
Abstract
Objective
Bone marrow stimulation surgeries are frequent in the treatment of cartilage lesions. Autologous chondrocyte implantation (ACI) may be performed after failed microfracture surgery. Alterations to subchondral bone as intralesional osteophytes are commonly seen after previous microfracture and removed during ACI. There have been no reports on potential recurrence. Our purpose was to evaluate the incidence of intralesional osteophyte development in 2 cohorts: existing intralesional osteophytes and without intralesional osteophytes at the time of ACI.
Study Design
We identified 87 patients (157 lesions) with intralesional osteophytes among a cohort of 497 ACI patients. Osteophyte regrowth was analyzed on magnetic resonance imaging and categorized as small or large (less or more than 50% of the cartilage thickness). Twenty patients (24 defects) without intralesional osteophytes at the time of ACI acted as control.
Results
Osteophyte regrowth was observed in 39.5% of lesions (34.4% of small osteophytes and 5.1% of large osteophytes). In subgroup analyses, regrowth was observed in 45.8% of periosteal-covered defects and in 18.9% of collagen membrane–covered defects. Large osteophyte regrowth occurred in less than 5% in either group. Periosteal defects showed a significantly higher incidence for regrowth of small osteophytes. In the control group, intralesional osteophytes developed in 16.7% of the lesions.
Conclusions
Even though intralesional osteophytes may regrow after removal during ACI, most of them are small. Small osteophyte regrowth occurs almost twice in periosteum-covered ACI. Large osteophytes occur only in 5% of patients. Intralesional osteophyte formation is not significantly different in preexisting intralesional osteophytes and control groups.
Introduction
Articular cartilage defects that do not involve the subchondral bone have limited to no spontaneous repair potential and can result in symptoms equivalent to those seen in severe osteoarthritis.1,2 Several techniques are being utilized to address symptomatic defects with the goal of restoring joint function with a durable tissue regenerate. Marrow stimulation techniques such as drilling, abrasion arthroplasty, or microfracture are frequent first-line treatment options for symptomatic small to medium cartilage defects of the knee. 3 These techniques attempt to induce a reparative tissue through stimulation of the subchondral bone at the bottom of the defect. 4 Blood and mesenchymal cells from the underlying marrow cavity form a clot in the defect that gradually differentiates into a fibrocartilaginous repair tissue. 5 Conversely, autologous chondrocyte implantation (ACI) transfers ex vivo cultured chondrocytes into the defect and may be performed as primary treatment in larger lesions, as well as to revise failed prior procedures. 6
Recently, there has been increasing interest in the importance of the subchondral bone, and growing recognition that this structure is intimately involved in the development and natural history of articular cartilage damage. As such, it can be expected to be an important factor in the outcome of cartilage repair procedures and in the determination of the patients’ prognosis. 7 As our understanding of the underlying pathophysiological changes grows, cartilage damage and osteoarthritis has evolved into a disease of the osteochondral unit and entire joint rather than a disorder limited to the articular cartilage. It is becoming apparent that without support from an intact subchondral bed, any treatment of the surface chondral lesion is more likely to fail. 7 Injury to the subchondral plate or calcified cartilage is thought to trigger reactivation of the secondary center of ossification, leading to thickening of the subchondral plate and calcified cartilage, and causing the tidemark to advance with corresponding thinning of the overlying cartilage.8-10
Recent studies have demonstrated subchondral bone changes in 30% to 50% of patients treated with microfracture, such as sclerosis, subchondral cysts, and osseous overgrowth resulting in the formation of intralesional osteophytes,3,11-14 which may be among the factors causing increased failure of ACI after prior microfracture.14,15
It has been recommended that these intralesional osteophytes be removed during revision with ACI to thin out the thickened subchondral plate, both to mechanically reduce the pathologically elevated stiffness as well as to simply create space in the defect for the regenerative tissue. 14 The authors had noticed regrowth of bone previously removed for notchplasty during ACL reconstructive surgery, raising concerns that osteophytes might recur as well. There have been no specific studies on the recurrence of intralesional osteophytes to determine the utility of removal during ACI surgery.
The purpose of this study was to review the incidence of intralesional osteophyte development in 2 cohorts of patients: those who had existing intralesional osteophytes removed during ACI and those who presented without intralesional osteophytes at the time of ACI. We hypothesized that intralesional osteophytes removed during ACI surgery would not regrow.
Methods
Demographics
All patients enrolled in this study provided prior written consent for inclusion in our center’s institutional review board–approved cartilage repair database.
A total of 497 patients underwent ACI surgery between June 1995 and December 2008. The general indications for ACI were followed as published elsewhere in greater detail: symptomatic, large full-thickness chondral defects of the knee that had failed nonoperative measures and prior surgical intervention with debridement or bone marrow stimulation techniques.6,16 Among this group, 165 patients were treated for intralesional osteophytes at the time of ACI, of which 87 patients underwent postoperative magnetic resonance imaging (MRI) at more than 1-year follow-up ( Table 1 ). Data from these 87 patients (53 males and 34 females) were analyzed for osteophyte regrowth after prior removal ( Figs. 1 - 4 ). A separate group of 20 patients without intralesional osteophytes at the time of ACI were selected as a control group; all of these patients underwent a routine postoperative MRI at a minimum of 12 months.
Patient Demographics.
ACI = autologous chondrocyte implantation; pACI = periosteal ACI; cACI = collagen membrane ACI.
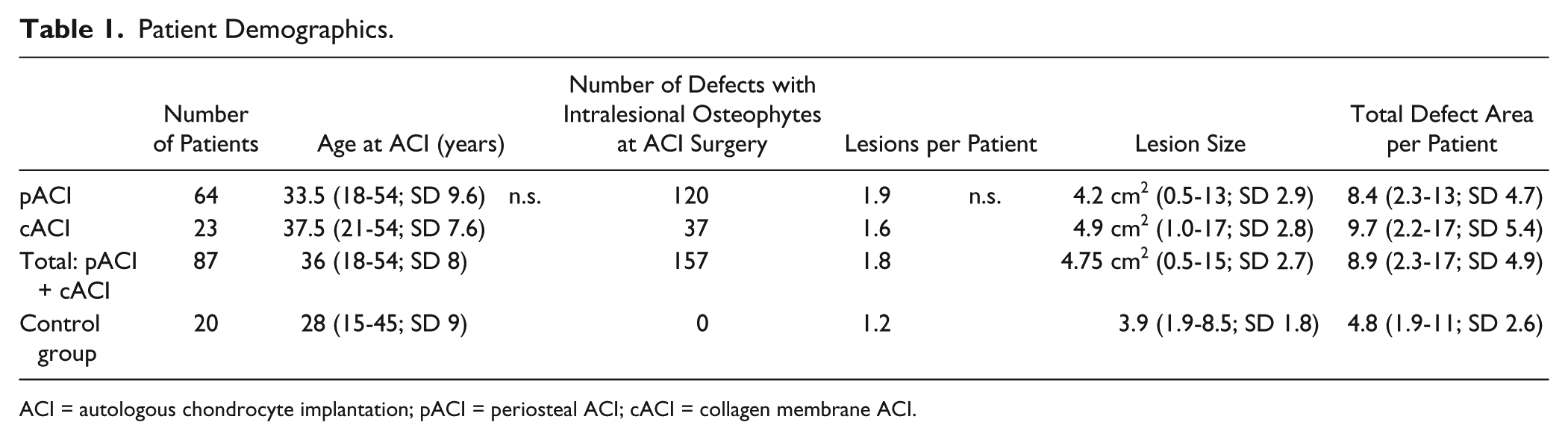
Intralesional osteophyte observed during surgery (
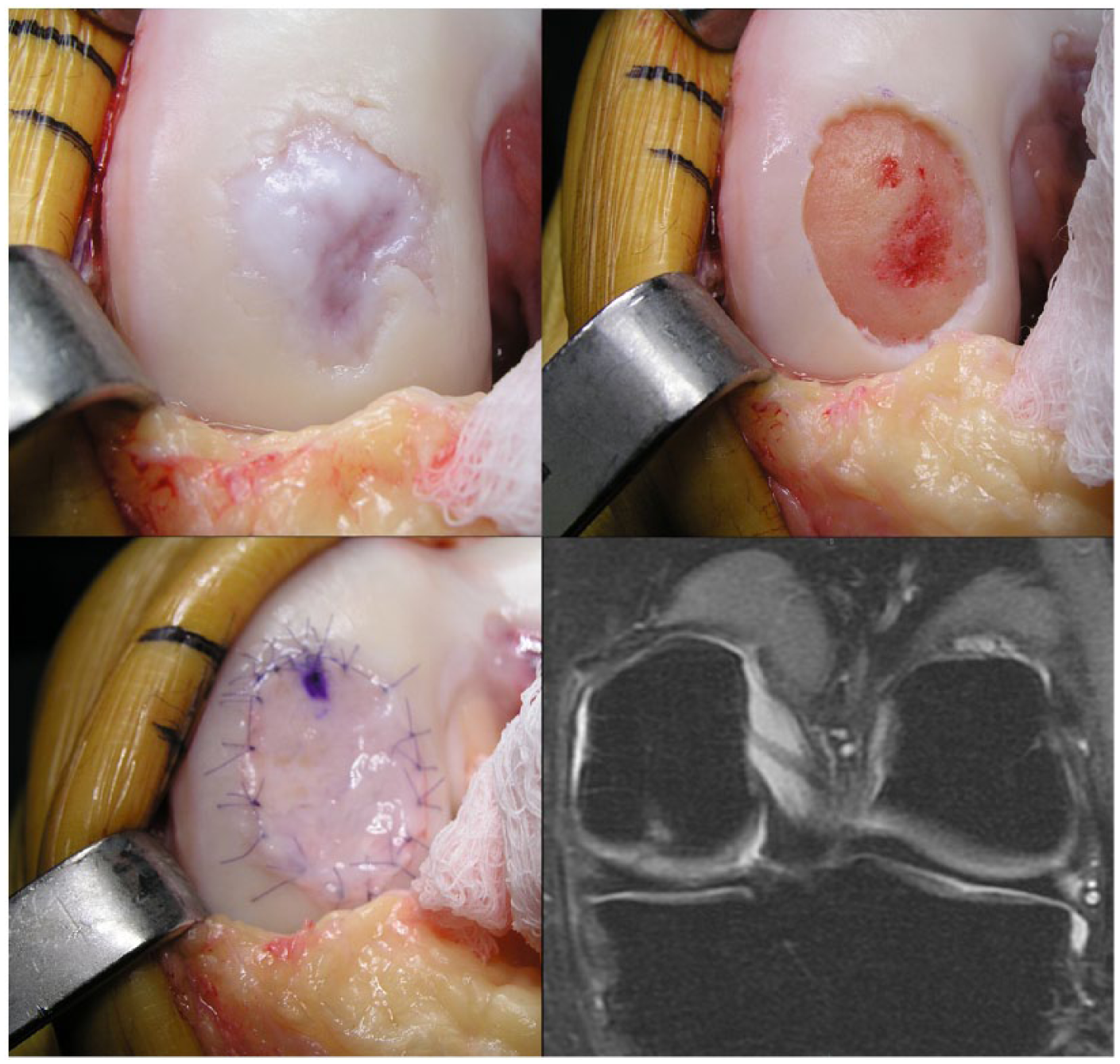
Intralesional osteophyte observed during surgery (
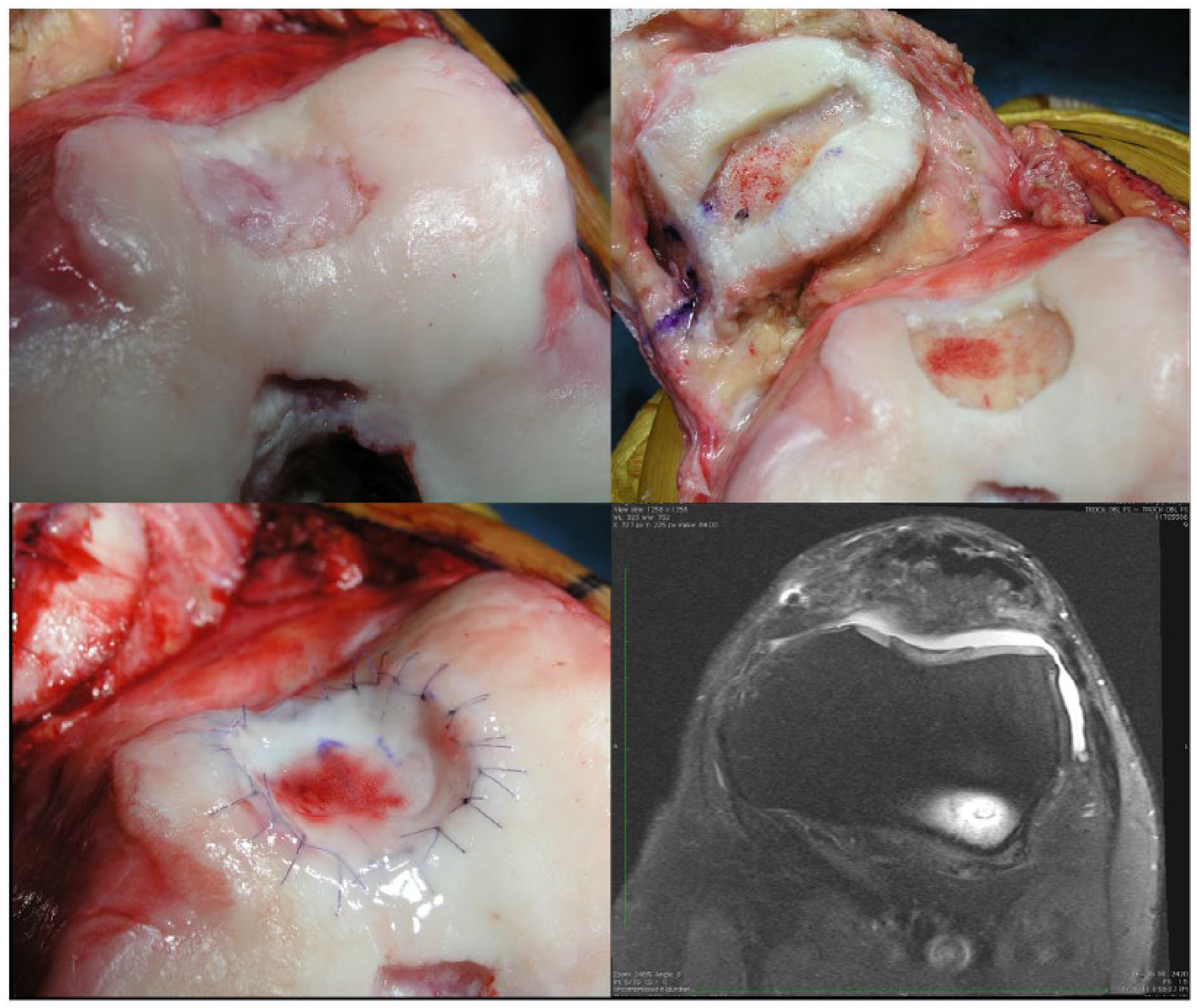
Intralesional osteophyte observed during surgery (
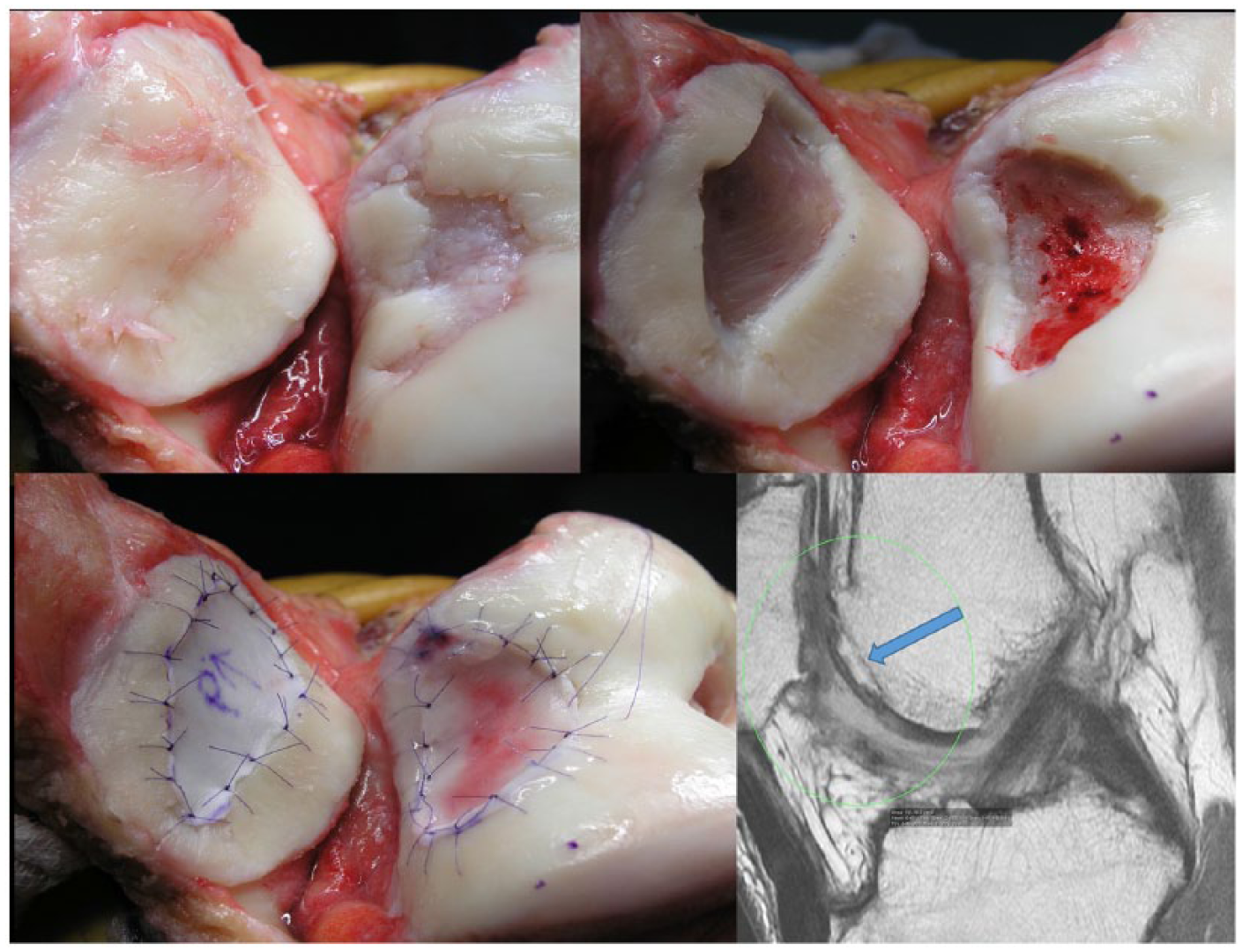
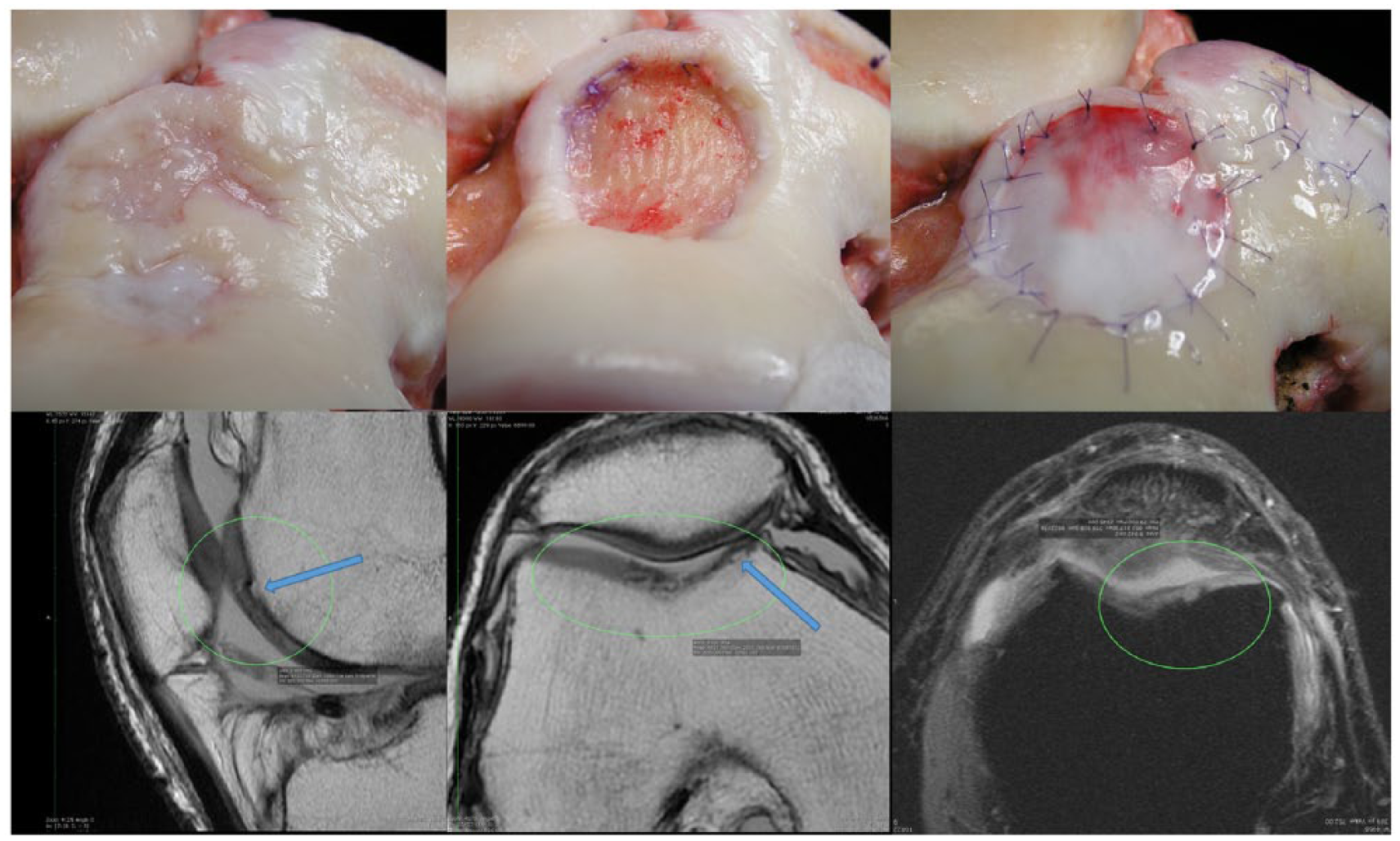
Intralesional osteophyte observed during surgery (
Osteophyte regrowth was categorized into 2 types: “small” when osteophytes regrew to less than 50% of the thickness of surrounding cartilage ( Fig. 3 ), or “large” when osteophytes exceeded more than 50% of the cartilage thickness ( Fig. 4 ). Intralesional osteophyte measurement was performed with MRI using Osirix Imaging Software (Advanced Open Source PACS Workstation DICOM Viewer, Pixmeo SARL). Two orthopedic surgeons with experience in cartilage repair and musculoskeletal MRI evaluation performed all measurements. In case of nonagreement regarding the osteophyte category, a third observer would decide.
Surgical Technique
The details of the ACI procedure have been described previously in greater detail. 17 In summary, autologous chondrocytes were expanded in cell culture from a cartilage biopsy harvested arthroscopically (Carticel, Genzyme Bio Surgery/Vericel, Cambridge, MA). In a second procedure, the cartilage defects were prepared by outlining all degenerated tissue with a fresh scalpel blade; then removing the tissue with a curette, including the layer of calcified cartilage, being mindful not to injure the subchondral plate by exerting excessive pressure. Intralesional osteophytes encountered during the debridement were removed with use of a high-speed bur under constant cold irrigation to avoid overheating the bone ( Fig. 5 ) Excess bone was burred down to the level of the surrounding, normal subchondral plate. Bleeding from the bone is generally minimal, provided care is taken not to extend the resection past the subchondral plate into the subchondral bone. Any existing bleeding is easily addressed with fibrin glue.
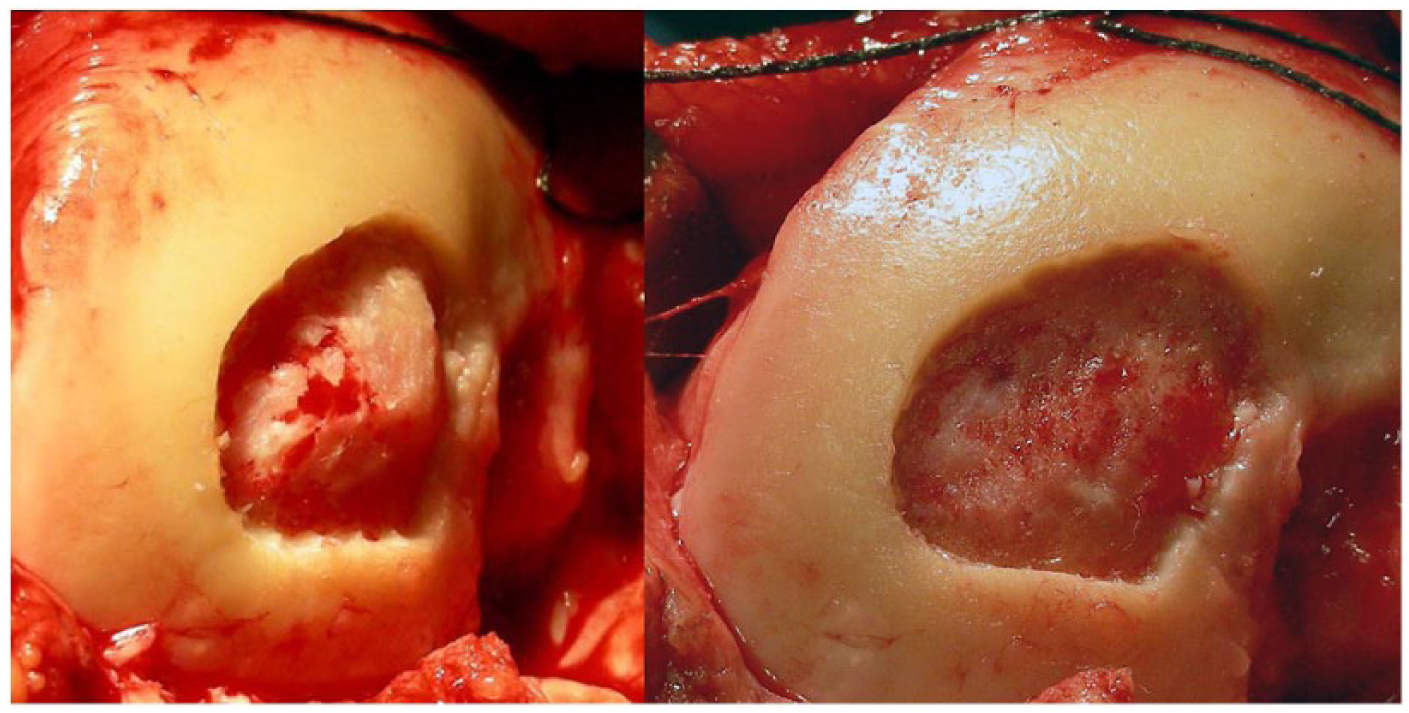
Intralesional osteophyte (
A periosteal patch harvested from the proximal tibia or a collagen membrane was then secured with resorbable sutures and fibrin glue (Tisseal, Baxter Biosurgery, Deerfield, IL) sealant. Periosteum ( Fig. 1 ) was used until May 2007, and a type-I/III porcine collagen-membrane (BioGide, Geistlich Pharma, Wolhusen, Switzerland) since then 18 ( Fig. 2 ). This membrane is derived from porcine peritoneum and resorbs within a few months of implantation. It is currently Food and Drug Administration approved in the United States only for dental applications; the use for ACI is off-label. After patch fixation, cultured autologous chondrocytes were then injected underneath the patch at an approximate density of 1 M cells per cm2.
Articular comorbidities such as malalignment, patellar maltracking, and meniscal or ligamentous deficiency were corrected in a staged or concurrent procedure.
Statistical Analyses
We performed descriptive analyses of the data. In order to compare subgroups we performed a chi-square test for the categorical data.
Results
Intralesional Osteophyte Group
Eighty-seven patients with 157 cartilage defects were treated with removal of intralesional osteophytes during ACI surgery. The mean age at implantation was 36 years (range 18-54 years; SD 8). There were no statistically significant differences between age or defect size for the 2 subgroups (periosteal patch–covered ACI [pACI] vs. collagen membrane–covered ACI [cACI]). The average size of the cartilage defect was 4.8 cm2 per defect (range 0.5-15 cm2; SD 2.7). Sixty-four patients (120 defects) were treated with periosteal patch–covered ACI (pACI) and 23 patients (37 defects) with collagen membrane–covered ACI (cACI).
Overall, osteophyte regrowth was observed in 62 lesions (39.5%) or 29 patients (33.3%). In the pACI group, osteophyte regrowth was observed in 55 lesions (45.8%) or 23 patients (35.9%). In the cACI group, osteophyte regrowth was observed in 7 lesions (18.9%) or 6 patients (26.1%). Comparing both groups, pACI showed a higher incidence of osteophyte regrowth (P < 0.01) ( Table 2 ). There was no disagreement regarding the osteophyte regrowth category among the 2 independent evaluators.
Intralesional Osteophyte Regrowth.
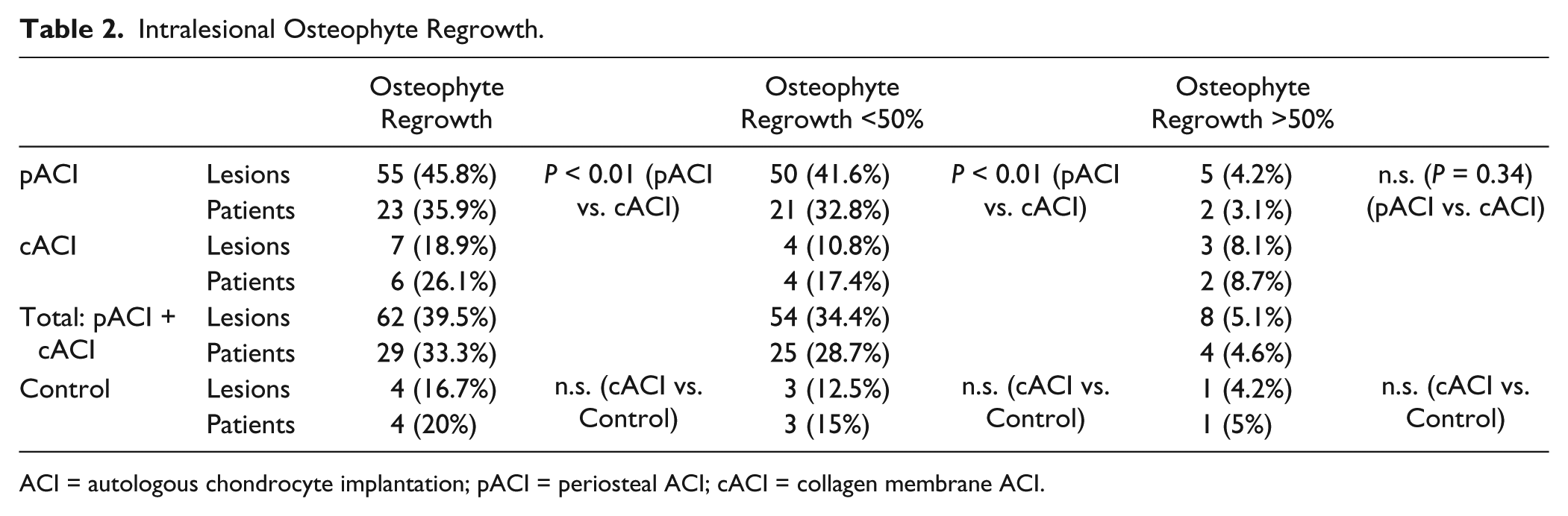
ACI = autologous chondrocyte implantation; pACI = periosteal ACI; cACI = collagen membrane ACI.
Further categorizing osteophyte regrowth based on size, small osteophyte regrowth was observed in 54 lesions (34.4%) or 25 patients (28.7%) overall. Small osteophyte regrowth was observed in 50 lesions (41.6%) or 21 patients (32.8%) in the pACI group, and in 4 lesions (10.8%) or 4 patients (17.4%) in the cACI group. Comparing both groups, pACI showed a higher incidence of small osteophyte regrowth (P < 0.01) ( Table 2 ).
Large osteophyte regrowth was observed in 8 lesion (5.1%) defects or 4 patients (4.6%) overall. Large osteophyte regrowth was observed in 5 lesions (4.2%) or 2 patients (3.1%) of pACI patients, and in 3 lesions (8.1%) or 2 patients (8.7%) of the cACI patients. There were no statistically significant differences among both groups ( Table 2 ).
Among the 157 lesions we could identify 5 cases where bone grafting was performed in a sandwich technique. 19 In this subgroup, only one case showed osteophyte regrowth, being smaller than 50% of the cartilage depth.
We observed 7 patients (8%) with ACI failures in this group. Among the failure patients there were 2 patients with 2 lesions that demonstrated osteophyte regrowth: one large and one small recurrence. There were too few failures to perform a meaningful statistical analysis of whether there was any correlation between osteophyte regrowth and failure.
Control Group
Twenty patients (24 defects) without intralesional osteophytes acted as control: the average defect size was 3.9 cm2 (range 1.9-8.5 cm2; SD 1.8). The average age at implantation was 28 years (range 15-45 years; SD 9). There were no significant differences between the groups with and without intralesional osteophytes regarding average defect size and age. All control group patients were treated with collagen covered ACI (cACI).
Intralesional osteophytes developed in 4 defects (16.7%) in 4 patients (20%): 3 small osteophytes (12.5%) and 1 large osteophyte (4.2%) were observed (15% and 5% of patients, respectively). There were no statistically significant differences in osteophyte incidence between cACI patients with and without intralesional osteophytes removed during prior ACI surgery. One patient (5%) in the control group failed ACI; no osteophyte was seen in this patient.
Discussion
Our study demonstrates that although there is a significant number of intralesional osteophytes that regrow after prior surgical removal during ACI surgery, this rate is not significantly different than that seen in patients without preexisting intralesional osteophytes, provided a collagen membrane is used during ACI (cACI). To our knowledge this is the first large prospective cohort investigating osteophyte regrowth after prior removal during ACI.
Most of the preexisting intralesional osteophytes in our series were due to previous marrow stimulation procedures. Previous studies demonstrated that ACI surgeries after previous bone marrow stimulation procedures lead to higher failure rate of ACI.14,15 We believe that damage to subchondral bone may cause permanent histological changes and may lead to recurrent intralesional osteophyte formation. However, with the current data we could not demonstrate whether osteophyte recurrence affects long-time survival of ACI procedures. Several studies have demonstrated an up to 50% incidence of subchondral changes, such as intralesional osteophytes, after microfracture or bone marrow stimulation procedures.3,13,20 Animal studies also have demonstrated a high incidence of subchondral bone cysts after microfracture procedures. 21 The ACI procedure has also been reported to result in changes of the subchondral plate, albeit at a lower rate than microfracture (25% vs. 51.5%). 22 Finite element analysis models have suggested that subchondral stiffening and stress concentration may cause an elevation in shear stresses in the deep cartilage layers.23,24 If intralesional osteophytes are present, the thinner layer of viscoelastic cartilage overlies a thickened and stiffened subchondral plate and is therefore more susceptible to damage from shear forces. We believe that microburring to remove the stiffened subchondral bone under copious cold irrigation is the best method to address intralesional osteophytes during surgery. Prior techniques included tamping the osteophyte down into the subchondral bone using a bone tamp, or debriding the osteophyte with a rangeur.
Although we observed that intralesional osteophyte regrowth occurs in approximately one third of patients, the incidence of osteophytes larger than 50% of the cartilage thickness was low (5.1%). We could not identify any correlation between osteophyte regrowth and ACI failure. Long-term clinical results seem to be more related to the type of cartilage defect, complexity of the defect, and whether a microfracture had been performed. 16 Therefore, we currently do not change our rehabilitation or physical restrictions in the presence of intralesional osteophyte removal, but we also believe that this question is not yet conclusively answered.
Previous studies have demonstrated that 25.7% of patients treated with periosteal-covered autologous chondrocyte require reoperation for hypertrophy of the graft or covering membrane compared to only 5% of patients after collagen membrane–covered ACI. 18 The use of a collagen membrane, rather than periosteum, for ACI also offers the benefit of a lowered incidence of osteophyte regrowth, an unsurprising finding given the role of periosteum in bone growth and healing.
Our study has limitations: MRIs were obtained at various time points between 1 and 3 years postoperative, with a majority between 12 and 18 months. Furthermore, this study was a nonrandomized cohort study rather than a randomized clinical trial, which would not have been feasible given the specific research topic. 25 Also, several patients who underwent surgery during the time of this cohort could not be included in this research due to lack of follow-up MRI. Finally, we have not evaluated subjective outcomes for patients in each group.
Conclusion
Small osteophyte regrowth after prior removal occurs in approximately 17% of patients treated with collagen-covered ACI, with almost twice that rate in periosteum-covered ACI. Large osteophytes occur only in 5% of patients regardless of which patch material was used. Surprisingly, the incidence of intralesional osteophyte formation is not significantly different between cohorts of patients with and without preexisting intralesional osteophytes at the time of ACI. Intralesional osteophytes therefore do not appear to be a contra-indication for ACI.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Partners Human Research Committee (APPROVAL NUMBER/ID: 2007P000470/BWH).
Informed Consent
Written informed consent was obtained from all subjects before the study.