
Abstract
Objective
The purpose of this study was to assess potential correlations between the mental component summary of the Short Form–12 (SF-12 MCS), patient characteristics or lesion morphology, and preoperative self-assessed pain and function scores in patients undergoing autologous chondrocyte implantation (ACI).
Design
A total of 290 patients underwent ACI for symptomatic cartilage lesions in the knee. One hundred and seventy-eight patients were included in this study as they completed preoperative SF-12, Knee injury and Osteoarthritis Outcome Score (KOOS), Tegner, Lysholm, and International Knee Documentation Committee (IKDC) scores. Age, sex, smoker status, body mass index, Worker’s Compensation, previous surgeries, concomitant surgeries, number of defects, lesion location in the patella, and total defect size were recorded for each patient. Pearson’s correlation and multivariate regression models were used to distinguish associations between these factors and preoperative knee scores.
Results
The SF-12 MCS showed the strongest bivariate correlation with all KOOS subgroups (P < 0.001) (except KOOS Symptom; P = 0.557), Tegner (P = 0.005), Lysholm (P < 0.001), and IKDC scores (P < 0.001). In the multivariate regression models, the SF-12 MCS showed the strongest association with all KOOS subgroups (P < 0.001) (except KOOS Symptom; P = 0.91), Lysholm (P = 0.001), Tegner (P = 0.017), and IKDC (P < 0.001).
Conclusion
In patients with symptomatic cartilage defects of the knee, preoperative patient mental health has a strong association with self-assessed pain and functional knee scores. Further studies are needed to determine if preoperative mental health management can improve preoperative symptoms and postoperative outcomes.
Keywords
Introduction
Autologous chondrocyte implantation (ACI) has been in clinical use in the United States since 1997 and provides good clinical outcomes in more than 70% to 80% of patients treated for focal cartilage defects of the knee joint.1-6 However, factors such as age, female gender, previous surgeries of the index knee, including microfracture, Worker’s Compensation (WC) status, defect number, location and size, and periosteum patch use have been associated with less favorable results.6-10 Patient-reported outcome measures have increasingly been incorporated as evaluation tools in pre- and postoperative assessments in orthopedic practice. Given the shift to self-assessed questionnaires, it is important to distinguish how psychosocial factors can influence patient-perceived and -reported pain and functional scores. Mental health issues such as anxiety and depression have been shown to contribute to knee pain in patients with osteoarthritis.11-14 Preoperative psychological factors have been associated with pre- and postoperative pain, satisfaction and clinical outcomes across orthopedic specialties such as spine,15-18 trauma,19,20 anterior cruciate ligament reconstruction,21-23 hand and upper extremity,24-28 and arthroplasty.29-34
Commonly used patient-reported evaluation tools in patients with cartilage lesions of the knee include the Knee injury and Osteoarthritis Outcome Score (KOOS) to assess pain, symptoms, activities of daily living (ADL), sport/recreation, and quality of life (QOL); the Lysholm score evaluating pain, symptoms, and function; the Tegner activity scale measuring patient activity level; and the International Knee Documentation Committee Subjective Knee Evaluation Form (IKDC) assessing symptoms, function, and sports activity. 35 To our knowledge, the specific relationships of psychological factors, patient-reported outcomes, objective clinical measures, and patient characteristics have not been reported for patients with symptomatic cartilage defects of the knee.
Considering the uncertain association of mental health with self-reported knee outcome scores, we sought to examine factors with potential influence on preoperative KOOS subgroups, Lysholm, Tegner, and IKDC scores for patients with symptomatic cartilage defects in the knee. Our hypothesis was that mental component summary of the Short Form–12 (SF-12 MCS) would show a stronger association with preoperative knee pain and function scores than other patient-specific demographic factors or cartilage defect morphology.
Materials and Method
Our institution prospectively collects data for all cartilage repair patients. Patients indicated for cartilage repair with ACI for focal cartilage defects in the knee by a single surgeon between March 2007 and July 2017 were enrolled for this study. Our institutional review board approved the study prior to initiation. Patients with incomplete preoperative self-assessments as described below, incomplete patient demographic data, or unreported defect morphology were excluded from this study.
Each patient enrolled in this study completed preoperative SF-12, KOOS, Lysholm, Tegner, and IKDC evaluation forms. The SF-12, which is derived from the SF-36, consists of a 12-item questionnaire measuring specific factors of general health-related QOL divided into the physical component summary (PCS) and the MCS. The mean score in the general population is 50 with a standard deviation of 10. Higher scores demonstrate better health-related QOL.36,37 The KOOS score was developed based on literature review, expert panel, and a pilot study evaluating 2 self-administered questionnaires in 75 patients after meniscus surgery 20 years prior. It holds 5 subscales (Pain, Symptom, ADL, Sport/Recreation, and QOL) that are scored individually from 0 (extreme knee problems) to 100 (no knee problems). 38 Originally designed for ligamentous injuries, the Lysholm score has an overall score of 0 to 100 and covers 8 domains, including limp, locking, pain, stair climbing, support, instability, swelling, and squatting and has also been shown to have predictive value for clinical outcome after ACI.10,39,40 The Tegner activity scale scores patient’s activity level on a numerical scale from 0 to 10 depending on their sports level. Patients participating in competitive sports are considered to have a Tegner score of 10, whereas recreational sports level is considered an activity level of 6, and disability or no sports participation an activity level of 0.39,41 The IKDC was developed by an international committee of knee experts to measure knee-specific symptoms, function, and sports activity with a maximum score of 100 (no limitation with daily activities and absence of symptoms). It is based on 18 items covering 3 domains: (1) symptoms (including pain, stiffness, swelling, locking/catching, and giving way), (2) sports and daily activities, and (3) current knee function and knee function prior to knee injury. 42
Patient’s age at the time of surgery, body mass index (BMI), sex, smoking status, WC status, and whether the patient had concomitant surgeries such as osteotomy or ligamentous repair/reconstruction and meniscus allograft transplantation (MAT), and/or multiple previous surgeries on the index knee were recorded. Cartilage defect morphology, including the size, number, and the occurrence of a patella lesion were collected from surgical notes.
Descriptive statistics were calculated to determine the sociodemographic and clinical characteristics of patients. Bivariate correlations were assessed by Pearson’s correlation coefficients (r). Categorical variables were coded as dummy variables for multivariate linear regression models (i.e., for sex, 0 represented male and 1 represented female). Models included patient age, sex, BMI, concomitant surgeries, multiple previous surgeries, WC status, smoking status, SF-12 MCS scores, defect number, defect size, and occurrence of a patella lesion. Patient-reported scores, including KOOS subgroups, Lysholm, Tegner, and IKDC scores were dependent variables. Regression coefficients are reported. All statistical analyses were performed in SPSS for Mac (version 23.0, IBM Corp, Armonk, NY). Significance was set at P < 0.05.
Results
The senior author (AHG) treated a total of 290 patients with ACI for focal symptomatic cartilage lesions within the knee joint during the study period. Of these patients, 112 patients were excluded, thus 178 patients (61.4%) were enrolled in this study. Of the included patients, 97 (54.5%) were female, 12 (6.7%) were active smokers, 12 (6.7%) were WC, 69 (38.8%) had multiple previous operations on their index knee, 124 (69.7%) underwent concomitant procedures, and 114 (64%) had at least 1 cartilage lesion on the patella. Concomitant procedures included 21 high tibial osteotomies, 99 tibial tubercle osteotomies, 9 distal femoral osteotomies, 14 MAT, 5 anterior cruciate ligament reconstructions, and 1 medial patellofemoral ligament reconstruction. The number of lesions ranged from 1 to 5 defects with 53.4% of patients presenting with 1 defect, 28.7% with 2 defects, 12.9% with 3 defects, 3.4% with 4 defects, and 1.1% with 5 defects across the knee joint. The mean age was 31.4 years (SD = 9.4; range = 14-56 years) with an average BMI of 26.5 kg/m2 (SD = 4.2; range = 18-38.2 kg/m2). The combined size of all assessed cartilage defects in a patient averaged 713.5 mm2 (SD = 482.8; range = 96-2753 mm2). The outcomes for all patient-reported knee-specific surveys are presented in Table 1 .
Patient-Reported Preoperative Outcome Measures.
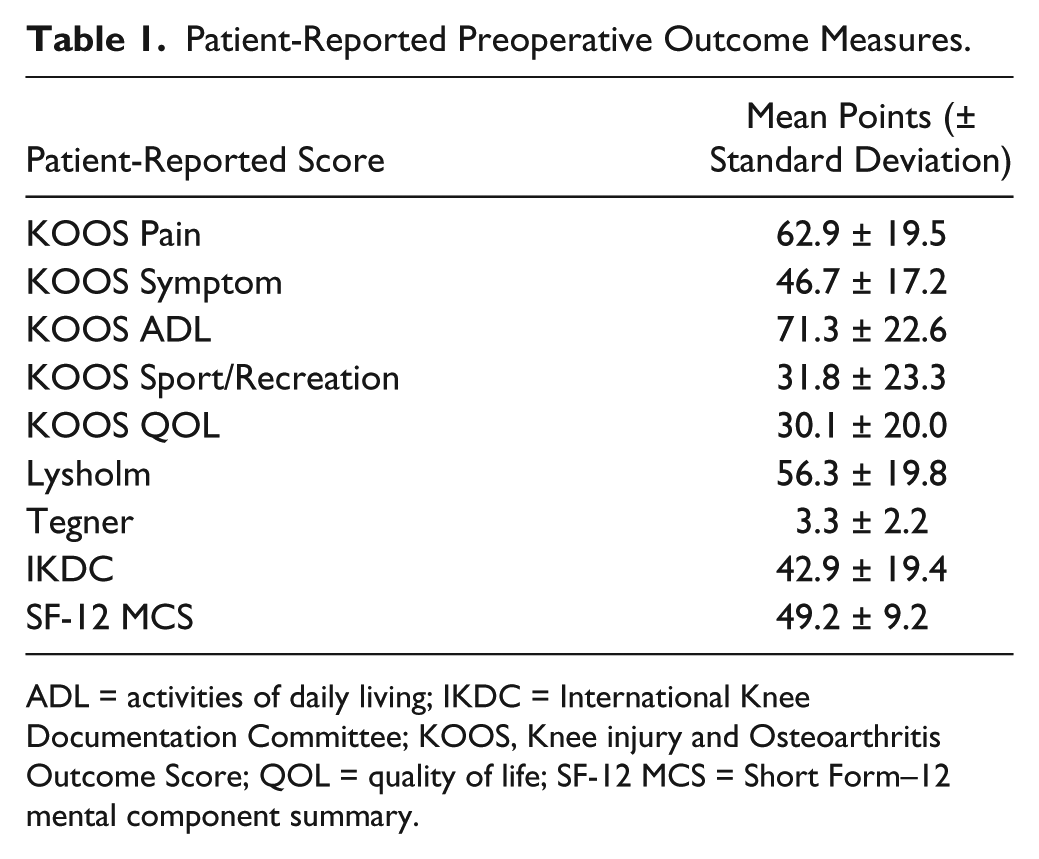
ADL = activities of daily living; IKDC = International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL = quality of life; SF-12 MCS = Short Form–12 mental component summary.
The SF-12 MCS showed the strongest Pearson’s correlation among all variables with each patient-reported outcome measures except the KOOS Symptom subscale ( Table 2 ).
Significant Bivariate Pearson’s Correlation of Preoperative Patient Factors with Knee-Specific Outcome Scores.
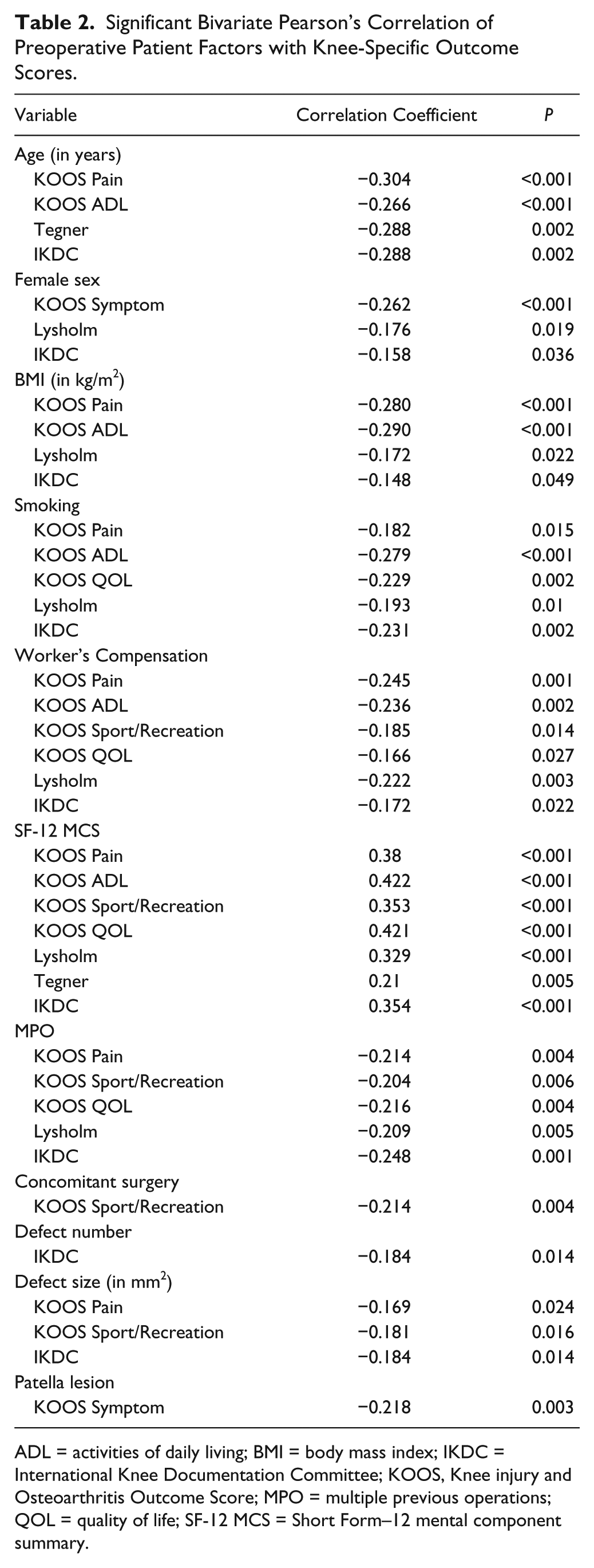
ADL = activities of daily living; BMI = body mass index; IKDC = International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MPO = multiple previous operations; QOL = quality of life; SF-12 MCS = Short Form–12 mental component summary.
In the multivariate linear regression models, the SF-12 MCS had the strongest association with every patient-reported outcome but the KOOS Symptom score (all P < 0.02 and P = 0.91, respectively) ( Table 3 ). Multiple previous surgeries only correlated with KOOS QOL (P = 0.042), whereas concomitant procedures were associated with the KOOS Sport/Recreation subscale (P = 0.045). With regard to defect morphology (location, size, number), only defect size was associated with preoperative KOOS Pain (P = 0.017).
Multivariate Regression of the Effect of Patient Characteristics, Defect Morphology, and Self-Assessed Mental Health on Preoperative Knee-Specific Outcome Measures.

ADL = activities of daily living; BMI = body mass index; IKDC = International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MPO = multiple previous operations; QOL = quality of life; SF-12 MCS = Short Form–12 mental component summary.
Significant association with P < 0.05.
Discussion
The purpose of this study was to evaluate the relationship between patient-reported preoperative knee pain and function scores, and factors, including mental health scores, age, BMI, smoking status, WC status, concomitant procedures, prior knee surgeries, and cartilage defect morphology. We found that the patient’s mental health as assessed by the SF-12 MCS had the strongest association with all outcome measures, except the KOOS symptom score. While the KOOS symptoms score was not associated with the patient’s SF-12 MCS, this score may be considered the most objective of the KOOS subscales, as the questions ascertain to the patient’s perception of swelling, grinding or clicking, catching in the joint, the ability to fully extend or flex the knee, and the severity of stiffness in the morning and later in the day. To our knowledge, this is the first study to report this strong association of mental health with preoperative functional and pain scores in patients indicated for the treatment of symptomatic cartilage defects in the knee. Other patient factors, including age, female sex, BMI, and smoking status did show associations with some of our preoperative scores ( Table 3 ). Thus, it may be of benefit to address modifiable factors such as BMI and smoking prior to surgery, as previous studies have shown an association with worse postoperative outcomes.10,43-45 Among defect morphology, only defect size correlated with preoperative pain.
As patient-reported outcome measures are becoming more commonly used to assess treatment response, it is important to understand how psychosocial and other patient factors may affect these scores. Numerous studies across various orthopedic subspecialties have demonstrated an association between mental health, and pre- and postoperative pain, satisfaction, and outcomes.15-31,33,34,38 While a formal psychological interview is the standard of care to assess a patient’s mental health, this type of evaluation is not feasible in the typical outpatient orthopedic clinic.
In this study, the SF-12 MCS was used to assess patient’s preoperative mental health. This is a validated assessment tool that has been used to evaluate orthopedic patients with a variety of conditions. Other authors have proposed to incorporate the SF-36 assessment in both the pre- and postoperative review of all patients undergoing ACI, because knee function scores alone do not capture all of the benefits to a patient’s global health following surgery. 46 Another study used the preoperative SF-36 MCS score, along with duration of symptoms and graft size to predict postoperative MRI scores and functional outcomes at 5-year follow-up after ACI. 47 In our study, the SF-12 was chosen to lower the respondent burden for the patient since the SF-36 MCS can also be obtained from the SF-12. 48 This study further demonstrates the importance of evaluating a patient’s mental health status as part of the routine preoperative assessment to better understand the patient’s self-reported pain and function scores prior to ACI. While we did not assess the effect on patient’s postoperative outcomes, understanding the preoperative effect of mental status on preoperative pain and function may help the clinician provide more accurate prognostic information to a given patient.
Commonly used measures of cartilage defect severity include the size, location, and number of defects within the knee. However, the multiple regression analysis in our study revealed that defect size was only correlated with preoperative KOOS pain. The observed correlation of defect size and preoperative KOOS pain could be supported by a previous laboratory study that showed that insulin-like growth factor–I (IGF-I) was expressed in knees with circumscribed cartilage lesions in a size dependent manner and these IGF-I levels correlated with patient-report pain scale. 49 On the other hand, the number of defects and presence of a patella lesion did not correlate with any of patient-assessed measures.
In our multivariate model, the SF-12 MCS was the only significant predictor that would lead to a clinically important change in the patient reported knee scores tested. Based on the minimum clinically important difference for these scores, a change of 14 to 22 points in the MCS would lead to clinically important changes in the KOOS-pain, Lysholm, Tegner, and IKDC scores. Interestingly, while preoperative functional scores have been positively correlated with outcome in patients undergoing arthroplasty, 50 for ACI a minimum threshold of preoperative self-reported scores has been established below which favorable outcomes are less likely. 51 Therefore, our findings suggesting a strong correlation between a patient’s mental health status and preoperative knee scores, opens the possibility of establishing mental health as the third preoperatively modifiable risk factor, besides BMI and smoking status, that could influence postoperative outcomes.
However, specific studies are needed to further investigate the association of pre- and postoperative scores in patients undergoing cartilage repair, specifically with attention to how improving preoperative scores through mental health interventions could impact postoperative outcomes.
Our study has limitations. This was a cross-sectional analysis of prospectively collected data. Of the eligible 290 patients, only the 178 with complete data sets were enrolled in the study, raising the possibility of selection bias. Given this limitation, the cohort may not have been fully representative of the entire patient population. We also did not specifically analyze for medical comorbidities, however, any major medical comorbidities represent a contraindication for cartilage repair; and therefore, our study cohort was younger and healthier than, for example, a cohort of arthroplasty patients. Furthermore, because of the nature of our practice as a tertiary referral center for cartilage repair, patients in this study had relatively large cartilage defects. Thus, it cannot be excluded that the observed association might not apply to patients with smaller defects. Finally, this cross-sectional study cannot establish causality between mental status and preoperative pain and function (i.e., did pain lower the mental health scores, or did baseline lower mental health scores lead to higher levels of perceived pain and disability). Hence, a prospective longitudinal study is needed to determine whether or not there is any bidirectional association between mental health and preoperative pain and function.
In conclusion, other studies have suggested a negative correlation of mental health and surgical outcomes. Our study suggests that decreased mental health scores are associated with reports of worse preoperative symptoms. In patients with symptomatic cartilage defects of the knee, the patient’s mental health as assessed by the SF-12 MCS had a stronger association with self-assessed pain and function scores than other patient factors or defect morphology. Consequently, the treating surgeon should be aware of, and take into consideration, any prospective patient’s mental health to help guide both surgical decision making and discussion of expected benefits. Further studies are needed to determine if referral for mental health services can improve perception of pain and function preoperatively, and possibly secondarily improve outcomes after surgical intervention.
Footnotes
Authors’ Note
The study was performed at the Cartilage Repair Center and Center for Regenerative Medicine, Brigham and Women’s Hospital, Harvard Medical School, Harvard University, Boston, Massachusetts, USA.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Partners Human Research Commitee (2017P002136/PHS).
Informed Consent
Waiver of Informed Consent from IRB.
Trial Registration
Not applicable.