
Abstract
Introduction
Autologous osteochondral transplantation (AOT) is a treatment for osteochondral lesions with known concerns, including histological degradation of the graft and poor cartilage integration. Platelet-rich plasma (PRP) and hyaluronic acid (HA) have been described has having the potential to improve results. The aim of this study was to evaluate the effect of PRP and HA on AOT in a rabbit model.
Methods
Thirty-six rabbits underwent bilateral knee AOT treated with either the biological adjunct (PRP, n = 12; HA, n = 12; PRP + HA, n = 12) or saline (control). PRP and HA were administered as an intra-articular injection. The rabbits were euthanized at 3, 6, or 12 weeks postoperatively. The graft sections were assessed using the modified International Cartilage Repair Society (ICRS) scoring system. The results from the PRP alone group is from previously published data.
Results
The mean modified ICRS histological score for the PRP-treated group was higher than its control (P = 0.002). The mean modified ICRS histological score for the HA-treated group showed no difference compared with its control (P = 0.142). The mean modified ICRS histological score for the PRP + HA–treated group was higher than its control (P = 0.006). There was no difference between the mean modified ICRS scores of the PRP- and the PRP + HA–treated grafts (P = 0.445).
Conclusion
PRP may decrease graft degradation and improve chondral integration in an animal model. In this model, the addition of HA was not synergistic for the parameters assessed. Level of Evidence. Basic science, Level V. Clinical Relevance. PRP can be used as an adjunct to AOT, which may decrease graft degeneration and improve clinical outcomes. HA may not influence AOT.
Introduction
Autologous osteochondral transplantation (AOT) is a surgical treatment for osteochondral lesions (OCL) that are large and/or cystic. The procedure involves removing an OCL and replacing it with an osteochondral autograft harvested from an available donor site.1-3 The clinical success of this procedure is well documented in the literature, particularly in weightbearing joints such as the ankle and knee.1-9 The procedure has also been shown to result in superior outcomes when compared with repeat arthroscopic bone marrow stimulation in OCLs of the talus that have failed a previous index procedure of bone marrow stimulation. 10 Furthermore, the scope of AOT for treating particularly large lesions, previously only amenable to salvage procedures, continues to expand. 11 While the clinical success of AOT for treating OCLs is promising, there are issues related to the biological ingrowth of the graft following the procedure.
The trauma of harvesting the graft, as well as placing it into the lesion site results in cartilage degeneration and loss of proteoglycan content.12,13 In addition, integration of the graft with the surrounding native tissue at the chondral interface has been shown to be incomplete. 8 These findings may contribute to poorer clinical outcomes in certain cases and may be attributable to the high rate of cyst formation seen following AOT.5,14 Because of these concerns, investigators have explored the potential to augment biologic integration and potentially improve outcomes following AOT.15-18
Two widely studied biological adjuncts used in cartilage repair are platelet-rich plasma (PRP) and hyaluronic acid (HA). PRP is an autologous blood product produced from the centrifugation of whole blood, resulting in a concentration of platelets greater than baseline level. 19 It has been proposed as a source of growth factors that may aid chondrogenic healing. 20 PRP may also encourage proteoglycan and type-II collagen deposition, as well as increase chondrocyte proliferation.21-24 HA, produced with varying molecular weights, has the potential to inhibit the activity of matrix metalloproteinases and catabolic cytokines, including interleukin-1.25-27
Our group has previously reported the effects of PRP on AOT in a rabbit model, concluding that PRP may improve integration of an osteochondral graft at the cartilage interface and decrease graft degeneration. 28 However, a comparison of the effects of PRP and HA on AOT repair has not been previously reported in the literature. Neither has previous investigative work assessed the potentially synergistic effects of combining PRP and HA. The aim of this study was to evaluate the effect of PRP and HA in isolation, as well as combined, on autologous osteochondral transplantation in a rabbit model. We hypothesized that PRP and HA would act synergistically and improve healing of a transplanted osteochondral graft accordingly by comparison with either adjunct alone.
Materials and Methods
Experimental Design
A rabbit model was selected for this study as the knee is sufficiently large to accommodate the surgical procedure and has been previously used as a model for AOT.17,29-31 Prior to commencing the study, approval was obtained from the Institutional Animal Care and Use Committee of our institution. A sample size calculation for the primary outcome of International Cartilage Repair Society (ICRS) histological score showed that 12 rabbits provided 88% power to detect a 2-point difference in score given a standard deviation of 2 points. Thus, 36 New Zealand White male rabbits with an average weight of 3.9 kg (range, 3.4-4.2 kg) were used, with 12 rabbits assigned to each treatment group, PRP, HA, and PRP + HA. The results from the PRP alone group have been previously published. 28
Each animal had an AOT performed on both knees, with the treatment (PRP, HA, or HA + PRP) assigned to the left or right knee using a computer-generated randomization schedule and the contralateral knee receiving an injection of saline and AOT (control).
Surgical Procedure
The protocol for PRP preparation and surgical technique for AOT has previously been described. 28 For the rabbits assigned to the PRP and PRP + HA group, 27 mL of blood was drawn from the great aural artery of each animal, and combined with 4 mL of anticoagulant (citrate dextrose solution A). For cytological analysis, one milliliter of blood was reserved in a separate syringe. The remaining blood was processed using a standard platelet concentration system according to the manufacturer’s protocol (Magellan Autologous Platelet Separator, Arteriocyte, Cleveland, OH) to yield 3 mL of PRP. One milliliter of the PRP was retained for cytological analysis and the remaining assigned to surgical use. No activation step was employed in this study.
Once both of the animal’s lower extremities were shaved, cleansed, and draped in a sterile fashion, bilateral 4-cm medial parapatellar incisions exposed the femoral condyles. A circular osteochondral defect measuring 2.7 mm in diameter and 5 mm in depth was created on a weightbearing segment of the lateral femoral condyle of the left knee using a drill. An osteochondral graft measuring 2.9 mm in diameter and 5 mm in depth was then harvested using a mosaicplasty harvester (Smith & Nephew, Memphis, TN) from the lateral femoral condyle of the right knee. Next, the osteochondral graft was press-fit into the defect created on the lateral femoral condyle of the left knee. Following this, an identical procedure was performed on the medial femoral condyles, with a defect created in the right knee and filled with a graft harvested from the left knee.
Prior to implantation, the grafts for the rabbits in the PRP and PRP + HA groups were randomized to be soaked in 1 mL of PRP or saline solution (control) for 10 minutes before press-fit placement in the osteochondral defect. For the HA group, the control graft alone was placed in the saline solution. At the time of graft placement, care was taken to ensure that the graft was placed in congruency with the surrounding native cartilage. The osteochondral graft donor sites were not backfilled.
The medial parapatellar arthrotomy was closed in layers with simple interrupted sutures (4-0 Vicryl; polyglactin; Ethicon, Johnson & Johnson), with skin closure performed using a running subcutaneous stitch (4-0 Vicryl). Following wound closure, knees that were randomized to PRP treatment (PRP and PRP + HA groups) received an intra-articular injection of 0.5 mL of PRP. Knees that were randomized to receive HA treatment (HA and PRP + HA) were administered 0.5 mL of HA (Durolane, Bioventus, Hoofddorp, the Netherlands) in an intra-articular injection. The knee was then moved through full range of motion to ensure there was no evidence of patella maltracking. The animals were allowed unrestricted cage activity postoperatively. The rabbits were euthanized with pentobarbital (100-150 mg/kg, intravenous) at 3, 6, and 12 weeks postoperatively, with 4 rabbits euthanized at each time point from each group.
Cytological Analysis
Whole blood and PRP samples underwent cytological analysis to determine platelet, white blood cell, and red blood cell counts.
Gross and Histological Processing and Scoring
Scoring was performed by 2 blinded reviewers. The ICRS macroscopic scoring system was used to assess all gross specimens. 32
The technique used for specimen preparation for histological processing has been previously reported. 28 Samples were stained with hematoxylin and eosin for modified ICRS histological scoring. The histological score was assessed on a scale of 0 to 21, with a modification to assess cartilage integration at the graft-native tissue interface. 33 Sections were additionally stained with alcian blue to determine glycosaminoglycan content and were processed for type-II collagen immunohistochemistry.
Statistical Analysis
The Shapiro-Wilk statistic was used to examine normality of all variables of interest prior to analysis. This test indicated that the data was not normally distributed and therefore continuous variables were evaluated using the Wilcoxon sign-rank test. Using a nonparametric statistical test allowed for a more conservative and appropriate estimate of the statistical significance of the results given the small sample size.
The Kruskal-Wallis test was used to test for differences in macroscopic and histological scores at each time point. All analyses were performed using SAS Software version 9.2 (SAS Institute, Cary, NC).
An analysis of the data collected from the subset of rabbits receiving PRP in isolation was published separately and the data from that publication is presented again in this study for comparison with results from the HA in isolation and PRP + HA groups. 28
Results
All surgical procedures were completed without perioperative complication. No rabbit experienced a postoperative complication, including, but not limited to, infection, lameness, and wound dehiscence.
Cytological Analysis
Cytological analysis for a subset of the animals used in this study has been published previously and are included as such in the following data. The PRP produced in our study showed a 6-fold increase in platelet count compared to whole blood (mean and standard deviation, 932.9 ± 360.2 vs. 154.9 ± 66.2, P < 0.001). The red blood cell count in the PRP was less than a third of that of the whole blood (6.9 ± 4.1 vs. 22.1 ± 16.0, P < 0.001). The white blood cell count was over 2-fold higher in the PRP compared with whole blood (11.4 ± 3.5 vs. 4.6 ± 1.4, P < 0.001).
Macroscopic and Histological Appearance of the Graft
All rabbits were euthanized at 3, 6, and 12 weeks postoperatively and the knees resected as a whole. Macroscopic assessment showed a mean score of 11.2 ± 0.9 in the PRP-treated group versus 10.3 ± 0.9 in the control group (P = 0.09). 2 The HA group showed a mean macroscopic score of 10.3 ± 0.9 versus 10.0 ± 0.6 in the control group (P = 0.27). The PRP + HA group demonstrated a mean macroscopic score of 10.25 ± 0.6 versus a control group score of 10.1 ± 0.8 (P = 0.44). Subjectively, it was noted that all grafts were at the level of the surrounding native cartilage with no significant step-off appreciated. The PRP- and PRP + HA–treated grafts appeared to show less evidence of a well-demarcated border surrounding the osteochondral transplant and fewer grossly visible fissures.
The mean modified ICRS histological score in the PRP treated group was 18.2 ± 2.7 versus 13.5 ± 3.3 in the control group (P = 0.002). 28 The mean histological score in the HA-treated group was 15.9 ± 2.9 compared with a control group score of 14.5 ± 3.6 (P = 0.15). The mean histological score in the PRP + HA–treated group was 17.9 ± 2.6, versus 14.0 ± 3.3 in the control group (P = 0.004). With regard to the osteochondral graft integration assessment specifically, the PRP and PRP + HA treatment groups showed improvement (2.5 ± 0.9 vs. 1.6 ± 0.7; P = 0.004 and 2.2 ± 0.8 vs. 1.5 ± 0.5; P = 0.01). 28 There was no difference in osteochondral graft integration between the HA-treated grafts and the controls (1.8 ± 0.8 vs. 1.8 ± 0.7; P = 1) ( Fig. 1 ).
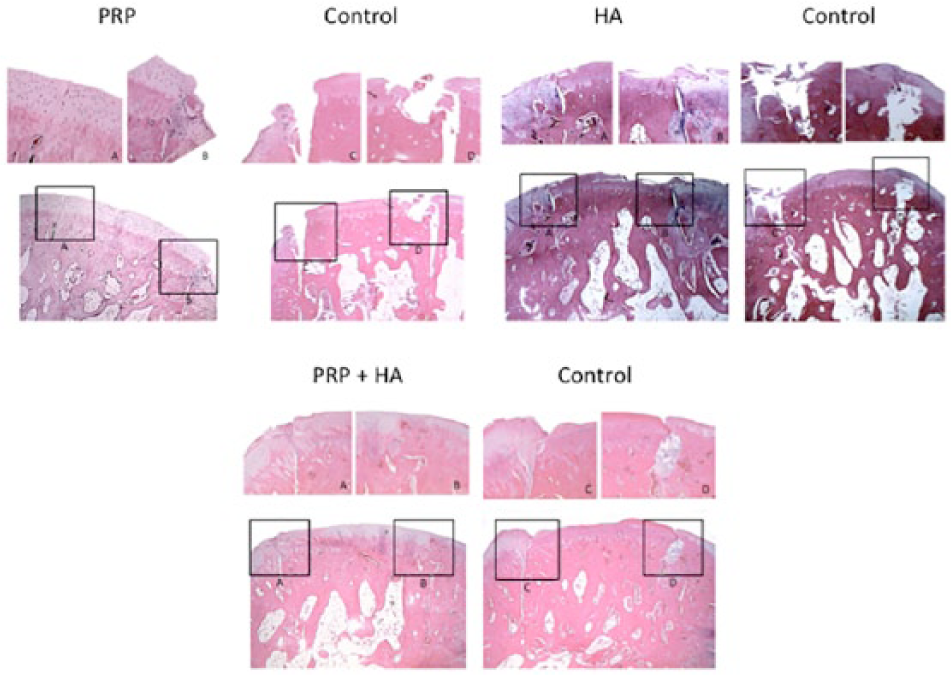
Sagittal sections of osteochondral grafts at 12 weeks following surgery. The top row images are magnified 200×, and the bottom row images are magnified 20×. PRP, platelet-rich plasma; HA, hyaluronic acid.
The PRP- and PRP + HA–treated grafts showed increased glycosaminoglycan content, indicated by greater alcian blue staining at the cartilaginous portion of the graft. Greater glycosaminoglycan content was also noted at the interface of the graft and native tissue. The same was not seen in the HA treated grafts compared with the controls. The PRP- and PRP + HA–treated groups also demonstrated increased reactivity to type-II collagen when compared with the controls. This was evident at both the cartilage cap of the graft and at the borders of the graft and native tissue interface. There was no noticeable difference in type-II collagen immunoreaction between the HA treated grafts and the controls ( Fig. 2 ).
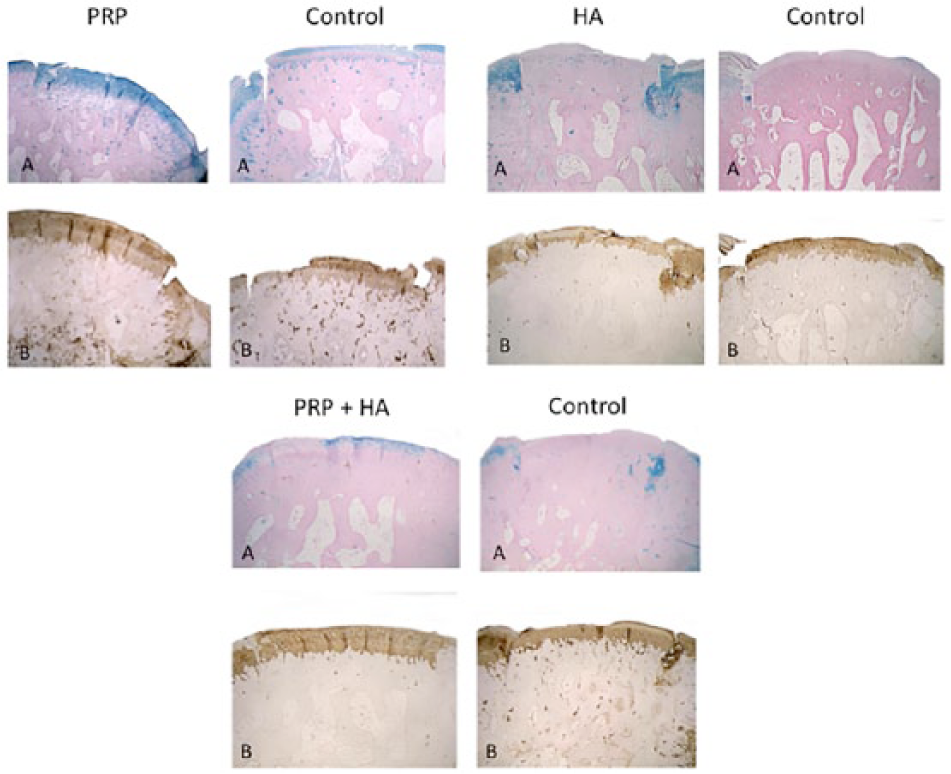
Sagittal sections of osteochondral grafts at 12 weeks following surgery. Glycosaminoglycan content was assessed using alcian blue staining (labeled A), and type-II collagen content was assessed using type-II collagen immunohistochemistry (labeled B). The images are magnified 20×. PRP, platelet-rich plasma; HA, hyaluronic acid.
Discussion
The results of this study did not detect a synergistic effect of PRP + HA when used as a combination of adjuncts with autologous osteochondral transplantation. Statistically significant improvements were found in the overall histological appearance of the osteochondral grafts in both the PRP and PRP + HA treatment groups, with no difference between those groups. However, there was no significant improvement seen in the HA treatment group when compared with the controls. The same results were seen when specifically assessing osteochondral graft integration. Therefore, PRP appeared to allow for an improvement in the histological appearance of the graft, with no further improvement seen with the addition of HA. The principal difference seen between the groups was at the cartilage level. With regard to the subchondral bone, little difference was seen between the groups, with the majority showing good integration and viability at the osseous level. This is as expected considering that the bone that was transplanted was a healthy autologous graft.
PRP and HA have been assessed as adjuncts to the management of cartilage pathology, with numerous in vitro and in vivo studies published in the literature.21-27 PRP has been shown to have multiple effects, which may explain the results seen in this study. These effects may be divided into anabolic and anticatabolic categories. The anabolic effects of PRP described previously include increased chondrocyte viability and proliferation, as well as increased proteoglycan deposition and type-II collagen content.21,24,34-36 Furthermore, Mishra et al. 22 demonstrated in a cell culture model that PRP increases migration of mesenchymal stem cells and their expression of chondrogenic markers such as Sox-9 and aggrecan. This is particularly relevant to AOT, as when the OCL is cored out it leaves bleeding subchondral bone, thus recruiting subchondral derived mesenchymal stem cells to the graft site. The amalgamation of these anabolic effects may lead to an increased quantity and quality of cartilage repair following AOT.
The anticatabolic effects of PRP have also been described in the literature. Catabolic cytokines such as interleukin-1 (IL-1) and tumor necrosis factor–α (TNF-α) are elevated in the presence of cartilage pathology.37,38 Furthermore, mechanical stress on chondrocytes, such as that applied to the joint during explantation and implantation of an osteochondral graft, leads to the release of matrix metalloproteinases (MMPs). 39 Basic science evidence has shown that PRP may mediate the effect of these catabolic cytokines, with evidence showing that it may lead to decreased IL-1- and MMP-mediated inhibition of type-II collagen and aggrecan gene expression.34,40
The anticatabolic effects of HA are also described in previous studies.41-43 In vitro evidence has shown that HA may downregulate synovial expression of MMPs produced in the presence of cartilage pathology. 41 This allows for a chondroprotective effect, with Greenberg et al. 44 concluding that HA inhibits the MMP- and IL-1-mediated decrease in glycosaminoglycan production by cartilage explants. These findings have been translated to the in vivo literature, with Elmorsy et al. 45 demonstrating that HA produced a statistically significant decrease in the histological damage to cartilage seen in a rabbit osteoarthritis model.
The current study demonstrated that PRP alone produced an improvement in the histological appearance of the graft. One possible hypothesis for this is that PRP produces both an anabolic and anticatabolic effect within the joint environment, versus the principally chondroprotective effect of HA. Recently, Sundman et al. 46 came to a similar conclusion when comparing HA and PRP in an in vitro model. The authors demonstrated that while both PRP and HA decreased TNF-α, a well-known mediator of acute inflammation in cartilage pathology, PRP decreased MMP-13 expression to a greater extent. Furthermore, PRP increased cartilage expression of the chondrogenic marker aggrecan. The same authors also showed that PRP exerted an influence on synoviocytes, increasing the production of hyaluronan synthase-2, a marker for hyaluronan production. It is likely that the combination of both the anabolic and anticatabolic effects of PRP versus the principally anticatabolic role of HA is responsible for the results seen in this study. It is important to note that there have been mixed results reported in the literature with regard to osteochondral healing supplemented by PRP. As an example, Altan et al. 47 reported on the results of using the mosaicplasty procedure and PRP versus mosaicplasty alone in a rabbit model. The authors reported that the addition of PRP improved osteochondral healing as the histological level. However, adding PRP to any technique of osteochondral repair does not appear to improve outcomes. van Bergen et al. 48 tested the effect of PRP in conjunction with demineralized bone matrix for osteochondral lesions in a goat model. They concluded that there was no significant difference seen in osteochondral healing with the addition of PRP. Furthermore, PRP has also been shown to be potentially detrimental to osteochondral healing when used in conjunction with a collagen-hydroxyapatite scaffold. 49
The limitations of this investigation include the use of an AOT to treat an acutely created osteochondral defect. In clinical practice, AOT is predominately employed to treat chronic OCLs. 50 The joint environment is invariably different between the two and therefore the results in this study may differ from those seen in clinical practice. Furthermore, the rabbits were sacrificed at 3 different time points. The purpose of this was to evaluate the changes of healing at different time points. This was done in the event that there were only changes to be seen early or late in the osteochondral healing process. However, this does lead to grouping all 3 times points into the results. In addition, contrasting results may be seen with varying formulations of PRP. Assessing the “ideal” formulation of PRP with regard to joint pathology is the focus of the more recently published literature, with currently no consensus available. Cavallo et al. 51 demonstrated how PRP may be produced with fewer leukocytes, and consequently lower platelet levels, or with increased leukocytes and therefore higher platelet counts. The authors showed that the differing formulations produced varying effects in vitro, with leukocyte-poor PRP (P-PRP) causing a greater expression of type-II collagen and aggrecan, and leukocyte-rich PRP (L-PRP) inducing greater HA production. Favoring P-PRP, Yin et al. 52 published the results of using the biological adjunct in a rabbit osteoarthritis model. The authors found that P-PRP decreased cartilage destruction and reduced IL-1 and PGE2 to a greater extent than L-PRP. However, Carmona et al. 53 in a study evaluating varying concentrations of L-PRP and P-PRP in a co-culture with equine cartilage explants published contrasting results. In their study, the authors showed that L-PRP exhibited the greatest anti-inflammatory and anabolic effect. To further add to the variability seen in the literature, the effect of PRP on synoviocytes must also be examined as cartilage does not exist in isolation within the joint. Assirelli et al. 54 cultured human osteoarthritic synoviocytes with L-PRP and P-PRP. The findings demonstrated that L-PRP upregulated the production of IL-1 and IL-8, resulting in a potentially greater pro-inflammatory environment. Similar conclusions were reached by a separate study assessing PRP and human synoviocytes, determining that L-PRP may additionally increase synoviocyte death. 55
A similar problem is found when using HA, with a multitude of commercially available products of varying molecular weights and half-lives. As an example, in a study comparing 2 HA formulations on an IL-1 treated cartilage-synovium co-culture, Greenberg et al. 44 found that while one HA product allowed for increased glycosaminoglycan content, the other decreased MMP concentrations. Therefore, depending on the equipment used, resulting in different formulations of PRP,56,57 and choice of HA product, varying results may be expected both in the literature and in clinical practice.
With regard to the biological adjuncts used in this study, the literature is unclear as to whether leukocyte-rich PRP (L-PRP) pure PRP (P-PRP) is optimal for osteochondral healing. Depending on the PRP preparation used, varying concentration of growth factors are expressed. Increased levels of platelet-derived growth factor and vascular endothelial growth factor are shown in L-PRP, while transforming growth factor and fibroblast growth factor are elevated in P-PRP. 57 The difference in concentrations of anti-inflammatory markers between leukocyte-rich PRP and leukocyte-poor PRP have also been studied, with Osterman et al. 58 reporting no difference between the two PRP preparations in a human osteoarthritis model. Therefore we believe that using a PRP formulation that neither extensively depleted nor concentrated the leukocytes would be best served in the current study. The formulation of PRP used in this study reflects these cytological characteristics. 59 Furthermore, the reason for using the HA product chosen in this study was its extensive half-life, which has been described as 32 days. 60 This allowed for a singular intra-articular injection at the time of surgery, rather than subjecting the rabbits to multiple injections postoperatively.
In conclusion, the findings of this study demonstrate that following AOT, PRP may decrease graft degradation and improve chondral integration in an animal model. In this model, the addition of HA was not synergistic for the parameters assessed.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded through educational grants from the Ohnell Family Foundation, Mr. and Mrs. Michael J. Levitt, and Arteriocyte, Inc. All funding was donated directly to the Hospital for Special Surgery. The funding was used for supplies and animal costs, and no author received any direct financial benefit from this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Institutional Animal Care and Use Committee of our institution.
Animal Welfare
The present study followed international, national, and/or institutional guidelines for humane animal treatment and complied with relevant legislation.