
Abstract
Objective
To compare characteristics for patients scheduled for autologous chondrocyte implantation with matrix-assisted chondrocyte implantation (MACI) with those enrolled in clinical trials and to describe differences in patient selection between countries.
Design
Anonymized data from patients scheduled for MACI treatment in the knee in Europe and Australia/Asia were obtained from the Genzyme/Sanofi database. Average age, defect size, and male-female ratio were analyzed and compared by country. Clinical cohort studies and prospective comparative trials using autologous chondrocyte implantation and related treatments were identified and weighted average age, weighted defect size, and male-female ratio were analyzed and compared with data from the database.
Results
From the database 2,690 patients were included with mean age 33.7 years and male-female ratio of 67:33. Mean defect size was 5.64 cm2 and 70% of the defects were 3 to 10 cm2. There were significant differences between patients’ mean defect sizes between countries. Sixty-nine studies (57 cohorts and 12 prospective comparative trials) with a total of 5,449 patients were identified. The combined weighted mean age was 34.2 years, and the combined weighted mean defect size was 4.89 cm2. Patients scheduled for MACI had significantly larger defects that those included in clinical trials. There was no significant difference in age. No differences were found between cohorts and prospective comparative trials.
Conclusion
The vast majority of patients scheduled for autologous chondrocyte implantation with MACI have chondral defect comparable to that generally recommended, but differences exist between countries. Patients enrolled in clinical trials have significantly smaller defects than those undergoing treatment outside controlled trials.
Introduction
Matrix-assisted chondrocyte implantation (MACI) is a commercially available third-generation autologous chondrocyte implantation (ACI) technique for the treatment of articular cartilage defects. Established treatment algorithms generally agree on the use of microfracture or osteochondral autograft transfer (OAT) as first-line treatment for smaller defects (<3 cm2) of the femoral condyles. The indication for MACI and other ACI techniques has generally been limited to larger focal chondral defects (>3-4 cm2) of the knee, mostly due to the expense of these procedures. Several studies have demonstrated superiority of ACI in larger defects,1,2 confirming recommendations for the use of ACI in this population; alternatively, osteochondral allograft transplantation (OCA) can be considered but is not readily available in many countries. Despite general agreement on these algorithms, they have never been validated nor has surgical adherence to their suggestions been demonstrated.
The 4 original studies by Brittberg and Peterson described periosteum-covered autologous chondrocyte implantation (ACI-p).3-6 After these initial studies, many surgeons replaced the periosteum with a collagen type I/III membrane (ACI-c) to reduce surgical time, patient morbidity, and the risk of hypertrophy. The current third generation of ACI utilizing matrix-seeded chondrocytes (ACI-m) was introduced and made commercially available, including MACI. The indications for ACI treatments have remained consistent with the original suggestions. Because the treatment is very costly, 7 much efforts have been put into ensuring that the treatment is only offered to the patients where superiority over microfracture can be expected, for example, larger defect sizes.
While evidence for using ACI and related treatment continues to expand, there have been few reports detailing patient and defect characteristics across large patient populations. It has also become evident that the strict inclusion criteria in prospective randomized clinical trials leads to patient selection that differs from that of patients actually undergoing cartilage repair treatments in clinical practice. The aim of the present study was to investigate these demographic parameters in patients receiving MACI and to compare them to the inclusion criteria for current clinical trials, essentially comparing the reality of cartilage repair with the idealized situation in a restricted trial environment. We hypothesized that patients scheduled for MACI treatment are different from those enrolled in clinical trials of chondrocyte implantation in terms of age, cartilage defect size, and number of defects, and that there are differences between countries. Secondary, we hypothesized that patients included in prospective randomized trials had smaller defects than those included in cohorts of patients treated in clinical practice, rather than a controlled trial.
Methods
Database Review
Anonymized data were obtained from the Genzyme/Sanofi database on patients scheduled for autologous chondrocyte implants with MACI between 2008 and 2013. Only data from countries with more than 10 patients treated were included. Patient demographics (age, gender) and cartilage defect characteristics (size, number of defects) were evaluated. Age and defect size were reported at the time of biopsy, rather than implantation. The database includes a large number of patients, which in the present study is used as an indicator of the characteristics of patients actually receiving ACI treatment.
Literature Review
MEDLINE and Google Scholar were reviewed for clinical cohort and comparative studies in English with unique patient data on patients treated with ACI techniques for treatment of focal cartilage defects in the knee (on April 8, 2015). Arthroscopic treatments could not be discriminated in the database, but the number of procedures is expected to be negligible. Arthroscopic approaches were excluded in the study search, due to the possible confounding of treatment indication in the comparison. The studies were evaluated based on patient age, gender, number of defects, and lesion size. Search words were “ACI,” “ACT,” “MACI,” “Autologous chondrocyte implantation,” “Autologous chondrocyte transplantation,” “Matrix-assisted chondrocyte implantation”; combined with “knee.”
Average patient age, average defect size, number of defects, and male-female ratio in the included studies were noted and compared with the database. Studies not mentioning average age and average defect size, and where these parameters could not be calculated using information in the respective articles, were excluded. Weighted average age and lesion sizes were calculated with respect to the enrolled patients in each study. Studies that presented follow-up data from patients previously published were excluded. Novel applications such as hydrogel-based administration were also excluded. Studies not directly addressing whether patients had been enrolled in previous trials were included. The included studies were grouped by country and compared by country to the database data when possible.
Statistical Analysis
Bartletts’s test revealed unequal variance of the patient age and defect size. Hence, t test for independent samples with unequal variances was used to test our hypotheses. Variables compared between cohort studies and comparative trials were investigated using weighted 2-sample t test. 8 Register data and data in studies (age and defect size) was investigated using t test with weighting of studies based on patient number. A significance level of P < 0.05 was used.
Results
A total of 2,690 patients from 9 European countries, Australia, and Singapore were included in the evaluation. Ireland, Portugal, Qatar, United Arab Emirates, China, Hong Kong, Philippines, New Zealand, and Malaysia had less than 10 patients operated and were excluded.
Comparison of Studies and Database
In the Genzyme/Sanofi database of 2,690 patients the average age was 33.7 years (range = 11-65), and male-female ratio was 67:33. Mean defect size was 5.64 cm2 (range = 0.16-47 cm2). Single defects accounted for 81% whereas 19% were multifocal. There were no correlations between mean defect size and number of defects or patient age. On average, 18.9% of cartilage defects were small (<3 cm2) (and 63.1% of these were <2 cm2); 11% were large (>10 cm2), and the majority of defects (70%) were medium in size (3-10 cm2) ( Fig. 1 ).
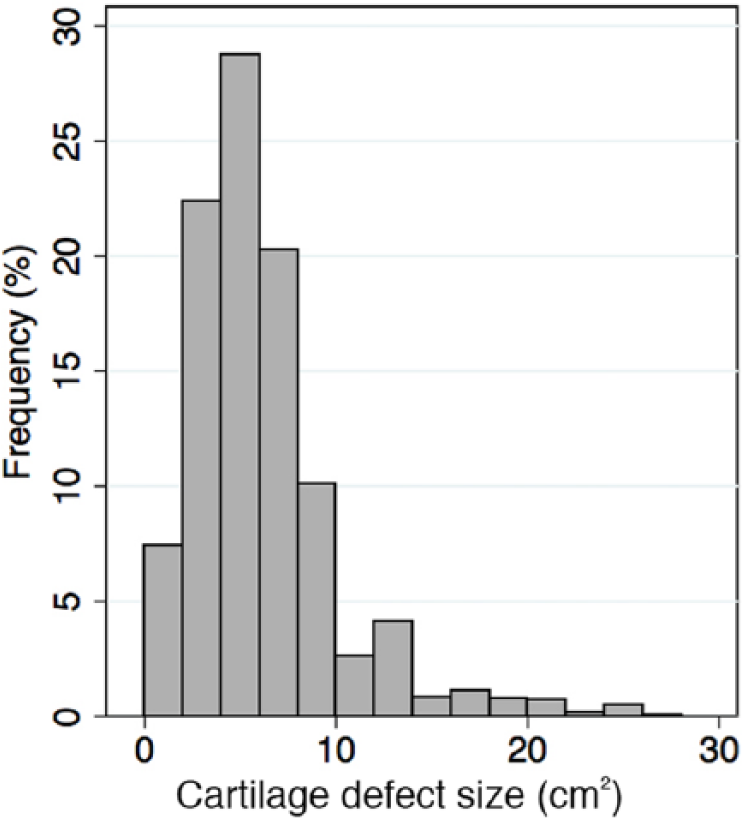
Frequency distribution of defect sizes of patients included in the database. Bars represent intervals of 2 cm2.
A total of 71 studies fulfilled the inclusion criteria with a total of 5,449 patients ( Tables 1 and 2 ). Twelve studies were prospective randomized trials. Four randomized trials were retrospective and were assigned to the cohort group of studies, giving a total of 57 studies in the cohort group. The weighted mean age of all studies was 34.2 years (range = 8-65 years), and the combined weighted mean defect size was 4.95 cm2 (range = 0.5-36 cm2). The defect size of the patients in the database was significantly larger than that of patients included in the studies (P = 0.001). There were no difference in age between the database and the studies (P = 0.68).
Demographics of Patients Receiving Chondrocyte Transplantation Enrolled in Cohort Studies and Retrospective Comparative Studies a .
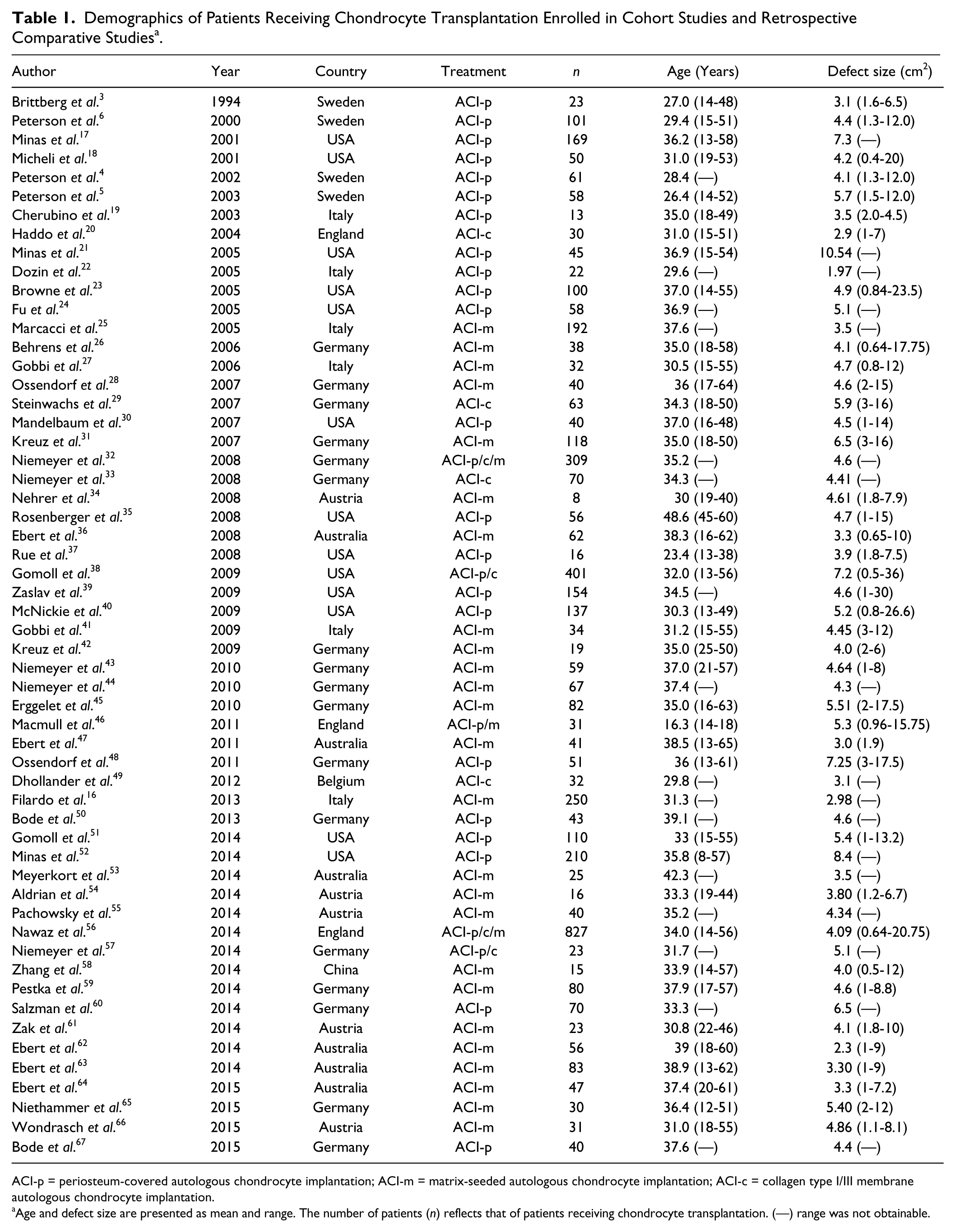
ACI-p = periosteum-covered autologous chondrocyte implantation; ACI-m = matrix-seeded autologous chondrocyte implantation; ACI-c = collagen type I/III membrane autologous chondrocyte implantation.
Age and defect size are presented as mean and range. The number of patients (n) reflects that of patients receiving chondrocyte transplantation. (—) range was not obtainable.
Demographics of Patients Receiving Chondrocyte Transplantation Enrolled in Prospective Clinical Comparative Trials a .
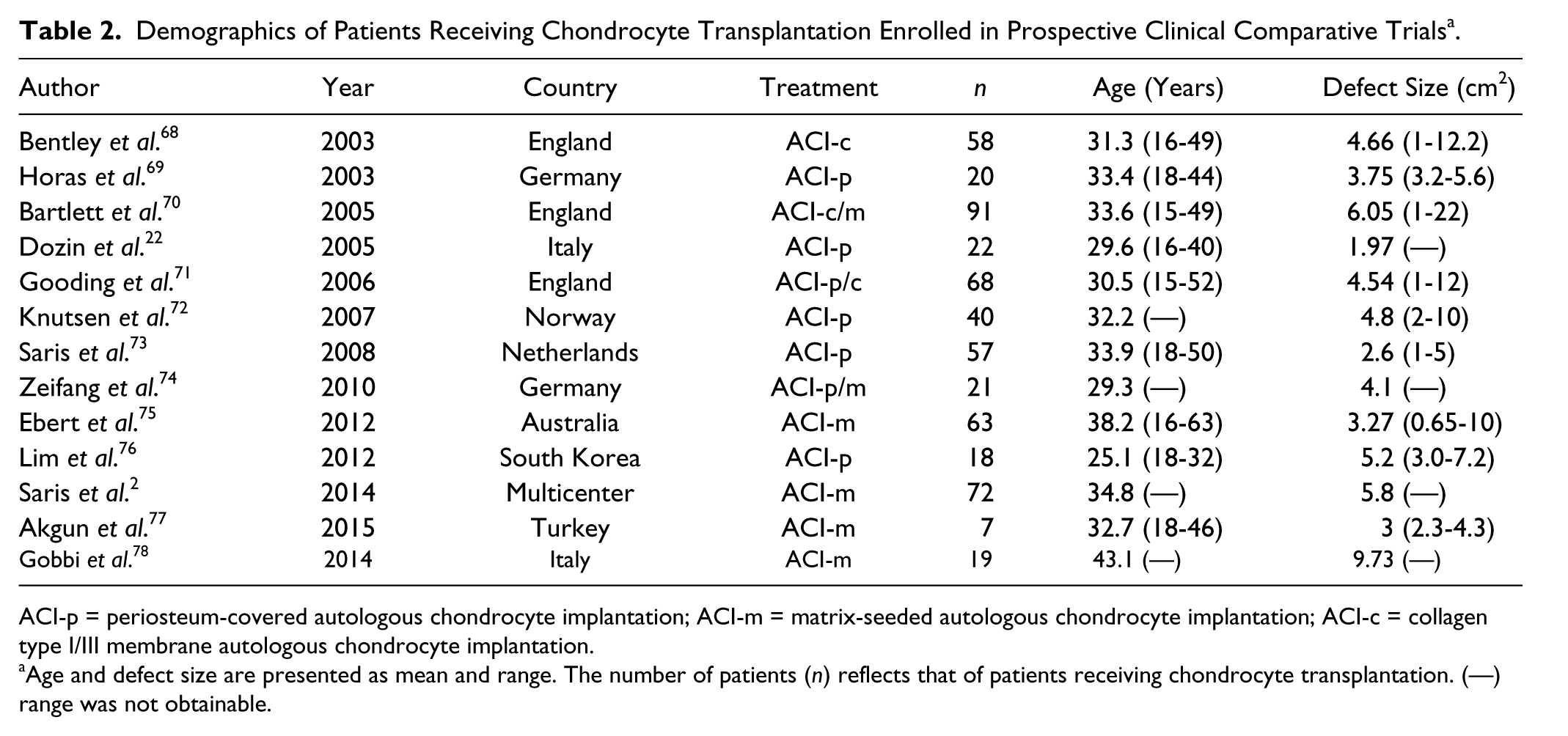
ACI-p = periosteum-covered autologous chondrocyte implantation; ACI-m = matrix-seeded autologous chondrocyte implantation; ACI-c = collagen type I/III membrane autologous chondrocyte implantation.
Age and defect size are presented as mean and range. The number of patients (n) reflects that of patients receiving chondrocyte transplantation. (—) range was not obtainable.
The weighted mean ages in cohort studies and randomized trials were 34.3 years and 32.9 years, respectively, and this difference of 1.6 years was not statistically significant (P = 0.91). Weighted mean defect size was equal for the 2 groups of studies (4.94 cm2 vs. 4.37 cm2; P = 0.93). Male-female ratios in the 2 groups of studies were also similar (60%), which was lower than that in the database (67%). Prospective comparative studies included only patients with single lesions while 19% of the treated patients in the register had multifocal lesions.
International Comparisons
Significant differences in patient age and cartilage defects size in the database were observed between countries ( Fig. 2 ). Defect sizes are presented in descending order: Turkey 7.4 cm2 [6.3; 8.5]; Spain 6.8 cm2 [6.0; 7.6]; Greece 6.5 cm2 [5.9; 7.2]; Italy 6.3 cm2 [5.8; 6.8]; Singapore 5.9 cm2 [5.1; 6.8]; Netherlands 5.7 cm2 [3.4; 8.1]; Australia 5.5 cm2 [5.1; 5.8]; Denmark 5.2 cm2 [4.3; 6.1]; Germany 5.1 cm2 [4.8; 5.5]; England 5.0 cm2 [4.7; 5.2]; Israel 3.6 cm2 [2.2; 4.9].
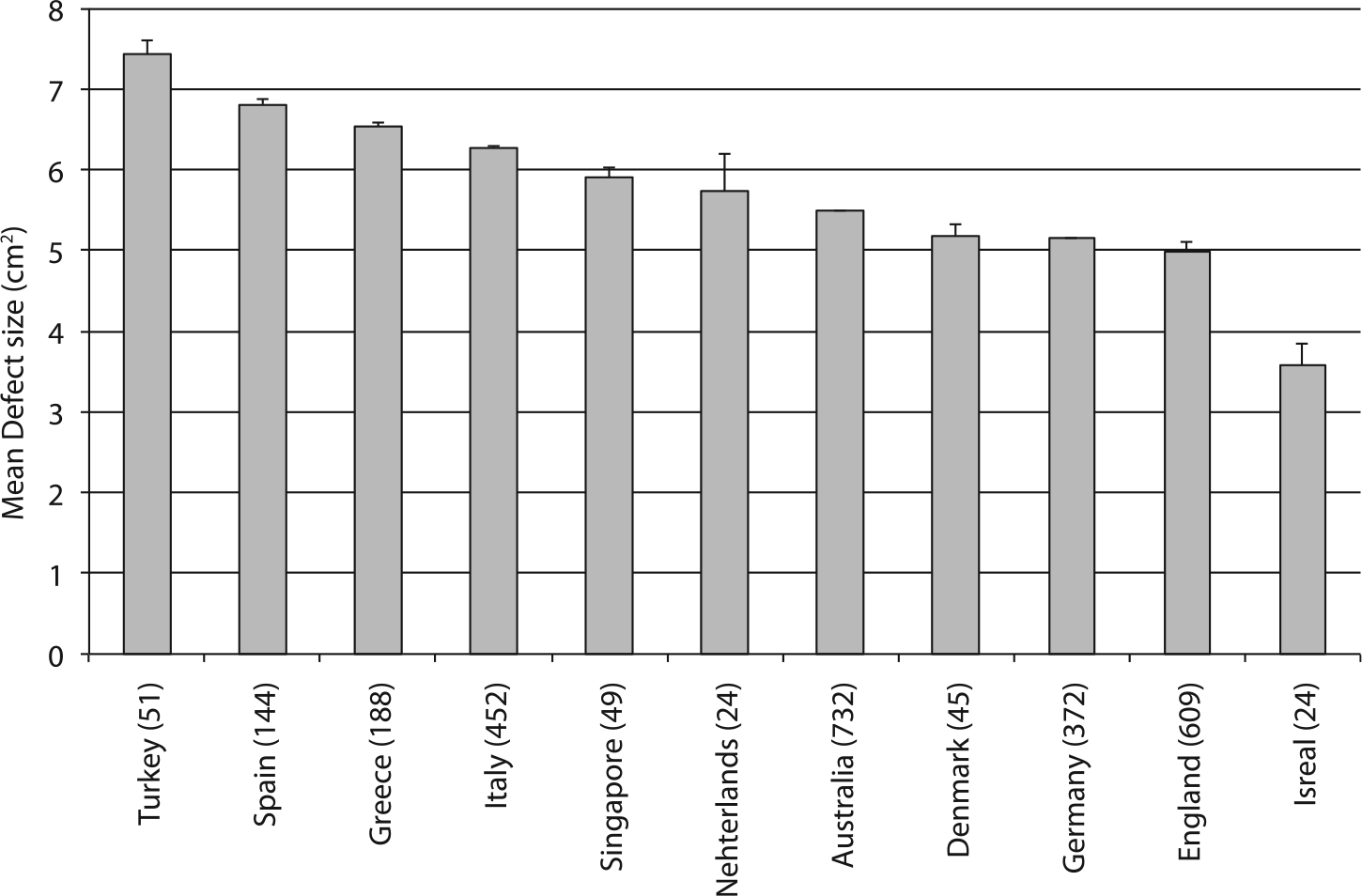
Mean defect size by country of patients included in the database. Values in parentheses are number of patients included by country. Bars are standard error of mean.
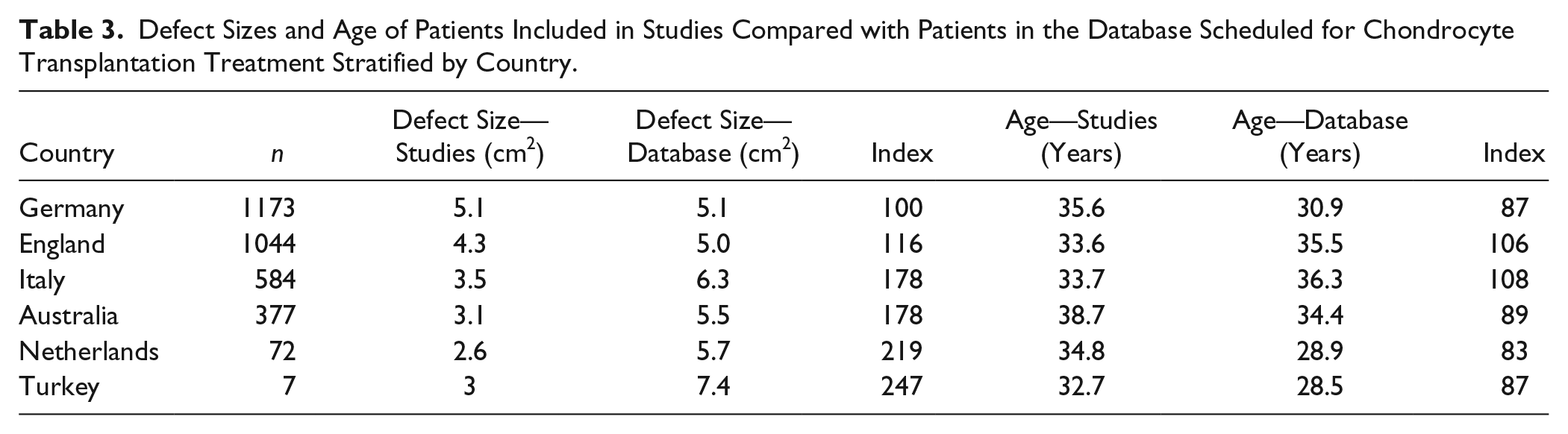
Stratification by country of the included studies showed that defect size in patients receiving chondrocyte transplantation was up to 1.5 to 2.5 times larger than that of the patients enrolled in their clinical trials.
In Swedish3-6 studies, average defect size was 4.5 cm2, in Austria34,53,54,60,65 3.2 cm2 (n = 154), whereas patients in the United Stated17,18,21,23,24,30,35,37-40,50,51 had the largest average defect size of 6.5 cm2 (n = 1,591). Notably, most studies included operated patients that were younger and had larger defects than their respective trials ( Table 3 ).
Defect Sizes and Age of Patients Included in Studies Compared with Patients in the Database Scheduled for Chondrocyte Transplantation Treatment Stratified by Country.
Discussion
In the present study, we compared 2,690 patients assigned for treatment with MACI for cartilage defects in the knee with 5,449 patients enrolled in cohort studies and prospective clinical trials. The majority of the patients scheduled for MACI treatment were comparable in terms of age and defect size, to those included in cohort and prospective comparative studies instructing current treatment guidelines. Comparing average defect sizes, however, the defects were larger in the database than the average defect size in the cohort studies. We further discovered that the size of the cartilage defects in patients assigned for MACI varied significantly between countries.
The differences in cartilage defect sizes between patients enrolled in trials and those scheduled for ACI with MACI may be multifactorial. Obviously, strict inclusion criteria for studies in terms of limiting population sizes for sufficient power may be partly responsible for this difference. However, due to the significant cost of the treatment compared to other modalities, public health care systems and private insurance companies may be reluctant to offer this treatment to patients with defect size in the lower end of the recommended interval.
Engen et al. previously addressed the issue of differences between patients enrolled in cartilage repair trials and those seen in their clinic with respect to all different surgical cartilage repair modalities. 9 They found that of 137 patients referred to their clinic with cartilage defects only 4.4% were eligible for inclusion in all randomized controlled trials ranging between 7% and 80% for the individual studies. The main contributor in their review was defect size, while age and additional joint injuries such as meniscal tears were also important. The database applied in our comparison did not contain information of joint comorbidities.
Treatment selection for focal articular cartilage lesions requires several patient-specific considerations as well as attention to additional joint pathologies.
Out of the various factors predicting outcome of ACI procedures for cartilage repair, age and defect size are often addressed. While some authors find age to be a factor influencing outcomes, convincing evidence of the role of defect size is still absent.10,11 Ebert et al. reviewed patients from 2 of their trials for factors predicting 5-year outcome after MACI treatment and found that while preoperative physical and mental scores in the SF-36 questionnaire contributed significantly to the 5-year KOOS value, cartilage defect size and preoperative duration of symptoms were only predictors of outcome on magnetic resonance imaging evaluation. 12 Behery et al. recently reviewed the evidence of different patient-specific parameters and their effect on outcome after cartilage repair in 13 studies. They found that neither patient age nor defect size were independent factors related to the clinical outcome. 13 Similar results were found by Smith et al., in an analysis of 284 patient data sets, and by Jungmann et al., investigating risk factors for revision surgery after ACI.14,15
Other factors for consideration in patient selection include alignment, ligamentous and meniscal injuries, and amount of degenerative changes. In the present article, we only address 2 specific characteristics, namely, age and defect size. Unfortunately, the database was inconsistent in the reporting of anatomical location of the defect and these data therefore were not included in our study. Females are less likely to receive ACI treatment as seen in the database compared with the studies. The role of gender in focal cartilage damage and outcome after ACI has been investigated previously and some controversy exists. While Jungmann et al. found the female gender to be negatively related to outcome, Filardo et al. showed in a match-pair analysis that while females generally had more complex cartilage injuries, all other factors equal, the female gender did not predict worse outcome after ACI-m.15,16
There are no clear explanation for the international differences observed in patient inclusion for MACI treatment. Cultural aspects may play a role but different health care and reimbursement systems may also be important. The database does not provide any information on whether patients were treated in private or public hospitals. Notably, studies carried out in the United States had the highest average defect size of the study population, but it still remains unclear how this compares to the patient population receiving chondrocyte implantation in that country.
The present study used nonstandardized surgeon assessment of defect size, which could potentially confound the data. If all surgeons overestimated or underestimated the defect size during arthroscopy for the database compared with a postdebridement measurement in the studies, this may be a potential source of bias. It is, however, a measurement method similar to that most commonly used in clinical studies. For example, the largest combined defect size in the register is estimated to be 47 cm2, which likely represents an outlier. The high number of included patients and surgeons performing the evaluations limit the role of this potential confounder as well as the influence of the very few statistical outliers. As the database contained age at the time of biopsy, the actual age of the patients at the time of surgery will be higher, but the actual age at the time of surgery is unknown. However, it could be argued that since the biopsy is taken at the time of indication for chondrocyte transplantation, this may be the more correct measure to use, as we do not look at the outcome in relation to age. The Genzyme/Sanofi database did not contain information on body mass index and the reproducible information on anatomical location of the defect was insufficient to allow for analysis. There were also no data on additional knee injury such as meniscal and ligament tears. All these factors are however also important in considering the correct patient selection for treatment of cartilage injuries with autologous chondrocyte implantation.
We compared patients scheduled for a commercially available third-generation ACI treatment—MACI. This was compared with patients scheduled for many different types of ACI-related treatments. In the comparison made in the present study, emphasis is put on indications, removing potential confounding since the indications are similar for all types of ACI treatments regardless of generation or commercialization.
In our comparison there is overlap in patient data between the database and the studies, since patients receiving MACI in the studies are also present in the database. This could impair the validity in terms of potential bias in the country-stratification comparison if countries with no or little difference between defect size in the database and reported studies (e.g., Germany and England) were only using MACI in the reported studies. This is however not the case and the risk of bias is presumed to be of small in this comparison.
Conclusion
This study shows that the vast majority of patients scheduled for ACI with MACI have articular cartilage defect sizes that are within the range of what is generally recommend for this procedure, although patients enrolled in clinical trials have significantly smaller defects than those scheduled for treatment outside a trial environment. This study also shows that patients receiving MACI treatment in 9 European countries, Australia, and Singapore have different cartilage defect sizes, and in some countries the difference between patients enrolled in trials and generally assigned for surgery differs significantly.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
No ethical approval was required for the completion of this work.