly explained by repetitive microtrauma or disorders in blood supply.6-9 However, recently a study postulated an instability of the anterior horn of the meniscus as a cause for the development of a nontraumatic OCD in the knee joint of adolescents. 10 This clinical concept has been called “door stop phenomenon.” The physiological anterior translation of the meniscus during extension is thus delayed by the instability of the anterior horn. This results in an entrapment of the meniscus between femur and tibia and a fast forward click to the original position in full extension. Stabilization of the anterior horn of the meniscus by suturing led to sufficient healing of the OCD with comparable results to patients after screw fixation but faster recovery. 10 It is however unclear whether a meniscus instability is also an important reason for nontraumatic osteochondral pathology in adults. Therefore, this case series wants to evaluate the treatment results after meniscus stabilization in adults with nontraumatic OCD. We hypothesized that this treatment method will lead to complete healing of the OCD in adults.
Methods
Ten patients referred to our hospital between January 2015 and December 2016 were included in this retrospective study. This study has been approved by the ethical and institutional review board of the hospital before commencement and meets the ethical standards of this journal.
All patients were adults and forced to quit sport activities because of pain within the knee joint at athletic loads. Inclusion criteria were the following: patient age ⩾18 years, closed epiphyseal plates, persistent knee joint pain, magnetic resonance imaging (MRI)-confirmed OCD of the knee joint with clinical symptoms and meniscal instability at the time of surgery, as defined later. All patients failed a 6-month course of conservative treatment, including partial weight-bearing, activity modification with sport cessation, physiotherapy, and vitamin D/calcium supplementation. Exclusion criteria included osteoarthritis with a Kellgren-Lawrence score >2, medial or lateral deviation of the mechanical axis >10 mm, prior significant ligament injury, meniscal lesion, anatomic meniscal variants (discoid meniscus), generalized inflammatory arthritis, systemic diseases, pregnancy, severe infection, known malignancy, bleeding disorders or anticoagulation, previous knee surgery, extracorporeal shock wave therapy, corticosteroid injection into the knee joint, and finally nerve-related symptoms such as radiculopathy.
MRI Examination
Magnetic resonance imaging of the respective knee joint was performed prior to the surgical treatment and 6 and 12 months postoperative. All 10 patients were imaged on the same 3.0-T MRI scanner (Avanto; Siemens Medical Systems, Erlangen, Germany) using an 8-channel phased-array extremity coil. All MRI examinations consisted of an axial frequency-selective fat-suppressed T2-weighted fast spin-echo (FSE) sequence, a coronal intermediate-weighted FSE sequence, a coronal frequency-selective fat-suppressed intermediate-weighted FSE sequence, a sagittal intermediate-weighted FSE sequence, and a sagittal frequency-selective fat-suppressed T2-weighted FSE sequence. A section thickness of 3 mm was used. To assure that the slices used for the evaluation of the progression of the OCD were taken through the same part of the OCD, the patient was placed in a standardized position and wore a knee splint for reproducible alignment of the leg. Grading and progression of the OCD was determined according to Hughes et al. 7 This classification distinguishes 4 stages, respectively, grades of an OCD. A grade I lesion means a stable lesion with signal intensity change of the subchondral bone and intact cartilage. Grade II lesions additionally show an in situ bone fragmentation. Grade III lesions are characterized by an in situ bone fragmentation and signal changes of the cartilage. Both grades are also classified as stable lesions. Grade IV lesions are subdivided in IVa and IVb lesions and are defined as unstable. Grade IVa lesions show bone fragmentation and a cartilage tear. In grade IVb lesions the osteochondral fragment is displaced from the subchondral bone (loose bodies) with subchondral defects and articular cartilage loss ( Fig. 1 ). Imaging evaluation with OCD classification was performed in a blinded manner by 2 independent orthopedic surgeons.
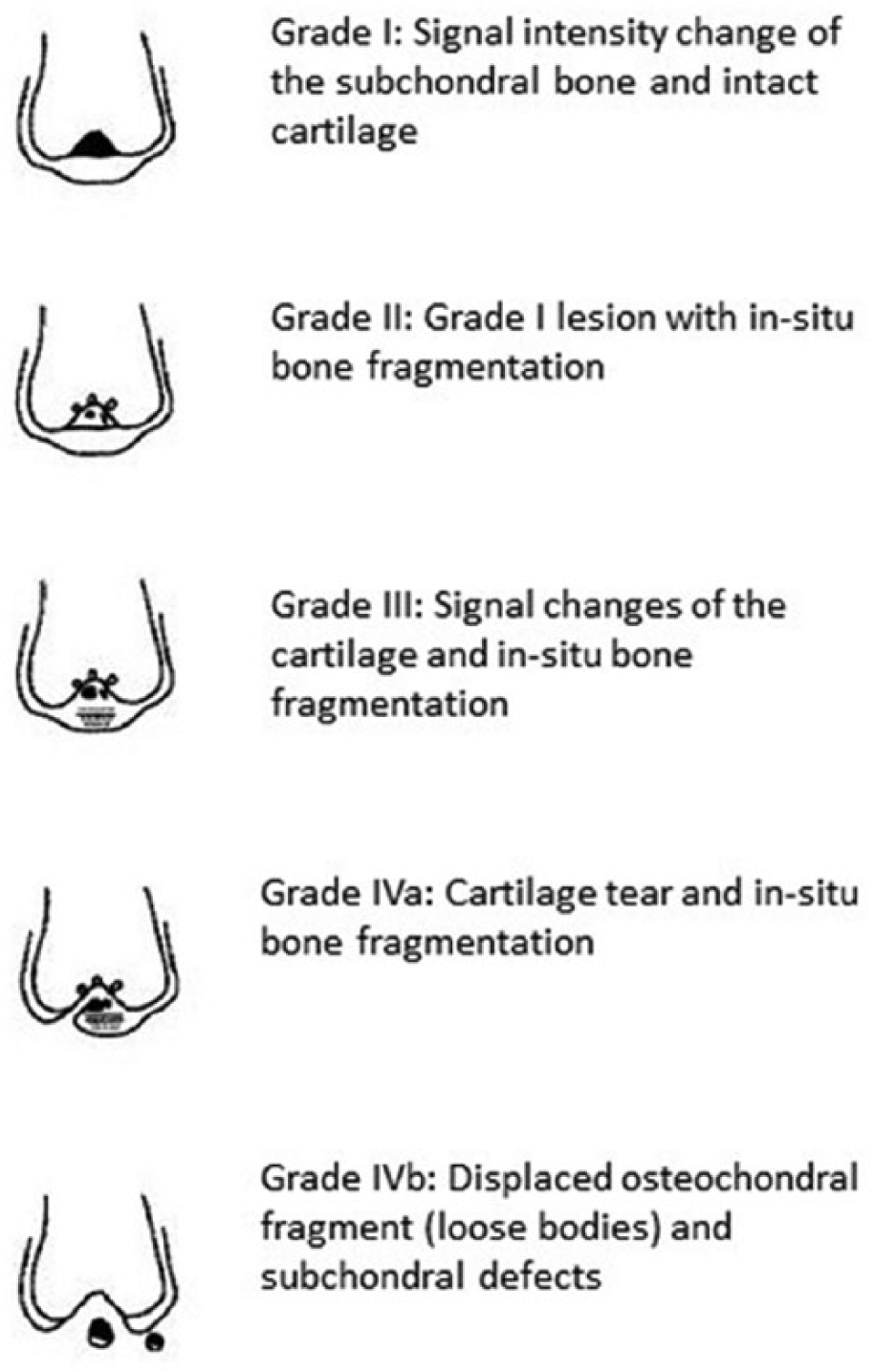
MRI classification of OCD of the knee according to Hughes et al. 7
Arthroscopic Intervention
Standard anteromedial and anterolateral portals were used to evaluate the MRI-confirmed OCD and for the stabilization of the anterior horn of the meniscus. The evaluation of the OCD was performed using a probe to determine the stability and size of the OCD. It was graded according to the arthroscopic classification of Guhl. 11 Grade I, respectively, stage I lesions are characterized by intact cartilage but partially soft surface. A grade II lesion means early separation with interruption of the cartilage. Grade III lesions are partially detached lesions, and grade IV lesions are defined by craters with loose bodies. All lesions of this study were noted to be stable, and no drilling, debridement, or direct treatment of the OCD was carried out. The meniscus in all cases in this series was found to have increased laxity at its peripheral edge with a pathologic amount of free movement occurring when it was probed under direct vision in a 90° flexed knee. This was determined in comparison with the rest of the meniscus and the ipsilateral medial or lateral meniscus. As previously described by Camathias et al., 10 increased mobility of more than 5 mm was considered to indicate instability. This instability materializes in a hypermobile anterior horn that impinges between the femur and tibia while the rest of the meniscus is stable. This instability was then stabilized with direct suturing of the meniscus to the capsule using an outside-in technique with PDS I (Ethicon, Somerville, NJ).10,12 The meniscus was fixed with 2 sutures in all patients and the sutures were orientated in a vertical direction to achieve maximal fixation to the anterior capsule. The first suture was placed at the intercondylar edge of the anterior horn and the gap between the sutures was at least 5 mm not exceeding 10 mm. The authors coined this procedure a meniscopexy.
Postoperative Rehabilitation and Follow-up Examination
Postoperatively, active and passive mobilization was initiated immediately under physiotherapy guidance. All patients were allowed partial weight-bearing with 20 kg and restricted range of motion from 0° up to a flexion of 60° using a hinged brace (Collamed, Medi GmbH & Co. KG, Bayreuth, Germany) for 6 weeks postoperative. Two weeks after surgery full weight-bearing was permitted in full extension. The patients were advised to avoid physical activities, such as running or jumping, for at least 3 months after surgery. Ice packs and medication with nonsteroidal anti-inflammatory drugs were allowed for postoperative pain.
Follow-up examinations were performed 6 and 12 months postoperative. Before treatment and at 12-month follow-up, knee function was evaluated by the Lysholm score.
Results
Four women and 6 men with a mean age of 20.6 ± 1.9 years were included in this study. Mean symptom duration, from the beginning of symptoms to enrolment in the study, was 7.9 ± 1.2 months.
Arthroscopic Findings
In 80% of the patients the OCD was found at the medial femoral condyle. Twenty percent showed an OCD at the lateral femoral condyle. Twenty percent of the patients had an advanced OCD lesion grade III according to Guhl. Grade I and grade II lesions were found in 40% of the patients each. None of the patients showed an instable grade IV lesion or loose bodies. In all patients, instability of the anterior horn of the meniscus could be detected during arthroscopic surgery. Consequently, in all patients arthroscopic meniscopexy was performed.
MRI Findings
Seven of 10 patients (70%) showed a grade III or IVa OCD lesion according to Hughes in the MRI preoperative. Thirty percent of the patients had a grade II OCD lesion. At final follow-up (12 months after surgery), an improvement of the OCD could be demonstrated in 10 of 10 patients (100%) within the MRI. Moreover, 8 of 10 patients (80%) showed an entirely healed OCD with a completely intact osteochondral surface (grade 0 according to Hughes) 12 months after arthroscopic treatment. In only 2 patients (20%) residual signs of the OCD (grade I according to Hughes) could be visualized within the MRI at the final follow-up.
Clinical Findings
Average Lysholm score before surgical treatment was 48.1 ± 14.12. Average Lysholm score 12 months after arthroscopic meniscopexy was found to be 97.5 ± 3.1. In one patient (Patient no. 6), the Lysholm score increased distinctly from 26 preoperative to 100 at the final follow-up. No complications were noted during and after surgical treatment for any patient in this study. The detailed data of all patients are listed in Table 1 . Corresponding findings of patient no. 5 and no. 6 in the MRI and in the arthroscopic intervention are displayed in Figure 2 and 3 .
Clinical Characteristics and Radiological Findings.
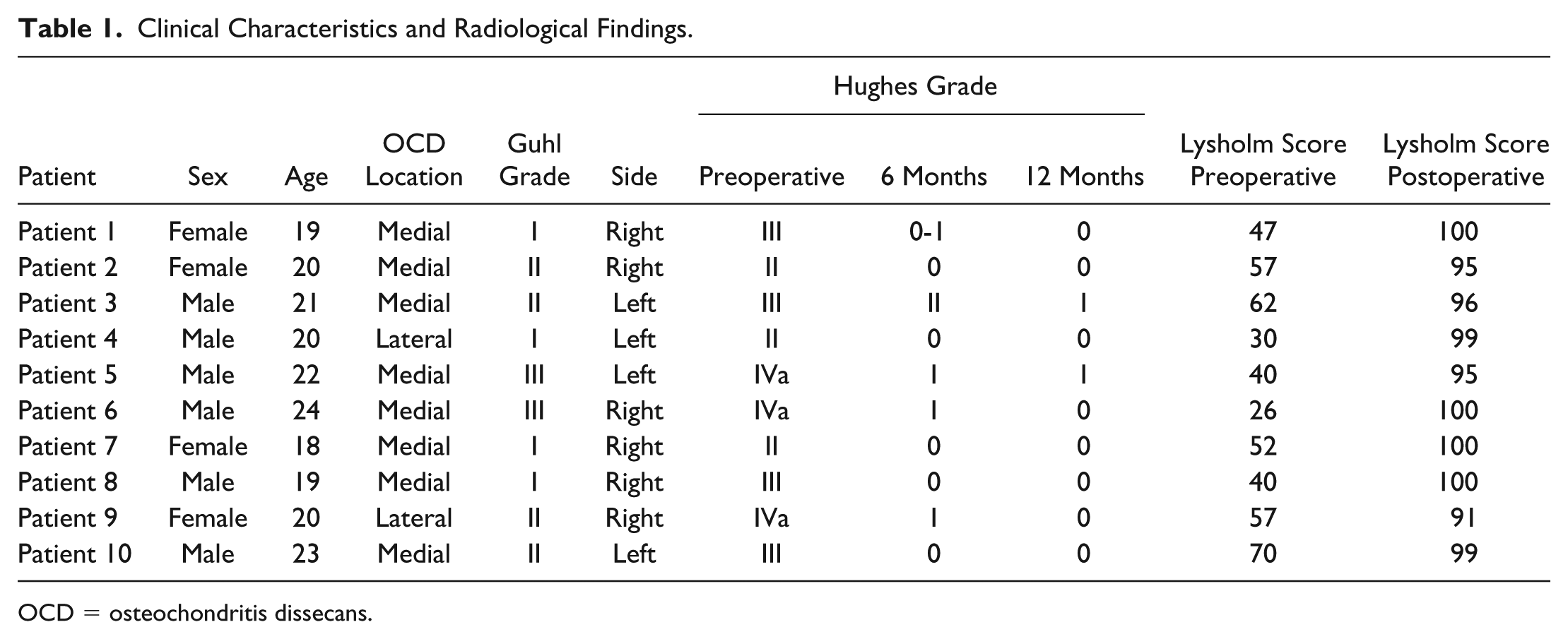
OCD = osteochondritis dissecans.
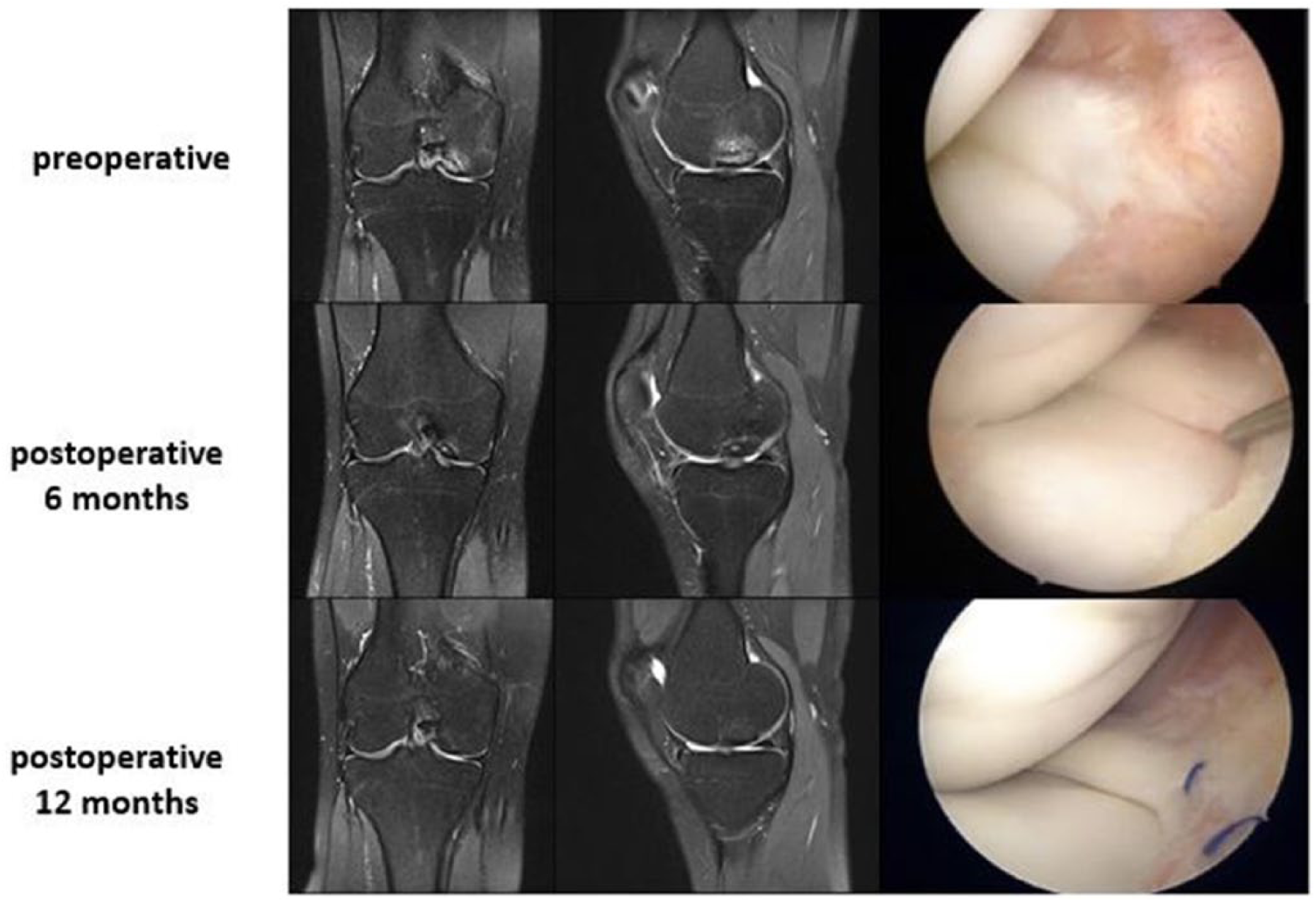
MRI and arthroscopic findings of patient no. 6.

MRI findings of patient no. 5 preoperative and 12 months postoperative.
Discussion
This study demonstrates that arthroscopic anterior meniscopexy may lead to a sufficient healing of a nontraumatic OCD in adults and underlines the clinical concept of a meniscal impingement as a cause of a nontraumatic OCD.
Despite the increase in research efforts, the etiology of and risk factors for a nontraumatic OCD remain unclear.4,6,13 Genetic predisposition, repetitive microtrauma, or vascular compromise has been attributed with playing a key role in the genesis of an OCD.9,14 However, an accepted treatment regime does not exist in the literature.1,2,4,10 A much-noticed clinical study, focusing on adolescents, showed very good outcome results after conservative treatment and clearly indicated that even high-grade OCDs (grade II-III according to Hughes) without dislocation have a tendency to heal spontaneously without specific treatment to either the OCD or other knee structures like the meniscus. 7 These results confirmed the hypothesis that the development of an OCD is not linked to a specific anatomic structure. However, in recent studies an association between a meniscus pathology and the development of an OCD were reported and the importance of meniscal stabilization when treating an OCD were emphasized.15,16 The underlying concept is an impingement of an instable meniscus between the tibia and the femur during extension, which was consistently confirmed in a number of publications since the 1950s.17-19 Consequently, Camathias et al. gave this specific impingement an official term (doorstop phenomena) and introduced in a recent study the stabilization of the anterior horn of the meniscus as a sufficient treatment option in patients with nondisplaced OCDs. 10 However, the treated patients had similar OCD lesions like the patients in the study by Hughes et al. and were also adolescents with open epiphyseal plates.7,10 Therefore, a conclusive proof that nonsurgical treatment would not have led to the same healing rates was not provided. The question whether meniscal suturing is truly effective in OCD or whether these results might be explained by spontaneous healing in patients with open epiphyseal plates remained unanswered.
In this context, the present study adds new information to this topic. For the first time meniscus stabilization was performed in adult patients with an OCD. All lesions (grade II-IVa according to Hughes) showed a steady healing of the OCD in the MRI follow-up examinations with consequent regression of clinical symptoms. Thus, these results provide evidence for the first time that indeed meniscopexy is of value in the treatment of an OCD because spontaneous healing of an OCD is very unlikely in adult patients with closed epiphyseal plates. The hypothesis that meniscal instability, specifically a hypermobile anterior horn that impinges between the femur and tibia, might be a decisive factor in the origin of OCD is confirmed. Consequently, the stabilization of the meniscus can eliminate this offensive mechanism and allow subsequent healing of the lesion. That means a simple suturing technique for an unstable meniscus could act as a first-line treatment for OCD in adult patients. In the past, most surgical treatment methods have targeted the OCD itself. 20 In the future, when a surgeon is choosing between different surgical techniques, meniscopexy as a minimally invasive soft-tissue procedure with fewer complications and good healing prognosis in patients with OCD should be considered.
Obviously, this retrospective study has some limitations. Most important, the question arises how many OCD cases are attributable to meniscal instability rather than other causes. The diagnosis of hypermobility of the meniscus is a rather subjective assessment. However, there was a treatment effect on both clinical and radiographic healing in conjunction with prior biomechanical data. As mentioned above in adult patients the epiphyseal plate is closed, and a spontaneous healing of the OCD is unlikely. Besides, all patients failed a 6-month course of conservative treatment, including partial weight-bearing before arthroscopic treatment.
Furthermore, the size of our study is limited and there is no control group, which received continued conservative and/or other surgical treatment. Despite these limitations, this is, to our knowledge, the first case series study that evaluates arthroscopic meniscopexy as a treatment concept of OCD in adult patients. This offers new conclusions and a novel, minimal invasive first-line therapy in the treatment of OCD that might actually change the clinical practice.
Conclusion
Arthroscopic meniscopexy can lead to sufficient healing of a nontraumatic OCD in adult patients caused by meniscal instability.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethical and institutional boards of the Hessing Stiftung Augsburg, Germany, have approved this study (ID: 17/0106).
Informed Consent
Written informed consent was obtained from all subjects before the study.