
Abstract
Objective
To test different fixation methods of a 3-dimensionally woven poly(ϵ-caprolactone) (PCL) scaffold within chondral defects of a weightbearing large animal model.
Methods
Full thickness chondral defects were made in the femoral condyles of 15 adult male Yucatan mini-pigs. Two surgical approaches were compared including total arthrotomy (traditional) and a retinaculum-sparing, minimally invasive surgery (MIS) approach. Following microfracture (MFX), scaffolds were placed without fixation or were fixed with fibrin glue, suture, or subchondral anchor. Experimental endpoints were between 1 and 6 weeks. Micro–computed tomography and histology were used to assess samples.
Results
The MIS approach was superior as the traditional approach caused medial condyle cartilage wear. One of 13 (7.7%) of scaffolds without fixation, 4 of 11 (36.3%) fibrin scaffolds, 1 of 4 (25%) of sutured scaffolds, and 9 of 9 (100%) of anchor-fixed scaffolds remained in place. Histology demonstrated tissue filling with some overgrowth of PCL scaffolds.
Conclusions
Of the methods tested, the MIS approach coupled with subchondral anchor fixation provided the best scaffold retention in a mini-pig chondral defect model. This finding has implications for fixation strategies in future animal studies and potential future human use.
Introduction
Once damaged, adult articular cartilage has limited ability to heal and will often continue to deteriorate, leading to arthritis, pain and disability.1,2 Over the past 20 years, many different surgical strategies have evolved to treat focal cartilage lesions with no single treatment proving superior.3,4 Autologous chondrocyte implantation (ACI) represents one treatment strategy that has received increasing interest with recent literature suggesting that ACI may offer superior results to traditional microfracture techniques. 5
ACI as a treatment strategy includes the implantation of autologous, externally cultured chondrocytes into a cartilage defect. ACI originally included the implantation of chondrocytes underneath a periosteal membrane. 6 This first generation ACI technique returned mixed clinical results and resulted in fibrotic hypertrophy in 10% to 26% of treated patients. 7 In response, matrix-assisted ACI (MACI) was developed in which chondrocytes are cultured onto a 3-dimensional (3D) collagen scaffold prior to implantation. 2 By using a scaffold, chondrocytes could be secured in the defect while avoiding the hypertrophic effects of a periosteal cover. While clinical results after MACI have been promising,8,9 there is interest in developing scaffolds that better promote hyaline-like cartilage and that maintain biomechanical properties similar to surrounding cartilage during the repair process. 10
Another material, poly(ϵ-caprolactone) (PCL), is a well-known, slowly degrading polyester that has a long track record of safe implantation into humans. 4 Recent studies examining PCL implantation into cartilage defects have described potential for cartilage repair,11-14 as well as integration into both subchondral bone and surrounding cartilage. 4 A recent study by Christensen et al. 4 showed evidence that at 13 weeks, a PCL scaffold implanted into an osteochondral defect demonstrated better filling, better integration, higher levels of chondrogenic markers, and higher histologic scoring compared with a collagen membrane. 4 Our group has extensive experience with 3D woven PCL scaffolds that exhibit functional biomechanical properties similar to those of hyaline cartilage, both at baseline and after extended culture and tissue maturation.15-17 This PCL scaffold therefore represents a potential implant that meets the goals of promoting articular cartilage formation while maintaining cartilage-like biomechanical properties.
An often overlooked aspect of scaffold-based cartilage repair is fixation technique.18,19 Without reliable scaffold fixation in vivo, integration to surrounding tissue may not be achieved. At worst, the scaffold may dislodge, becoming an intra-articular loose-body causing further damage to the cartilage.
20
Current literature examining fixation techniques for various scaffold, including PCL scaffolds, is limited. Several small animal studies have reported adequate fixation of PCL scaffolds both with fibrin glue,
4
and with press fitting.21,22 A single large animal study describes fixation of PCL scaffolds with both press-fit and with a poly(
With the availability of a novel woven PCL scaffold that has potential to better encourage hyaline-like cartilage formation while maintaining hyaline cartilage biomechanical properties, there is interest in performing comparative large animal studies. Prior to long-term large-animal studies, however, it is necessary to identify a reliable fixation technique for the PCL scaffold. The purpose of this study was to identify the most reliable fixation strategy of a 3D-woven PCL scaffold in a chondral defect model in the Yucatan mini-pig.
Methods
Animal Model
All animal procedures were performed at the University of Pennsylvania with approval from the Institutional Animal Care and Use Committee (IACUC). Fifteen adult male Yucatan mini-pigs (Sinclair Bioresources) underwent unilateral stifle joint surgery. All procedures were performed under anesthesia with sterile technique. Following surgical procedures, animals were housed independently and were allowed full weightbearing with unrestricted movement. Experimental endpoints for animals were between 1 and 3 weeks except for 1 final animal that was euthanized at 6 weeks.
Surgical Approach
Two surgical approaches were examined for their ability to promote scaffold retention and preserve the integrity of the knee articular surface. The traditional approach, which has proved successful in juvenile pigs, 24 was performed by creating a lateral parapatellar arthrotomy extending from the tibial tubercle to the vastus lateralis following a medial parapatellar skin incision. This approach included cutting through the lateral patellar retinaculum. The patella was dislocated medially to expose the trochlea of the femur. On closure, the retinaculum and capsule was repaired with 0-Vicryl suture.
Despite previous success in juvenile animals, pilot experiments proved that the traditional approach was inadequate for scaffold retention in adult animals. Therefore, we adopted a minimally invasive surgical (MIS) approach described previously. 25 We utilized this approach in order to preserve tracking of the patella in the trochlear groove. Briefly, a skin incision was made along the medial stifle joint. A medial arthrotomy was made from the tibial tubercle to the inferior border of the patella. Care was taken to preserve the medial retinaculum. The infrapatellar fat pad was sharply dissected, and the patellar tendon was retracted without dislocating the patella to expose the trochlea. The joint capsule was repaired with 0-Vicryl suture.
Defect Creation and Fixation Techniques
Following trochlea exposure, full-thickness circular chondral defects (4-mm diameter) were created in the trochlear groove (n = 4 per knee). Defect sites were demarcated with a 4-mm biopsy punch and a curette was used to remove cartilage to the level of the subchondral bone. In each defect, an awl was used to create 3 microfracture holes in the subchondral bone (0.8-mm diameter × 2-mm depth). Scaffolds were placed in each defect and were fixed. All were flush with the articular surface. Tested fixation strategies progressed in a stepwise manner until scaffold retention rate reached 100%.
Scaffolds were initially implanted without any additional fixation following a traditional approach ( Fig. 1A ). Scaffolds were pressed into the defect and pressure was applied for 5 minutes to allow infiltration and clotting of blood from microfracture holes. This was compared with fibrin-secured (Tisseel, Baxter Healthcare) scaffolds following the traditional approach. Fibrin-secured scaffolds were pressed into the defect and fibrin sealant was applied over the top of the scaffold and allowed to set for 5 minutes ( Fig. 1B ). Fibrin was applied only to the scaffold top as fibrin has been shown to block cell migration. 27
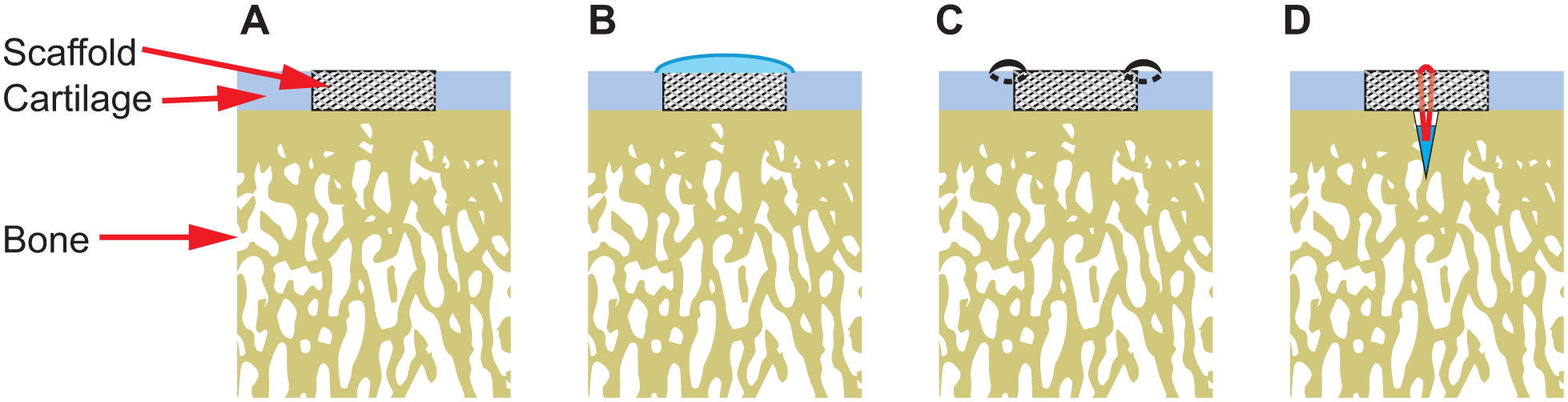
Poly(ϵ-caprolactone) scaffold fixation techniques. (
After the traditional approach was abandoned, fibrin fixation was again tested with the MIS approach. This was followed by transchondral suture fixation with two to four 6-0 vicryl sutures securing each scaffold to the adjacent cartilage ( Fig. 1C ). Finally, subchondral bone anchors (Mitek Microfix Quickanchor, Depuy) were used to secure the scaffolds. Anchors loaded with 6-0 suture were deployed into a central predrilled hole (1.3-mm diameter × 5-mm depth) in the subchondral bone of the defect. Both ends of the suture were threaded through the center of the scaffold and tied over the scaffold top ( Fig. 1D ).
Scaffold Design
Three-dimensional textile scaffolds were produced by weaving multifilament PCL yarns (~150 µm in diameter) in orthogonal x-, y-, and z-directions. 15 The yarns were woven into a flat structure measuring 0.75 mm thick to precisely match the thickness of the native porcine articular cartilage. After weaving, the material was soaked in 4 M NaOH for 15 to 16 hours to clean the fibers of surface contaminants and increase hydrophilicity. Scaffold discs of 4-mm diameter were punched from the flat material using a biopsy punch and sterilized using ethylene oxide gas.
Biomechanical Testing
Pull-out tests of each fixation strategy were performed to determine the force required to both displace the scaffold 100% from a chondral defect and for the scaffold to pull free from each respective osteochondral plug. Full-thickness 4-mm chondral defects were prepared ex vivo in osteochondral plugs harvested from bovine femoral trochleae. Woven PCL scaffolds were implanted in the defects with fibrin (n = 6), suture (n = 6), or anchor (n = 4) fixation, utilizing the same methods as employed during surgery. One end of a 0-vicryl suture loop was securely adhered to the top surface of the scaffold with super glue and the other loop end was attached to a 50 N load cell attached to an Instron 5848 mechanical tester. Tensile tests were performed perpendicular to the chondral surface ( Fig. 2 ). Samples were loaded at a crosshead speed of 0.05 mm/s. For reference, the tensile strength of 6-0 Vicryl suture loop was also tested (n = 4). Forces at which the scaffold was displaced 100% (0.75 mm) from the defect, and at which mechanical failure (complete separation of scaffold and osteochondral plug) occurred were measured.
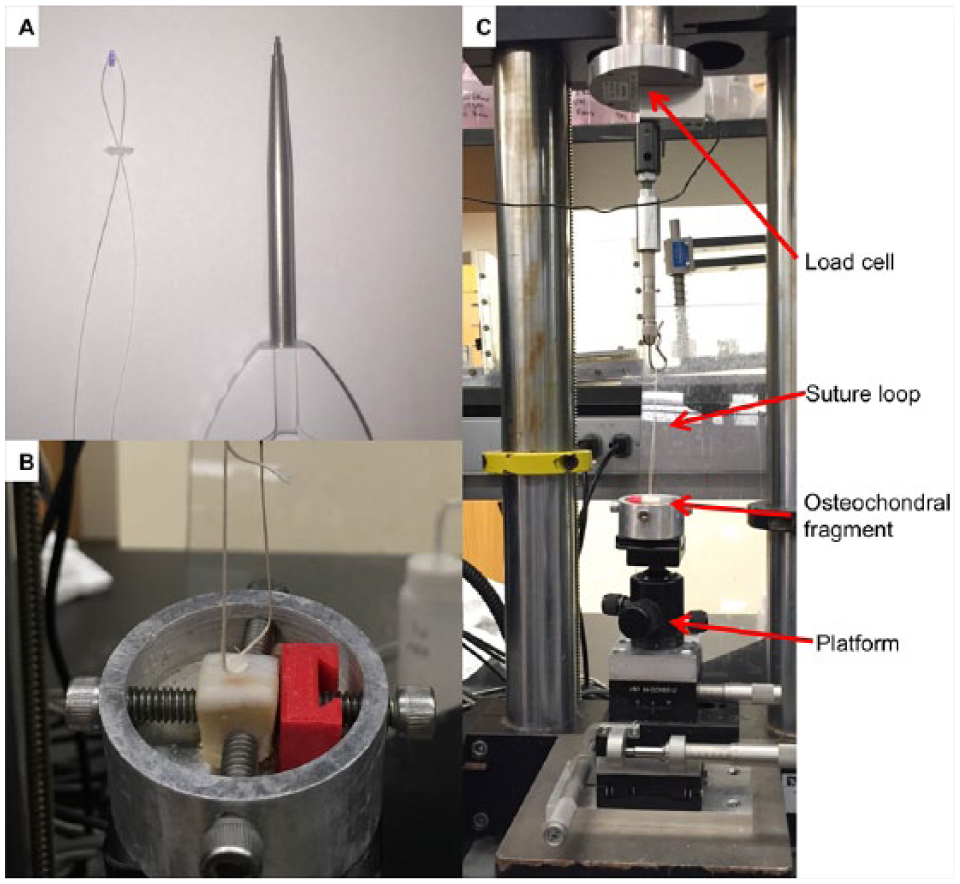
Tensile testing of a poly(ϵ-caprolactone) (PCL) scaffold within an osteochondral defect. (
Scaffold Retention Analysis
After euthanasia and gross inspection, four osteochondral specimens including defects were removed and fixed in 10% formaldehyde. Samples were immersed in a contrast agent (Lugol’s solution, Sigma-Aldrich) for 48 hours. Micro–computed tomography (µCT) was performed on each specimen (Viva CT75; Scanco) to confirm gross findings of scaffold retention, to assess for scaffold migration, and to assess surrounding bone reaction. After µCT, samples were decalcified (Formical 2000; Decal Chemical Corporation) for 1 week. Samples were then dehydrated, paraffin embedded, and sectioned to 7 µM. Sections were stained with hematoxylin and eosin (H&E) as well as Safranin O and Fast Green (SafO/FG). Samples with retained scaffolds underwent immunohistochemistry to assess deposition of type I and type II collagen. Sections were rehydrated and subjected to proteinase K antigen retrieval. Sections were incubated with a type I antibody (5 µg/mL; Developmental Studies Hybridoma Bank, University of Iowa) or a type II antibody (5 µg/mL; Developmental Studies Hybridoma Bank, University of Iowa) overnight at 4°C. After washing, bound antibody was detected using the Millipore Immunoperoxidase Secondary Detection System (EMD Millipore Corporation).
Statistical Analysis
Statistical analysis for the biomechanical testing was performed with 1-way analysis of variance and post hoc Tukey’s comparison test. Statistical analysis of scaffold retention data was performed using Fisher’s exact test with Bonferroni’s correction when appropriate. Analysis was performed in GraphPad version 6.04 for Windows (GraphPad Software, La Jolla, CA) and in R version 3.3.2.
Results
Scaffold Retention
Following surgery, all animals were walking within 12 hours and had no noticeable gait abnormalities after recovery. Sixteen scaffolds were placed into defects following the traditional surgical approach. Only 1 of 13 (7.7%) scaffolds without fixation remained in place, and only 1 of 3 (33.3%) scaffolds fixed with fibrin remained in place after 1 to 3 weeks ( Fig. 3 ).
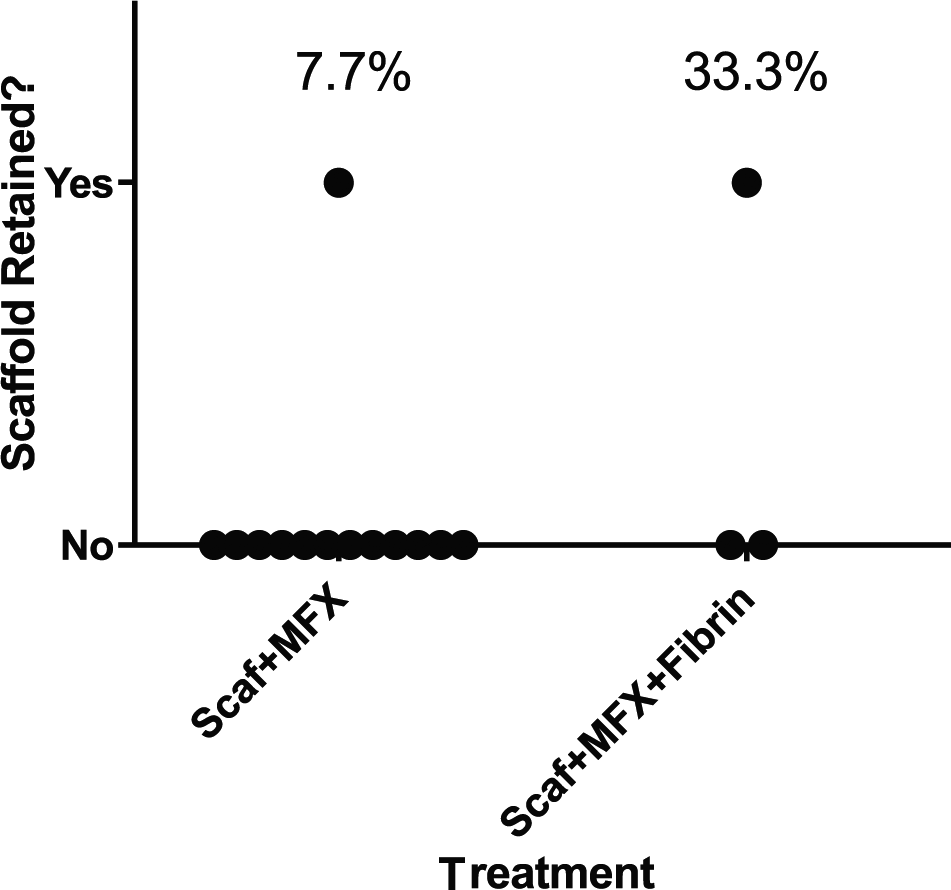
Comparison of poly(ϵ-caprolactone) (PCL) scaffold retention rates using the traditional surgical approach with or without application of fibrin glue covering. There was no significant difference between fixation methods in the traditional surgical approach (P = 0.35). Scaf = PCL scaffold; MFX = microfracture.
In addition to scaffold loss, pigs receiving the traditional approach also showed gross signs of mechanical damage to the medial trochlea ( Fig. 4 ). The direct mechanical damage was thought to play a role in scaffold loss, and the traditional approach was abandoned.
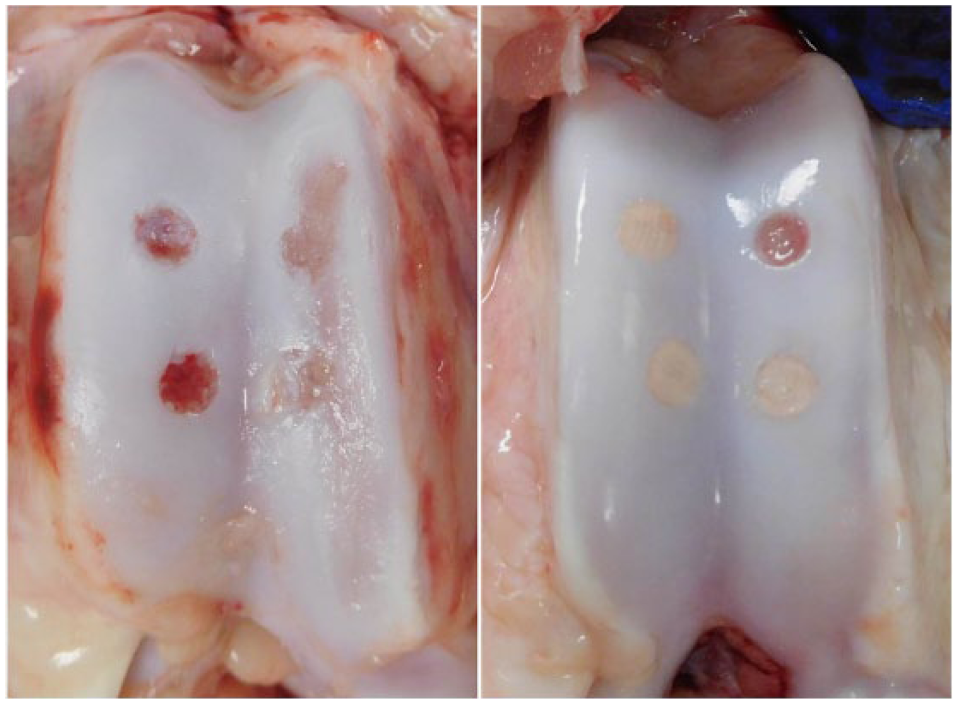
Femoral trochlea of pigs following traditional (left) versus minimally invasive surgery (MIS) (right). Linear mechanical wear along the medial condyle was noted in a majority of stifle joints following traditional surgery. Three intact poly(ϵ-caprolactone) (PCL) scaffolds and 1 empty defect are noted in the MIS example.
Twenty-four scaffolds were placed following the MIS approach. Four of 11 (36.3%) fibrin-fixed scaffolds were found in place after 2 weeks and there was no evidence of medial cartilage wear ( Fig. 4 ). Fixation with suture was found to be technically challenging given the thin cartilage of adult pigs, and only 1 of 4 (25%) scaffolds were found in place after 2 weeks. Finally, 5 of 5 (100%) of scaffolds fixed with anchors were found in place after 2 weeks. Four of 4 (100%) anchor-fixed scaffolds were also found in place after 6 weeks ( Fig. 5 ).
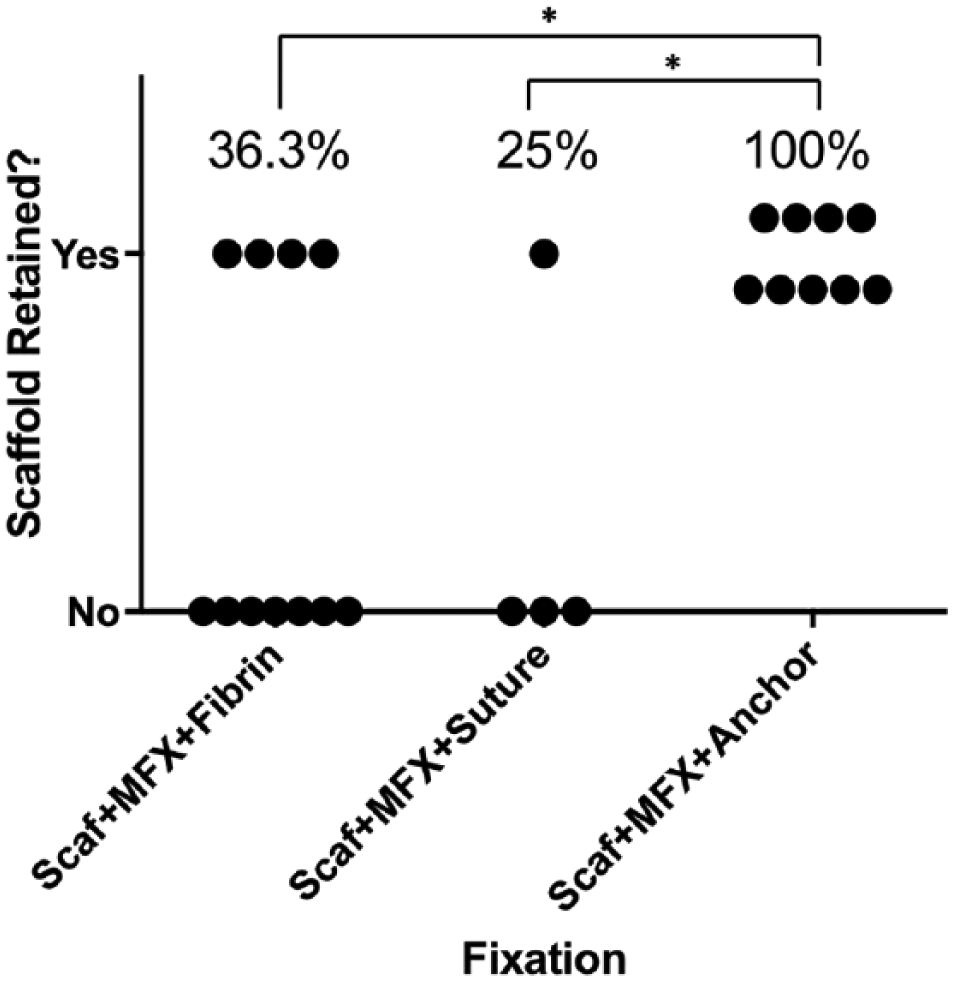
Comparison of poly(ϵ-caprolactone) (PCL) scaffold retention rates using the minimally invasive surgical approach, comparing fibrin, suture, and subchondral anchor fixation methods. Anchor fixation significantly increased retention when compared with suture (P = 0.042) and fibrin fixation (P = 0.0142). Scaf = PCL scaffold; MFX = microfracture. *P < 0.05.
Biomechanical Testing
Scaffolds fixed with fibrin resisted tension until the fibrin failed and the scaffold was pulled free from the defect. The suture and anchor-fixed scaffolds were gradually displaced from the defects as the suture stretched until suture failure. Fibrin fixation and suture fixation were comparable in tension force needed for scaffold displacement but suture-fixation required a statistically significant greater force to cause failure (0.49 ± 0.46 vs. 0.17 ± 0.22 N and 0.49 ± 0.43 vs 3.99 ± 2.25 N, respectively). The most common reason for construct failure was suture pulling through the cartilage. Anchor fixation required a statistically significant greater force for scaffold displacement and construct failure compared with fibrin (0.49 ± 0.46 vs. 3.53 ± 1.06 and 0.49 ± 0.46 vs. 6.96 ± 2.94 N) and compared with suture fixation (0.172 ± 0.23 vs 3.53 ± 1.066 and 3.99 ± 2.36 vs. 6.96 ± 2.94 N). Anchor load to failure was statistically equivalent to the suture control (6.96 ± 2.94 vs. 7.60 ± 0.56) ( Fig. 6 ).
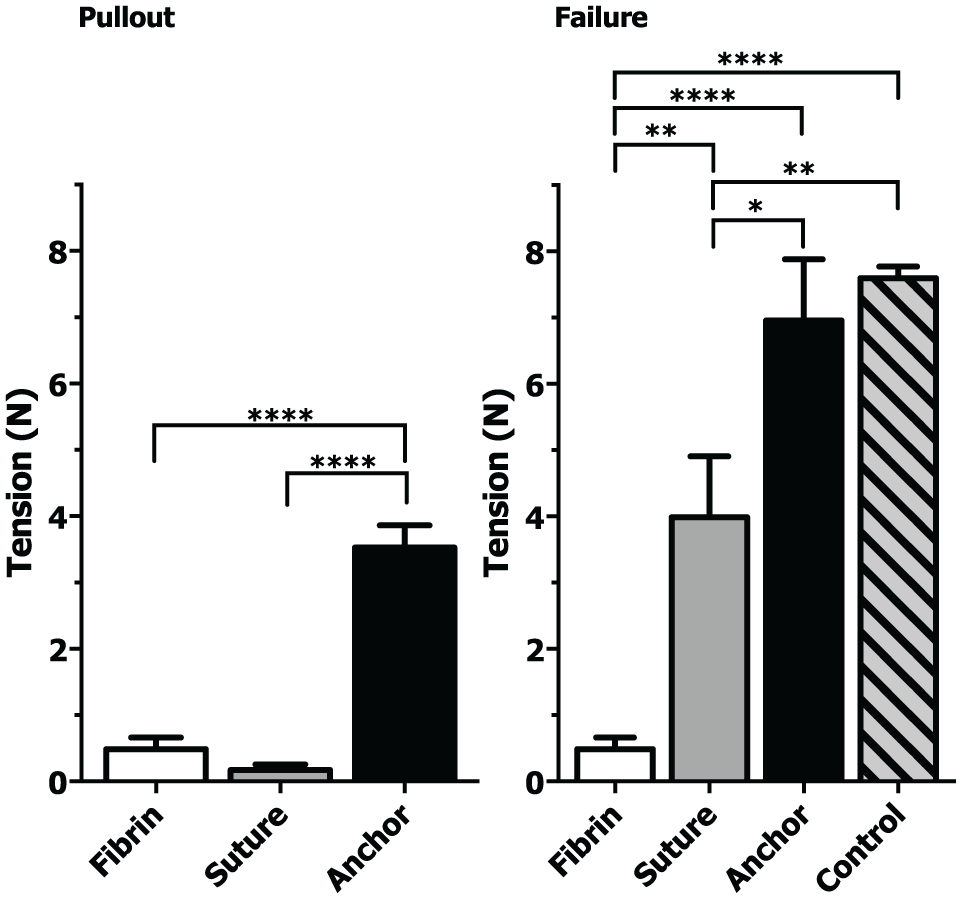
(Left) Tensile force required to displace the poly(ϵ-caprolactone) (PCL) scaffold 100% from the defect (pullout). (Right) Tensile force required to cause total failure compared across different fixation techniques. Control indicates failure strength of suture alone. *P < 0.05, **P < 0.01, ****P < 0.0001. Control, Fibrin, Suture n = 6. Anchor n = 4.
μCT and Histology
Representative µCT and histology sections of an empty defect compared with an intact anchor-fixed scaffold are shown in Figure 7 . µCT analysis showed that scaffolds did not migrate when fixed with an anchor. However, µCT images also showed loss of trabecular architecture immediately below the scaffold and surrounding the anchor. Histologic analysis with H&E and SafO/FG at 2 weeks showed evidence of early matrix formation, and fibrous material overgrowing the scaffold. No obvious cell infiltration was noted. Fibrous material was found to have replaced the trabecular bone directly beneath the scaffold ( Fig. 8 ). Immunohistochemical staining revealed the space beneath the scaffold to contain both type I and type II collagen with no obvious trabecular-like architecture. Fibrous material overgrowing the scaffold also consisted of type I and type II collagen.
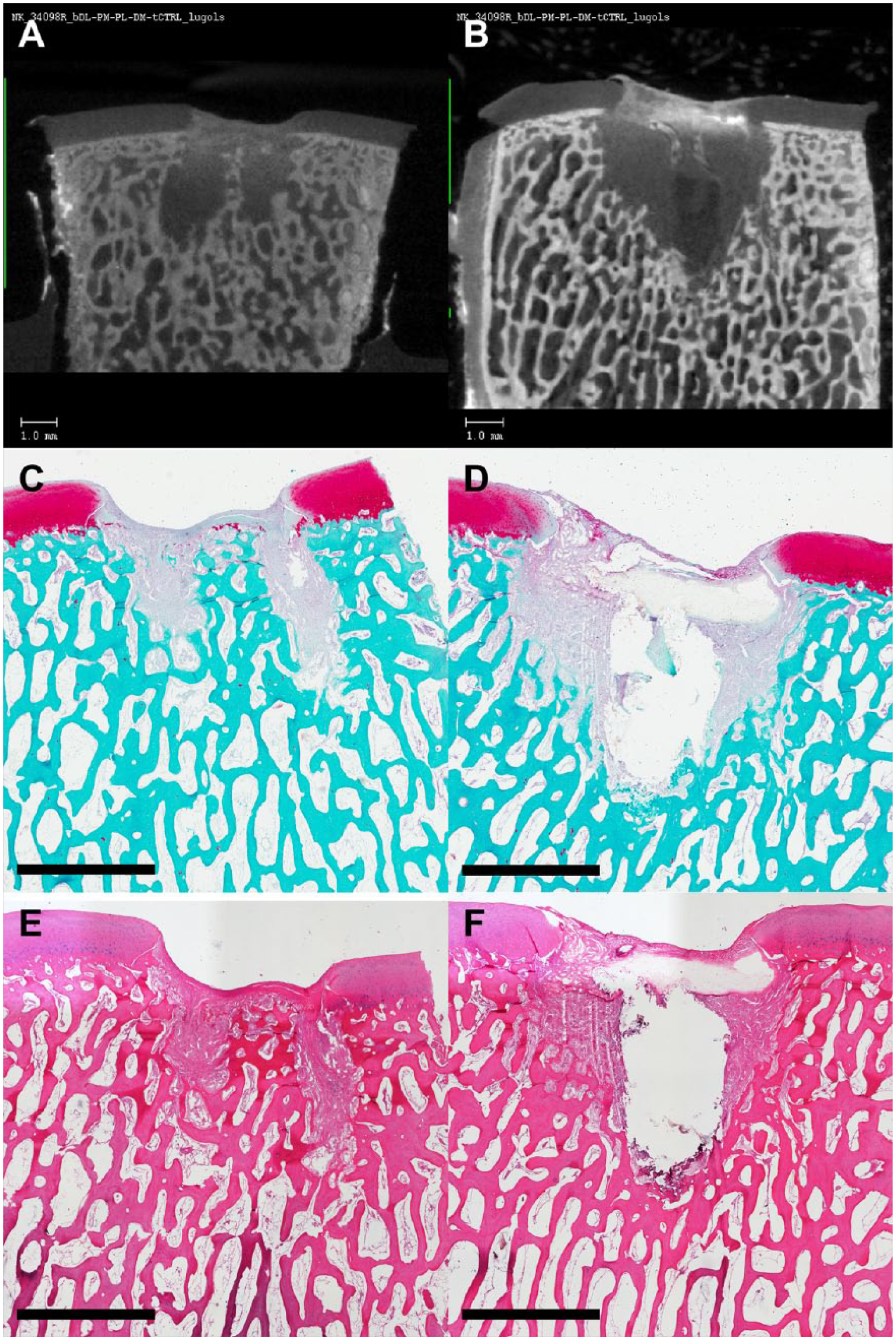
Representative images of micro–computed tomography (µCT) and histology of defects with failed fixation (left) and defects with anchor-retained scaffold. (
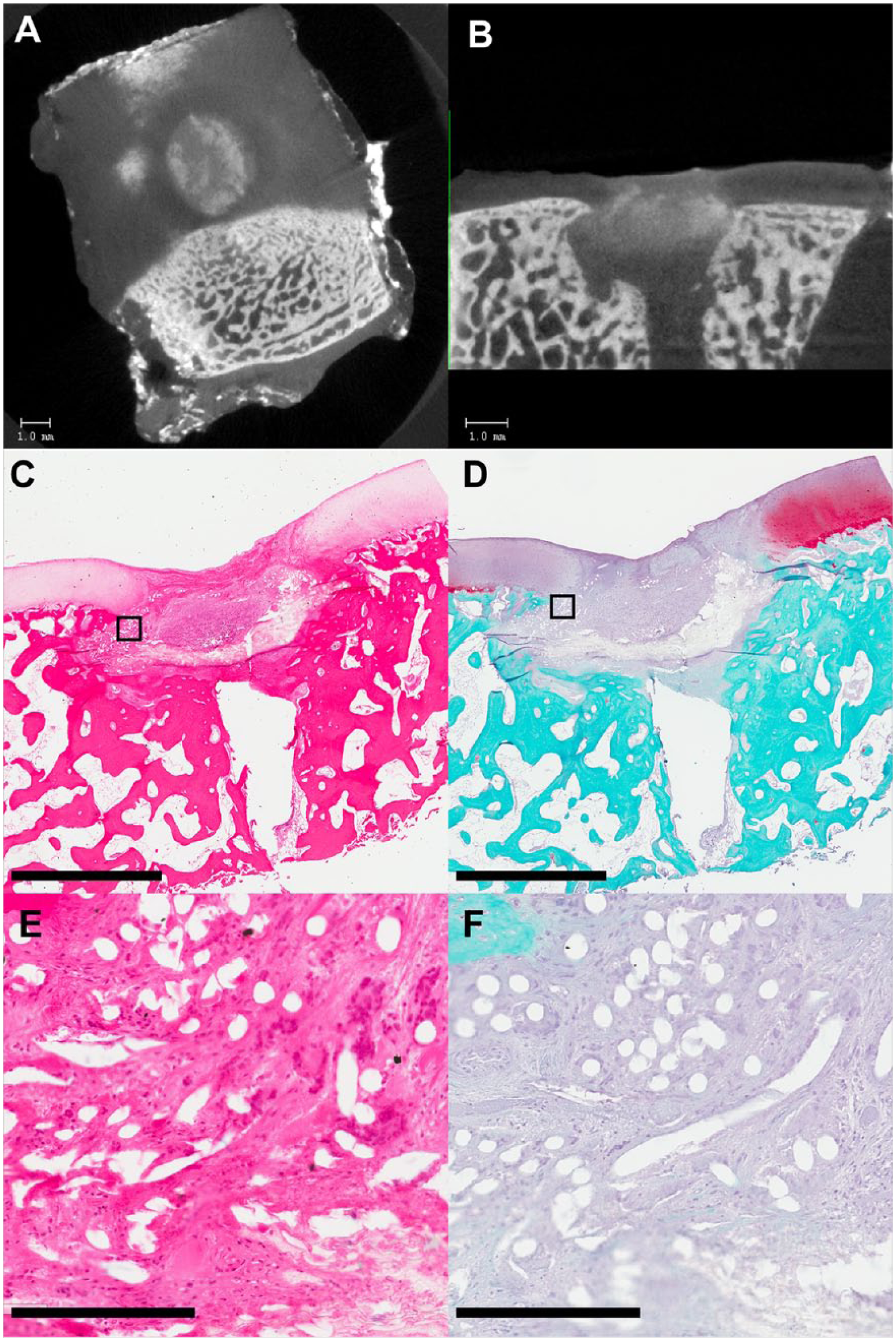
Micro–computed tomography (µCT) and histology of 6-week defects with retained scaffold. (
Discussion
The purpose of this study was to identify the most reliable fixation technique for implantation of a woven PCL scaffold used in a chondral defect in a clinically relevant large animal cartilage repair model. Our findings demonstrated that the PCL scaffolds used in this study are reliably fixed with subchondral anchoring, but that they were not secure without fixation, with fibrin gluing, or with suturing. The surgical approach was a critical factor and sparing the patellar retinaculum during implantation appeared to be important to protect the cartilage and scaffolds from mechanical stress postoperatively.
Without fixation, few PCL scaffolds stayed confined within the chondral defects created in this study. This is may have resulted from the lack of an adequate “press-fit” as the woven textile scaffolds are inherently flexible and may have deformed instead of generating sufficient frictional forces with the surrounding cartilage to remain in place. Unfixed scaffolds may have also been dislodged by shearing forces generated through direct contact with the opposing patellar cartilage as the joint articulated. Since the thickness of the scaffolds used in this study precisely matched the thickness of the native cartilage, full-thickness defects were created with flat, smooth bases on the subchondral bone. However, variation in preparation of the defect may have resulted in an uneven base and caused the scaffold to extend beyond the height of the surrounding cartilage and into the joint space where it could be contacted and disrupted by the opposing cartilage surface. In theory, without fixation, scaffolds might remain in place from clot formation from the underlying vascularized bone. 19 Our findings are consistent with other literature showing that additional fixation is necessary to retain a PCL scaffold within chondral defects of a mobile knee joint, although this conclusion is not necessarily applicable to other conditions such as osteochondral defects or joint resurfacing. 26
Only about one-third of fibrin fixed scaffolds stayed in place. Biomechanical tests revealed that the tension force required to displace a scaffold fixed with fibrin glue is low, consistent with existing literature.7,28 Knecht et al. 19 found that fibrin fixation of non-PCL scaffolds infer varying strength depending on implant material, which may explain why fibrin fixation is considered adequate for other scaffold types. Drobnic et al. 7 reported fibrin glue interposed between scaffold and collagen as an adequate fixation technique for collagen scaffolds in human cadaver knees following passive range of motion but also found that scaffolds displaced with the addition of 10 and 20 kg compressive weight through the knee joint. 7 As fibrin glue may block mesenchymal stem cells from penetrating the scaffold, 27 we believe that placing fibrin overtop the scaffold is more effective and practical. Regardless, the animals in this study were fully weight bearing, and our results are therefore consistent with findings of Drobnic et al. 7 that load bearing through the knee joint may create shear forces that overcome the fixation strength of fibrin glue.
Only 25% of sutured PCL scaffolds stayed in place. This technique was only attempted once as it was found to be technically challenging and caused significant damage to the surrounding cartilage. Biomechanical testing showed that although the amount of force required to break the suture was relatively high compared with other fixation methods, the force required to displace the scaffold from the defect was low. This was because of the fact that suture could not be tightened enough to prevent displacement without tearing the surrounding cartilage. Failure of this construct occurred with the tearing of the suture through cartilage, which has been previously described in literature examining suture fixation. 19
Success occurred with subchondral anchor fixation where all PCL scaffolds were retained at 2 and 6 weeks. Biomechanically, anchor fixation required a slightly higher force to fail compared to fibrin or suture fixation, but required a much stronger force to displace the PCL scaffold compared with fibrin and suture fixation. It is likely that the most important factor in holding the PCL scaffold in place lies in preventing the scaffold from displacing from the defect. Complex noncompressive forces may act to pull the scaffold out of the defect. Scaffold extrusion above the plane of the surrounding cartilage may result in fixation failure and complete scaffold displacement due to shear forces exhibited by the patella. Anchor fixation is the only fixation strategy tested that provided enough pull to prevent scaffold extrusion during normal knee loading and motion.
Histologically the PCL scaffold showed evidence of fibrous ingrowth, consistent with studies of PCL scaffolds.11-14 The loss of trabecular architecture around the scaffold and anchor are also consistent with descriptions of histologic findings by Vikingsson et al. 23 following PCL fixation with a pin.
There were several limitations to this study. First of all, adult pig cartilage is thinner than human cartilage (0.75 vs. 2.5 mm), 29 which may alter the forces acting on the scaffold. In addition, our study confirmed the retention of scaffolds at 2 weeks (5/5) and at 6 weeks (4/4) but this may not be a long enough time point to guarantee long term placement of the scaffold. Another limitation is the inability to limit loading and mobility of the operative limb due to the mini-pig’s intolerance for casting or immobilization devices. While we observed pigs to favor the non-operative limb immediately following surgery, it is possible that early return to full weightbearing in the operative limb limited the efficacy of certain fixation techniques. The small defect size relative to total joint size is another potential limitation, as larger defects may be a more appropriate model of clinically encountered cartilage pathology. However, this defect size is useful for the evaluation of multiple treatments within the same joint, and has been determined to be of adequate size to prevent spontaneous healing in the mini-pig.24,30 It is important to note the subchondral remodeling response beneath anchor-secured scaffolds. It is unclear whether this response is caused by the presence of scaffold and anchor or is due to the creation of a full thickness chondral defects, as is seen in other animal models of cartilage repair.31,32 Studies with time points beyond 2 weeks are necessary to determine the extent of this response. Finally, although scaffold thickness was produced to match porcine cartilage thickness, variation in defect creation and depth may have affected whether scaffolds were proud.
In this study, we evaluated various fixation techniques of a PCL woven scaffold, including no fixation, suture, and subchondral anchor in a fully weightbearing, large animal model. Of these four techniques, only the subchondral anchor was sufficient for long term fixation of the woven scaffold in a chondral defect. These findings may have implications for future, longer term studies utilizing PCL woven scaffolds, and may also help determine the best fixation strategy for other synthetic scaffolds and ultimately when used in humans improve clinical outcomes.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided by the AO Foundation and the U.S. Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors Farshid Guilak, Bradley T. Estes, and Franklin T. Moutos are paid employees of Cytex Therapeutics, Inc.
Ethical Approval
Ethical approval for this study was obtained from University of Pennsylvania Institutional Animal Care and Use Committee (IACUC).
Animal Welfare
The present study followed international, national, and/or institutional guidelines for humane animal treatment and complied with relevant legislation.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.