
Abstract
Objectives
To evaluate the main symptoms of knee osteoarthritis (OA) and tissue structure changes after a single dose bone marrow–derived mononuclear cell (BM MNC) intra articular injection. Case series study. Patients with knee OA Kellgren Lawrence (K-L) grade II and III received 1 injection of BM MNC. The clinical results were analyzed with the Knee injury and Osteoarthritis Outcome Score (KOOS) and Knee Society Score (KSS) before, 3, 6, and 12 months after injection. Radiological evaluation was performed with a calibrated x-ray and the magnetic resonance (MR) imaging before and 6 to 7 months postinjection.
Results
A total of 34 knees were treated with BM MNC injections. Mean (±SD) age of patient group was 53.96 ± 14.15 years; there were 16 males, 16 females, KL grade II, 16; KL grade III, 18. The average injected count of BM MNCs was 45.56 ± 34.94 × 106 cells. At the endpoint of 12 months 65% of patients still had minimal perceptible clinical improvement of the KOOS total score. The mean improvement of KOOS total score was +15.3 and of the KSS knee score was +21.45 and the function subscale +27.08 (P < 0.05) points. The Whole Organ Magnetic Resonance Imaging Score (WORMS) improved from 44.31 to 42.93 points (P < 0.05). No adverse effects after the BM-MNC injection were observed.
Conclusions
The single dose BM MNC partially reduces clinical signs of the knee osteoarthritis stage II/III and in some cases, decreases degenerative changes in the joint building tissue over 12-month period.
Keywords
Introduction
Treatment of the early stages of the knee joint osteoarthritis continues to present its challenges in orthopedic practice. An ideal therapy should target both inflammatory and tissue degeneration processes in the joint building tissue, combination of which characterizes the development of osteoarthritis. Routinely orally used nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroid injections successfully reduce inflammation; however, an influence on the degenerative process to the joint structures, such as cartilage, synovial membrane, and metaphyseal bone has not been demonstrated. Additionally, the long-term use of the NSAID therapy is commonly associated with gastrointestinal, hepatic, renal, and/or cardiac side effects among others. 1
Alternatives include viscosupplementation—a treatment using hyaluronic acid (HA). It provides joint lubrication and shock absorbency and acts as a backbone for the proteoglycans of the extracellular matrix. 2 However, evidences gathered from clinical trials does not clearly support any positive effects the HA may have on slowing down the progression of OA, and the guidelines for clinical use of the HA are not unanimous, they advise cautious use of this treatment.3,4
It has been suggested that in platelet-rich plasma (PRP) platelet α-granules containing growth factors and bioactive molecules injected in a knee joint could signal the beginning of regeneration process in the host tissue cells. 5 However, one of the downsides is a limited continuance of the improvement (approximately less than a year) which does not yield a regenerative effect on articular tissues, hence why the PRP cannot be unequivocally considered as superior to the HA.5,6
The problem of the tissue renewal could be resolved by application of stem cells, which represent naive cells differentiating to specific tissue lineages during development. These cells reside within tissue compartments with a purpose to replace cell populations over the lifetime. In the 1970s, Freidenstein 7 discovered that the cells extracted from the red bone marrow in vitro demonstrated properties of adherence, colony formation, and osteogenic lineage differentiation. Later in the 1990s, Caplan 8 named these cells “mesenchymal stem cells” (MSCs) and proposed that they would have a differentiation capacity for all mesenchymal tissues. So far, this theory has not been sufficiently proven and the concept of the bone marrow–derived cells as “stem” cells remains open to debate. Later on, Caplan 9 revised the concept of multipotent stem cells and proposed that pericytes—the cells closely associated with capillaries and microvessels—are the main source of multipotent stem cells. The International Society of Cell Therapy defined the “MSCs” as a plastic-adherent, capable of trilineage differentiation and possessing cell surface antigens CD105, CD73, and CD90 with a lack of CD45, CD34, CD14, CD11b, CD79α, CD19, or HLA-DR. 10
Attractiveness of the ‘MSCs’ in cartilage repair is found in their immunomodulatory capacity and production of trophic factors. The “MSCs” are able to suppress immune cell proliferation and cytokine release. 11 Despite the theoretical controversies, clinical studies investigating use of the MSCs to treat cartilage injury and OA have demonstrated encouraging clinical outcomes, as well as the magnetic resonance imaging (MRI) and histological findings consistent with restoration of hyaline-like cartilage.12-14 Renewal of the joint building tissues and slowing down of degenerative processes caused by OA has been reported.15,16
The MSC therapy seems to be a simple, safe, and minimally invasive approach to target cartilage lesions and early stages of OA. Despite the growing number of studies on these biological treatments the evidence on their effectiveness in orthopedic practice is still limited. A uniform analysis of clinical benefits of the BMSC-based therapy in larger patient groups is still missing.
This study had the following aims:
To observe the presence of adverse events associated with the applied therapy.
To find out the clinical effectiveness of the knee OA Kellgren- Lawrence (K-L) stage II-III affected joints treated by the single intra-articular injection of the bone marrow–derived mononuclear cells (BM MNC) over the period of 12 months.
To evaluate structural changes of the joint building tissue over the 12-month follow-up period using x-ray and MRI.
Materials and Methods
Patient Enrolment and Study Design
This is a prospective case series study done in the Latvian State Hospital of Traumatology and Orthopedics and the Cell Transplantation Centre of the Pauls Stradins Clinical University hospital during the period of 2013-2016.
The inclusion criteria are the following: degenerative osteoarthritis of the knee, K-L grade II-III, at least 6 months of persisting pain, and some of OA symptoms. The exclusion criteria are the following: age >75 years, oncologic diseases, severe renal, pulmonary or hepatic impairment, hematologic diseases, including anemia and thrombocytopenia, diabetes mellitus of the first type, severe effusion, contracture or instability and axial deformities more than 10° in the knee joint, septic arthritis or skin disorders, use of corticosteroids and immunosuppressive agents, previous injection in the target knee within 2 months. Before the inclusion, clinical history, physical examination, routine laboratory tests, calibrated X-ray and MRI were performed.
The previous medical history of the enrolled patients was carefully evaluated. The BM MNC injection was performed not prior to 1 month after the surgical intervention in the same knee joint.
The clinical study protocol was approved by the State Central Medical Ethics Committee. All patients provided informed consents for the study according to the Helsinki Declaration, and all patients voluntarily agreed to participate and signed informed consent forms.
Bone Marrow Harvesting and Cell Preparation
Cells used in this study were extracted from the patient’s own red bone marrow. Iliac crest puncture was done under local anesthesia. Totally, up to 45 mL of the bone marrow was aspirated into heparin-treated syringes. The bone marrow aspirate was shipped at room temperature to the central cell-processing laboratory. The bone marrow aspirate was processed manually in a sterile environment according to requirements of the Good Manufacturing Practice standard (GMP). The aspirate was diluted with sterile 0.9% NaCl (1:5), filtrated through 70-µm cell strainer (BD Biosciences), and BM MNCs were isolated and enriched by the density gradient centrifugation by Ficoll-Paque Premium (GE Healthcare Ltd) according to manufacturer’s instructions with minor protocol modifications. Separation of the mononuclear cell fraction was performed at 800 × g for 25 min. The MNCs were washed (centrifugation at 600 × g) 3 times with 45 mL 0.9% NaCl containing 10 U/mL heparin and resuspended in the saline with 10,000 U/L heparin. This isolation produced up to 5 cm3 of MNCs suspension, which was sterile packed and released for clinical application. During the gradient centrifugation, plasma factors, red blood cells, and platelets were removed. The cell suspension used for injection contained only mononuclear cell fraction, and no other additional biological substances were added.
Flow cytometry was used to detect the MNCs count and cell viability in the injectate released for application. Samples of the final product were taken and used for the flow cytometric analysis within 2 hours after processing. A stem kit from the Beckman Coulter was used for the cell labelling with CD45-FITC, CD34-PE, 7-AAD, and Stem-Count fluorospheres. Cells were analyzed using FC-500 (Beckman Coulter). The analysis protocol was created manually. The Stem CXP program was used for detection of the MNC, CD34+ cell count, and cell viability. Gating was performed according to the ISHAGE protocol according to the manufacturer’s suggestions. The cell viability was assessed using the 7-AAD method that is included in the ISHAGE protocol. Each measurement contained at least 50,000 events. Maximum number of events was 100,000. Obtained numbers of cells/µL were calculated for the total number of the MNCs and the CD34+ cells within the transplantation material. Measurements with less than 50,000 events were excluded from the cell count analysis.
Follow-up and BM-MNC Injection Procedure
The knee joint puncture was performed using anterolateral approach in the flexed knee without using local anesthesia. 5 to 10 mL of saline was injected to be sure of the correct needle placement in the joint cavity. In case of free drainage of the saline by aspiration, the correct placement in the knee joint cavity was considered. The injection of BM MNC suspension into the knee joint was performed without changing the needle position. After 1 hour of bed rest, patients were discharged home. No restrictions on further activities were given. The short-term use of painkillers during the evaluation period of 12 months was accepted. The patients continued using SYSODOA and doing physical activity at their usual level. At enrolment, the patients were recommended avoiding excessive physical activity and sport exercises exceeding their normal everyday activities and habits. During visits at the time points 1, 3, 6, and 12 months, it was controlled.
Clinical Assessment
The clinical assessment was based on outpatient visits at the 1-, 3-, 6-, and 12-month time points after the injection of BM MNC by the same surgeon who performed injection in the knee joint. Complete history of the changes in OA symptoms and knee joint function, as well as adverse events was obtained and recorded.
Clinical assessment was performed using the Knee Society Score (KSS) and Knee injury and Osteoarthritis Outcome Score (KOOS). KSS scoring system is a version of the knee score modified by Dr John Insall in 1989. The scoring system combines the relatively objective Knee Score that is based on the clinical parameters and the Functional Score based on how the patient perceives his knee functions during specific activities. The maximum Knee Score is 100 points and the maximum Functional Score is 100 points. 17 At the same time points, the patients completed the KOOS. It consists of 5 subscales: Pain, Symptoms, Activities of Daily Living (ADL), Sport and Recreation Function (Sport/Rec), and the knee-related Quality of Life (QOL). The KOOS score of 100 indicates no symptoms, and 0 indicates extreme symptoms. 18
Radiological Assessment
Weightbearing anteroposterior and lateral semiflexed radiographs were obtained before the cell injection procedure and 12 months after. Radiographs were scored according to the K–L classification. Joint space width was measured at 0- and 12-month time point.
The MRI was performed prior to and 6 to 7 months after the BM MNC injection on 30 out of 34 cases. Unfortunately, 4 patients refused to undergo the final MRI due to different reasons. The MRI examinations were performed with a 1.5-T scanner using a dedicated knee coil. All patients were placed in the supine position. The MRI protocol included proton density fat saturation sequence on the sagittal, coronal, and axial planes and proton density fast spin echo sequence on the sagittal and coronal planes.
All X-rays and MRI images were evaluated by 2 musculoskeletal radiologists. The examiners were blinded to all clinical data. The MRI evaluation was performed using the semiquantitative Whole Organ MRI Scoring (WORMS) method. The WORMS score analyzes 14 different features and scores the changes in the following points: articular cartilage integrity (0-6), subarticular bone marrow abnormality (0-3), subarticular cysts (0-3), subarticular bone attrition (0-3), marginal osteophytes (0-7), medial and the lateral meniscal integrity (0-4), anterior and the posterior cruciate ligament integrity (0-1), medial and the lateral collateral ligament integrity (0-1), synovitis/effusion (0-3), intra-articular loose bodies (0-3), and periarticular cysts/bursitis (0-3). A score of 0 points represents normal tissue structure. These features were evaluated in 15 different regions subdivided by anatomical landmarks in the fully extended knee. 19
Statistical Analysis
All data were analyzed using IBM SPSS 22.0. Firstly, data were analyzed for normality using skewness and kurtosis as well as a histogram and a Q-Q plot. If the data were normally distributed, the paired or independent Student t test was done. The KSS, and KOOS subscales between the baseline and follow-up points within each group were analyzed in this manner using the paired t test. A P value <0.05 was considered as statistically significant. The Levene test was used to evaluate homogeneity between the 2 study groups. The independent Student t test was used for comparing the different BMMNC groups. If data were not normally distributed, the Mann-Whitney U test was used.
Results
In this study, 46 patients with knee OA of K-L stages II-III were screened and 32 of them were included. The mean (±SD) age in this group was 53.96 ± 14.15 years; 16 were males and 16 were females. The estimated K-L grade was II for 16 and III for 18 knees. Two of 32 patients received MNC injections in both knee joints.
According to the previous medical history, total knee arthroplasty on the contralateral knee joint had been performed in 10 patients and total hip replacement in 1 patient. Arthroscopy with meniscus resection on the same knee joint had been performed on 11 patients, and in 1 case anterior cruciate ligament replacement had been previously done. Two youngest patients of the cohort had a previous history of patellar dislocations. The incidence of previous surgery done on the knee joint in the patient group treated with the BM MNC was 35%.
No adverse effects after the BM-MNC injection were observed. The patients reported the procedure of the iliac crest puncture as painless, and no complications in donor sites were observed. Pain and swelling in the knee joint caused by the puncture and the BM MNC injection decreased during the first 24 hours in the majority of patients. No additional treatment was applied. Positive response was observed in 97% of knees after the BM MNC injection. At the end of the follow-up, all subscale results had improved comparing to the baseline. The mean KOOS subscales improved accordingly: total score +15 points, the symptoms subscale +9.3, the pain subscale +20.5 points, the activities of daily living subscale +18.4, the sports subscale +18.5, and the quality of life subscale +23.9 points ( Table 1 ).
Results of the KOOS and KSS Scores during the Follow-up Period.
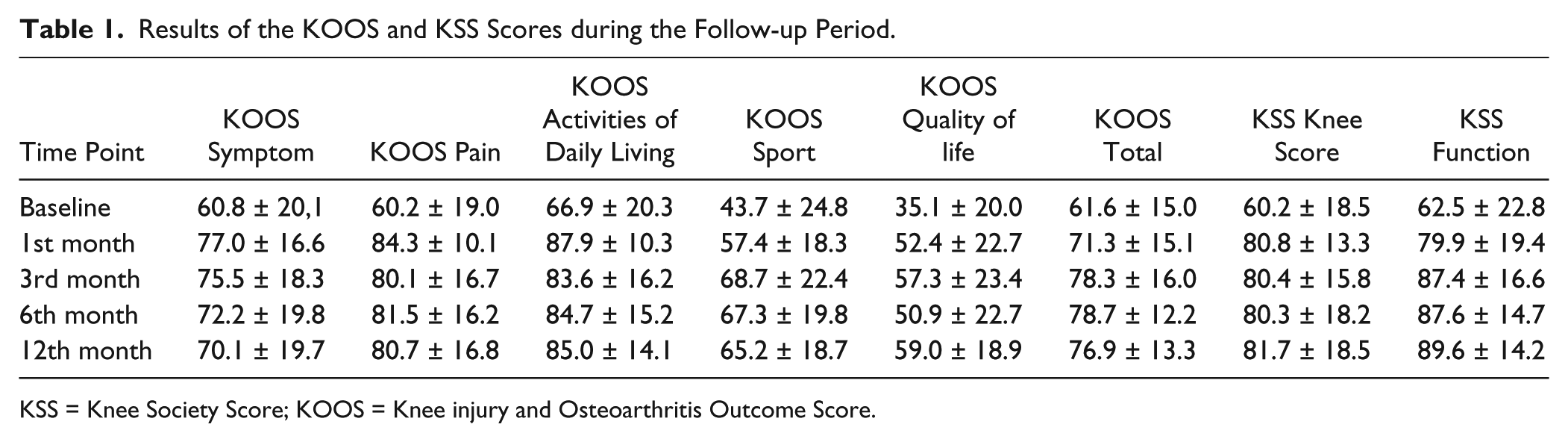
KSS = Knee Society Score; KOOS = Knee injury and Osteoarthritis Outcome Score.
Statistical analysis of the KOOS score results between the baseline and all of follow-up time periods demonstrated statistically significant improvement (P < 0.05) in all subscales except symptoms subscale at the 12-month time point and the sport subscale at 1 month after the BM MNC injection.
During the first months after the BM MNC injection rapid improvement was observed in the majority of cases in the pain, symptoms, and activities of daily living subscales. The results in the sport and the quality of life subscales improved progressively during the 12-month period ( Fig. 1 ).
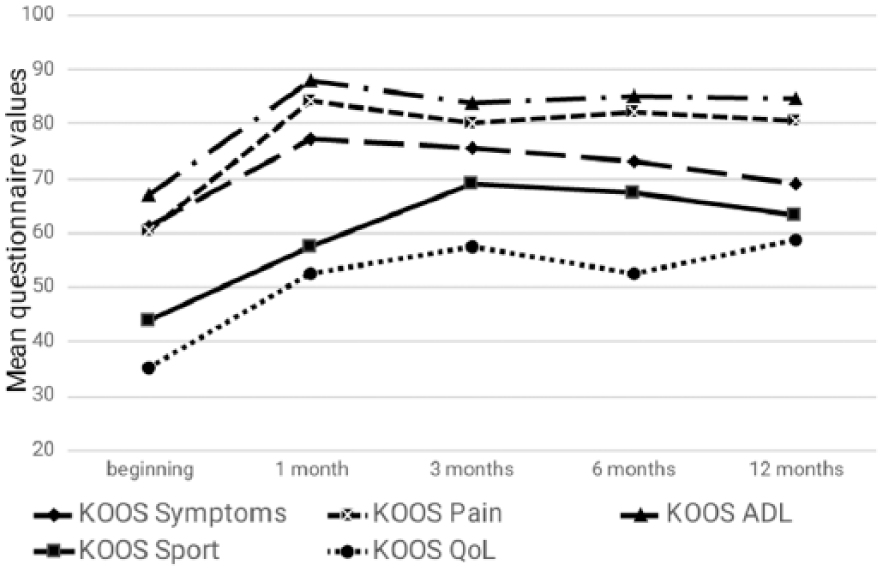
Results of Knee injury and Osteoarthritis Outcome Score (KOOS) score during the 12-month follow-up period.
The clinically relevant changes of the symptoms or minimal perceptible clinical improvement measured with the KOOS score starts from 8- to 10-point difference. 20 At the endpoint of 12 months, 65% of the patients still had improvement for more than 10 points of the KOOS total score. At the 6-month time point, 78.26% of the patients had improvement in the pain subscale for more than 10 points and after 12 months it decreased to 66.67%. However, the share of more than 10-point improvement of the quality of life subscale increased from 65.22% at 6 months to 75% at the 12-month time point ( Fig. 2 ).
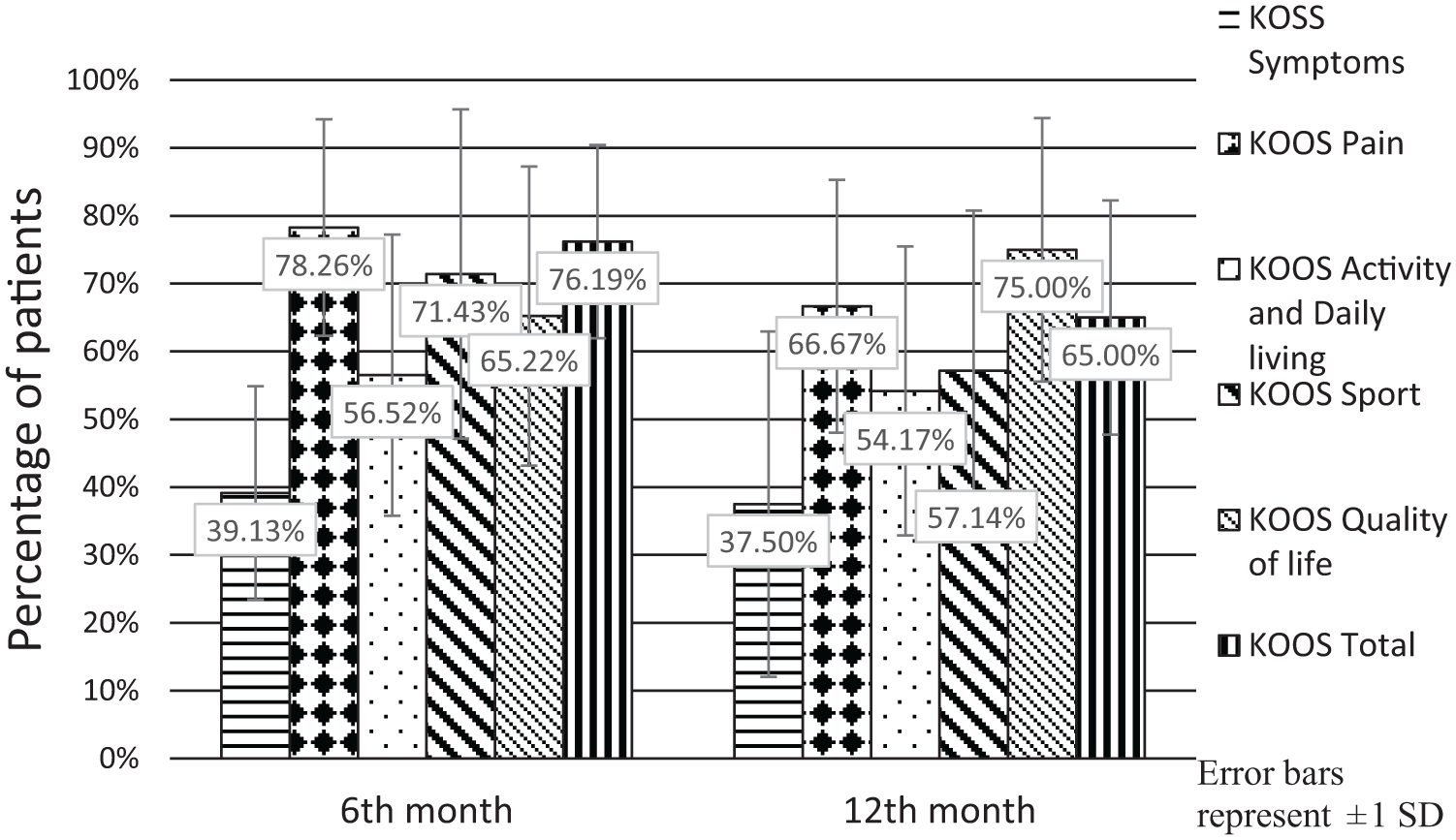
Minimal perceptible clinical improvement of 10 points by Knee injury and Osteoarthritis Outcome Score (KOOS) score.
OA clinical signs measured by the KSS demonstrate the improvement in both the knee score and the subscales of the functional score ( Table 1 ). At the endpoint of 12 months, the mean KSS knee score had +21.45 and the functional score had +27.08 points improvement ( Fig. 3 ).
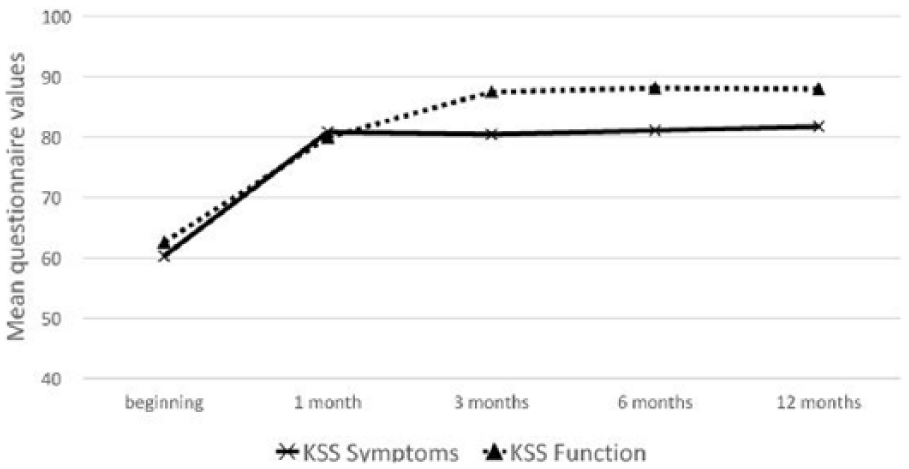
Results of Knee Society Score (KSS) during the 12-month follow-up.
The subscale of the KSS knee score demonstrated a similar pattern as the KOOS score. The KSS knee score containing questions about pain and symptoms demonstrated improvement particularly during the first month ( Fig. 3 ) whereas the function score improved more progressively.
Results of the Radiological Investigation
The x-ray examinations showed no signs of further development of the OA and no changes in the K-L grade 12 months after the BM MNC injection. No unexpected changes in the bone structure or any periosteal reaction were evident. No statistically significant difference regarding joint space width change between beginning and end of study was found.
MRI was evaluated using the WORMS score. The mean score before the injection was 44.31 points, and after 6 months period statistically significant (P< 0.05) improvement to 42.93 points was observed.
We found changes on 3 of WORMS score features: articular cartilage, subarticular bone marrow and synovitis ( Table 2 ). In all other WORMS score features like subarticular cysts, subarticular bone attrition, marginal osteophytes, medial and lateral meniscal integrity, anterior and posterior cruciate ligament integrity, medial and lateral collateral ligament integrity, intraarticular loose bodies, and periarticular cysts/bursitis, no changes were observed during the follow-up period.
Results of the WORMS Subscales.
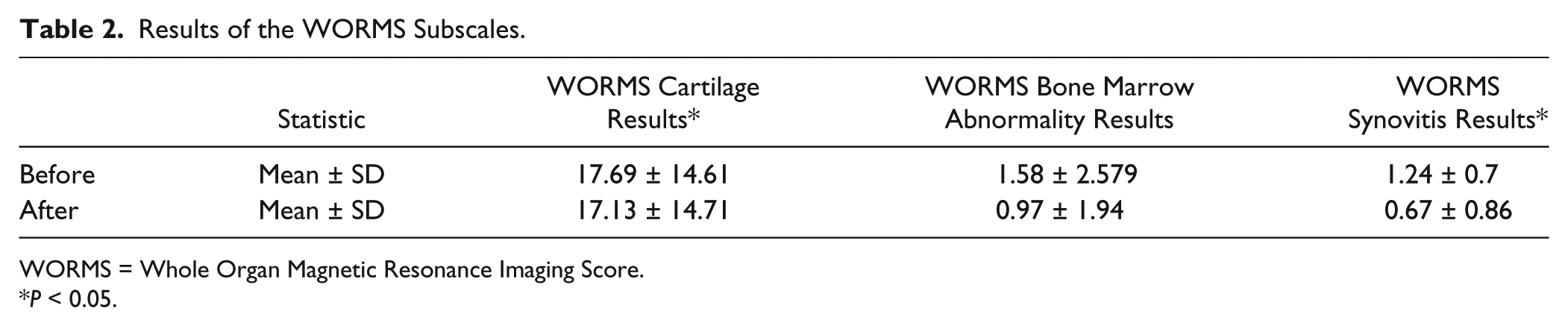
WORMS = Whole Organ Magnetic Resonance Imaging Score.
P < 0.05.
Edema of the bone marrow has been usually associated with pain and degenerative activity of the OA. A decrease from 1.58 WORMS points to 0.97 points was observed. Further analysis of the WORMS bone marrow abnormalities section demonstrated a decrease of the bone marrow edema in 57.14% of the patients after the period of 6 months, whereas 28.57% had no changes, but in 14.29% worsening was observed. The MRI changes related to the synovitis improved in 63.16% of cases, no difference was observed in 31.58% and they increased in 5.26% of the cases ( Fig. 4 ).
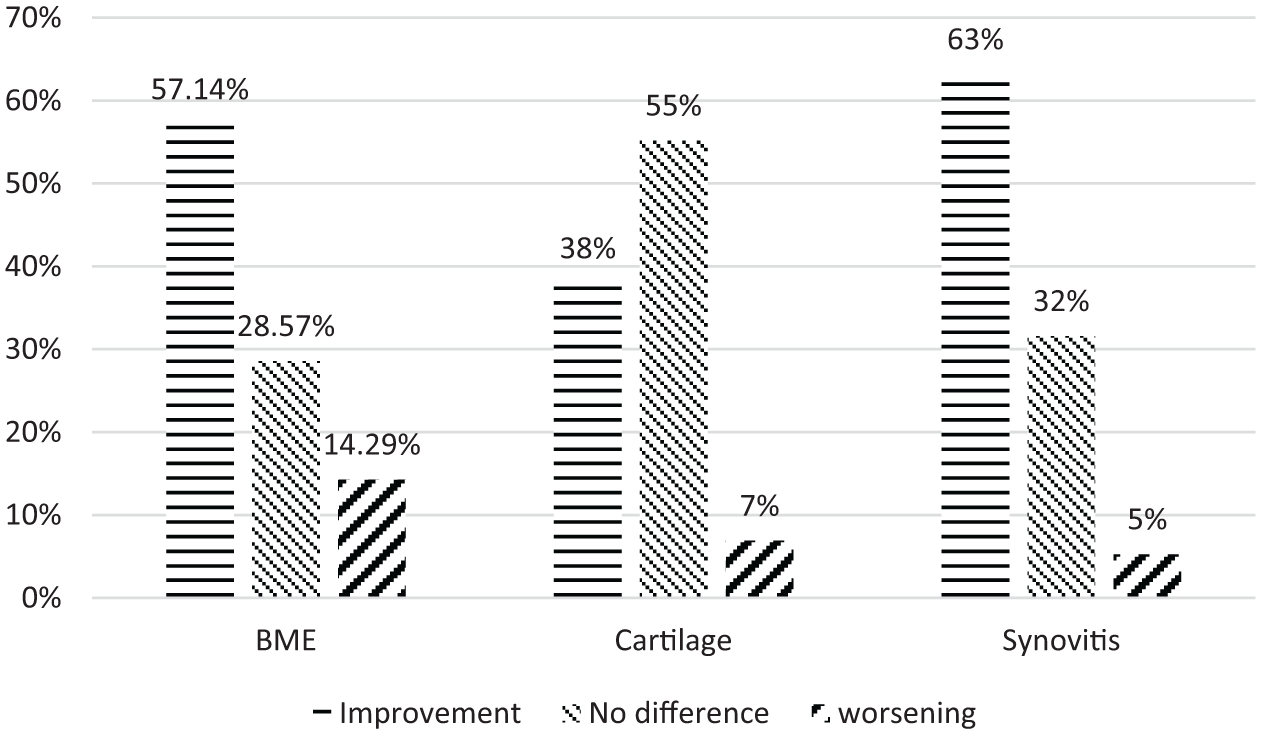
Magnetic resonance imaging (MRI) changes after 6 months.
Cartilage changes in the MRI after 6 months period improved in 37.93%, no change was observed in 55.17% and further degeneration was present in 6.90% of cases.
Distribution of the cartilage lesions in the knee joint is outlined in Figure 5 .
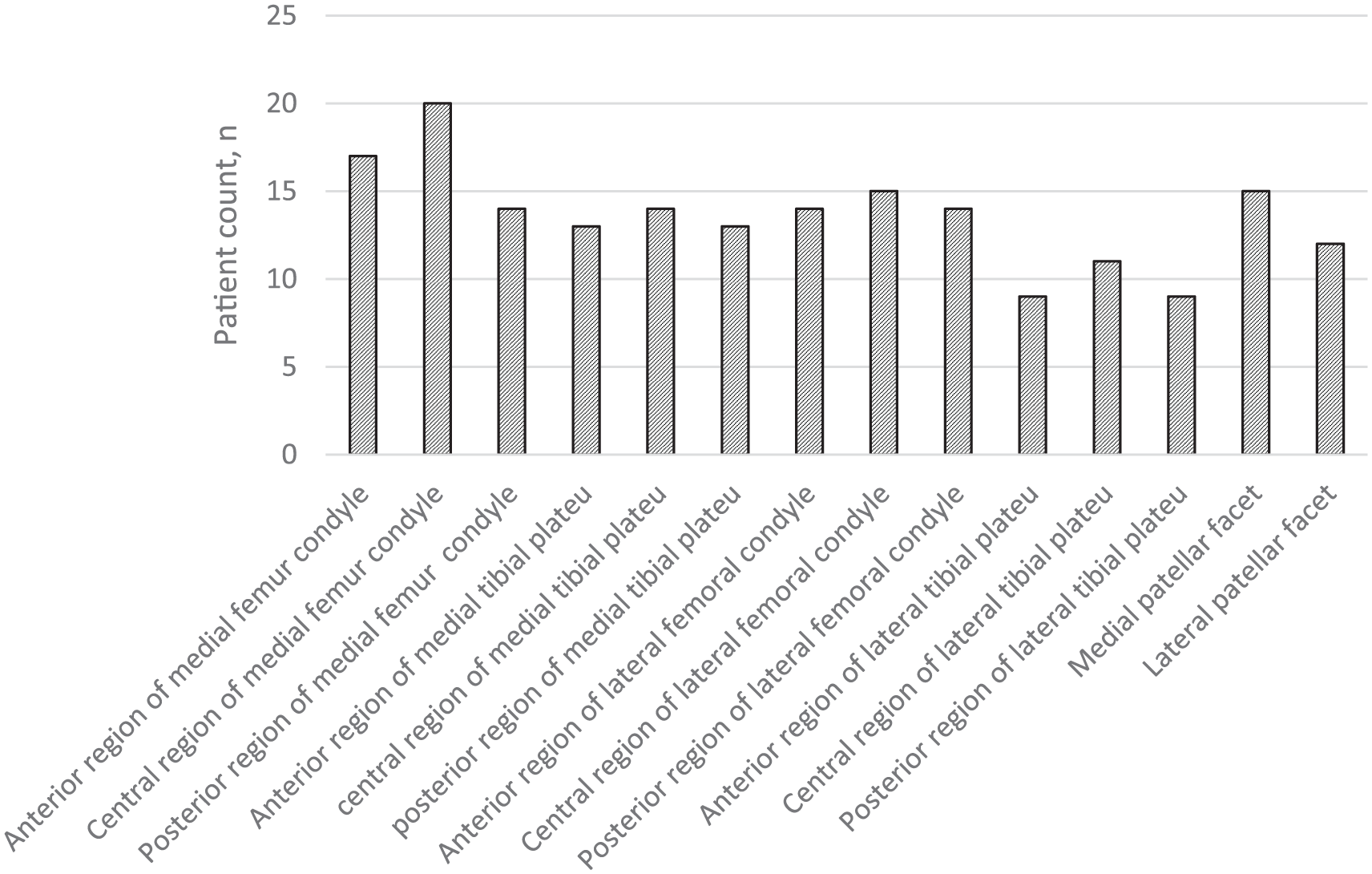
Locations of the cartilage lesions.
Analysis of the Cell Material
After preparation of the red bone marrow using gradient centrifugation method all extracted mononuclear cell material was returned to the same patient. Before the injection, flow cytometry tests were applied to each extracted mononuclear cell sample. Mononuclear and CD34+ population count, as well as cell viability was analyzed. Among 34 cell samples, 24 were analyzed by the flow cytometry tests, 10 were excluded according to the protocol, while the measurement did not reach 50,000 events. We observed a wide distribution of the cell yields (8.3 × 106 to 158.79 × 106). The average final yield of the cell extraction was 45.56 × 106 ± 34.94 × 106 MNC containing 1.04 × 106 ± 1.61 × 106 CD34+ cells. The cell viability was detected prior the cell extraction process in the red bone marrow and after the final cell preparation. The average cell viability in the red bone marrow was 74.36% ± 9.85%, but after the preparation processes the viability increased to 79.75% ±11.28%.
No positive correlation between the used cell quantity and the improvement in the OA clinical signs was found.
Discussion
MSCs can be isolated from several human sources, such as bone marrow, adipose tissue, synovial membrane, synovial fluid, umbilical cord blood, periosteum, dermis, trabecular bone, infrapatellar fat pad, articular cartilage, etc.21,22 Among these, the ones derived from the bone marrow or the adipose tissue are more often used in clinical practice. After extraction, the MSCs can be multiplied by culturing or used just as a cell concentrate. The cultured cells are characterized by higher number of homogeneous cells, while the concentrated ones are smaller in numbers and more heterogeneous but are kept in their original niche, and therefore their effect is possibly favored. 23 The most suitable strategy is not clear until now. The count of MSCs extracted from the adipose tissue demonstrates significantly higher numbers comparing to those from the bone marrow aspirate. Despite higher MSC count in the adipose tissue, certain studies show ability of the BMSC to produce higher levels of the collagen II and sulfated glycosaminoglycans, which can benefit in a better cartilage extracellular matrix formation.24,25 Most of the bone marrow progenitor cells are of hematopoietic lineage while the MSCs capable of differentiating into bone, cartilage, and synovial tissue population are very low in count. 26 The estimated frequency of the MSC in the BM nucleated cell population differs in range from 0.0017% to 0.034%. 27 Easy access to the mononuclear cell fraction containing all bone marrow stem cells (BMSC) by using the bone marrow concentration makes them beneficial for practical use. Cell yields and correlation to clinical effects are active topics for discussion in all fields using the MSCs as a therapeutic agent. There is no clear answer so far. We observed a wide distribution of cell yields (8.3 × 106 to 158.79 × 106). The extracted mononuclear cell yield could depend on the patient’s individual condition or the bone marrow acquisition and the cell processing quality. In the previous study on the BM MNC processing efficacy, similar variety of mononuclear cell quantity was found. 28 Correlation between the used mononuclear cell quantity and the clinical improvement during 12 months was not evident.
In the study of Jo et al. 29 adipose tissue–derived MSCs (AD MSCs) were used. Eighteen patients with knee OA were divided into 3 groups and treated by different MSCs dosages: 1 × 107, 5 × 107, and 1 × 108 cells. The increase in the score results with superiority of high-dose group was reported. 29
A larger sample group and a wider range between the used cell quantities could be helpful in finding the optimal cell dosage patterns for achieving the best clinical results.
Clinical benefit has been showed in most of the clinical studies on the use of BMSC in the treatment of isolated cartilage lesions and OA patients regardless of the cell source, indication, or administration method, with better results in the patient groups of younger age, lower BMI, smaller lesion size, and earlier stages of OA.29,30 No major adverse events strictly related to the treatment have been reported. 23 Gobbi et al. 31 used transplantation with BMAC covered collagen matrix in 15 patients operated for knee cartilage lesions of grade IV. A significant improvement in all scores and particularly improvement of results of the KOOS score of about 20 points was reported. 31
Comparing the clinical effect measured by the KOOS score, we found similar improvement levels as reported by Oliver et al. 32 Approximately 10 points higher improvement levels have been reported by Kim et al. 33 Both teams have used BMAC and lipoaspirate combination injected in the knee joints affected by OA. 33
Assessment of the scores of our patient group shows statistically significant reduction in pain. Score improvement of about 20 points still lasted in the 12th months of follow-up. A maximum of beneficial effects, such as relief of pain and OA symptoms and improvement of the daily activities, were reached in the first month after the procedure, and it continued at the same level or slightly decreased during 12 months of follow-up period. Despite that, the quality of life improved continuously and reached the maximum in the 12th month. The highest improvement was observed in knee pain. Least improvement was observed in other OA symptoms like stiffness or crepitation in the joint. However, the improvement correlation to age or OA K-L stage was not evident in our patient group.
Centeno et al. 34 in their study analyzed the largest patient material of 681patients and 840 knees. This study demonstrated both decrease in knee pain and functional improvement after using the injection of BMAC, pure and augmented with PRP and the adipose tissue, in the treatment of knee OA. 34 However, more adverse effects like knee pain and swelling in the BMAC and the BMAC combined with adipose tissue groups were reported. No differences in clinical improvement between groups were found. In our study, the bone marrow aspirate was processed in order to isolate mononuclear cells and reduce contamination with red blood cells and erythrocyte lysate. We assume that purification of the cell solution is the reason why no adverse effects like swelling and pain after the cell injection were observed.
Because of the lack of a control group, it is necessary to compare our results with studies about natural history of knee OA progression. The analysis of the literature about the natural progression of the knee OA shows that once the OA process is started progression is inevitable. In the Framingham osteoarthritis study with 869 subjects, a K-L grade progression was observed on 3% male and 4 % female participants per year. 35
Another study with 942 patients and 4-year follow-up concluded that a greater decrease in 4-year joint space width (JSW) significantly correlated with worse 4-year KOOS Pain, Symptom, and Quality of Life, and particularly a 3.5-mm loss of JSW over 4 years correlated with a clinically significant 8-point drop in 4-year KOOS Pain scores. 36 When comparing the results with those reported in literature about the natural knee OA progression, it can be seen that our results indicate clear and notable improvement of OA clinical signs compared with baseline. Therefore, it is likely that injection of BM MNC is associated with these improvements.
The natural history of the knee joint space narrowing in knee OA patients also has been studied by numerous studies.37,38 It has been reported that estimated joint space narrowing ranges from 0.1 to 0.3 mm/year; however, variation exists around these numbers. In our patient group, we did not observe joint space narrowing during the 12 months of follow up period.
Koh et al. 39 have used adipose derived cultured MSCs in the patients of knee OA. The results of this study analyzed by MRI using WORMS score significantly improved from 60.0 points to 48.3 points (P < 0.001). Particularly notable was the change in cartilage WORMS, which improved from 28.3 points to 21.7 points (P < 0.001). 39
Our MRI findings also demonstrated the WORMS score improvement and a significant reduction of the synovial effusion and the bone marrow edema. Restoration of the cartilage surface was observed in some individuals, but it was not clearly evident in the majority of cases. However, the lack of a control group limits as to association of the observed changes with applied therapy. The natural history of the osteoarthritis progression should be taken in account. Bone marrow edema is usually associated with pain and activity of the degenerative process. 40 Loss of the bone marrow integrity will compromise repair and regeneration and faster degeneration on the joint cartilage. Raynauld et al. 41 has reported that in natural history of knee osteoarthritis further progression of cartilage defects can be found in MRI with respective cartilage volume loss of 3.8% and 6.1% at 6th and 24th month. In another study from Ding et al., 42 33% of patients with knee OA had worsening of cartilage defect score, whereas 37% of patients had improvement in 2-year period. The study by Davies-Tuck et al. 43 shows that in 2-year period, cartilage defect score decreased even in 81% of patients in 2-year period and improvement was observed only in 4%. In our study, the cartilage had improved in 37.93% of patients however further degeneration occurred only in 6.9% of cases and the rest remained unchanged. While comparing with the literature data about natural knee OA progression on MRI, we could not draw strong conclusion regarding the improvement of the joint structures associated with applied treatment method. However, it seems that our treatment method could slow down progression of cartilage degeneration.
Limitations
There was no control group in this study. The placebo effect might play a role in the patient’s subjective self-scoring process. Some of the differences measured with scores were not statistically significant because of a high variability of results. Of course, a larger sample size and a longer follow up period could be helpful to improve the strength of our conclusions and to collect data about the factors influencing patient outcome.
Conclusions
The intra-articular injection of the BM MNCs is a safe manipulation with no serious side effects over the 12-month period.
The BM MNC injection in majority of cases provides a statistically and clinically significant improvement of knee osteoarthritis of stage II-III symptoms at the 12-month period.
Injection of BM MNC suspension in the knee joints affected by OA of stage II-III suggests slowing down of degenerative structural changes of the knee joint tissue.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Pauls Stradins’ Clinical University Hospital, University of Latvia, Research Institute of Cardiology, Latvian State Hospital of Traumatology, and Orthopaedics for institutional support. This study was supported in part by the Latvian National Research Program “Biomedicine for Public Health” (BIOMEDICINE) and by grant from the “Sistemu Inovacijas” corporation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The clinical study protocol was approved by the State Central Medical Ethics Committee.
Informed Consent
All patients provided informed consents for the study according to the Helsinki Declaration, and all patients voluntarily agreed to participate and signed informed consent forms.
Trial Registration
Not applicable.