
Abstract
Objective:
Safe articular cartilage lesion stabilization is an important early surgical intervention advance toward mitigating articular cartilage disease burden. While short-term chondrocyte viability and chondrosupportive matrix modification have been demonstrated within tissue contiguous to targeted removal of damaged articular cartilage, longer term tissue responses require evaluation to further clarify treatment efficacy. The purpose of this study was to examine surface chondrocyte responses within contiguous tissue after lesion stabilization.
Methods:
Nonablation radiofrequency lesion stabilization of human cartilage explants obtained during knee replacement was performed for surface fibrillation. Time-dependent chondrocyte viability, nuclear morphology and cell distribution, and temporal response kinetics of matrix and chaperone gene transcription indicative of differentiated chondrocyte function were evaluated in samples at intervals to 96 hours after treatment.
Results:
Subadjacent surface articular cartilage chondrocytes demonstrated continued viability for 96 hours after treatment, a lack of increased nuclear fragmentation or condensation, persistent nucleic acid production during incubation reflecting cellular assembly behavior, and transcriptional up-regulation of matrix and chaperone genes indicative of retained biosynthetic differentiated cell function.
Conclusions:
The results of this study provide further evidence of treatment efficacy and suggest the possibility to manipulate or induce cellular function, thereby recruiting local chondrocytes to aid lesion recovery. Early surgical intervention may be viewed as a tissue rescue, allowing articular cartilage to continue displaying biological responses appropriate to its function rather than converting to a tissue ultimately governed by the degenerative material property responses of matrix failure. Early intervention may positively impact the late changes and reduce disease burden of damaged articular cartilage.
Keywords
Introduction
The goal of early surgical intervention for articular cartilage damage is to stabilize lesions as a means to decrease symptoms and disease progression. 1 Lesion stabilization remains a necessary prerequisite toward articular cartilage tissue preservation because removing the irritant of damaged tissue and creating a residually healthy lesion site remain required substrates for permitting or inducing effective in situ healing responses. Comparative effectiveness research has demonstrated significant advances in the safety profile for articular cartilage lesion stabilization with nonablation radiofrequency technology,a,2,3 improving evidence-based medical decision making and health care resource allocation.
Prior to the advent of nonablation technology for articular cartilage lesion stabilization, thermal and plasma radiofrequency ablation devices appeared to be more efficacious than mechanical shavers by exhibiting a smaller time-zero collateral injury footprint.6-12 However, because matrix corruption and chondrocyte depletion within contiguous healthy tissue occur commensurate with, and often significantly expand following, volumetric tissue removal,2,3,13-25 this technology did not become widely adopted, as it is understandable that such damage can impair or inhibit in situ healing responses13,15,16,19,25 as well as contribute to disease progression by enlarging lesion size.18,22,23,26-33 Despite optimizing ablation device performance, this collateral injury footprint transgresses zonal boundaries in which the depth of necrosis in nontargeted tissue remains larger than native superficial zone thickness; consequently, the functional properties and vital healing phenotype of the superficial zone are always effectively eliminated.2,3 These collateral wounds originate because ablation technology, like mechanical shavers, cannot distinguish between damaged and undamaged tissue. Utilizing direct electrode-to-tissue interfaces indiscriminately deposits current into tissue, which causes surface entry wounds and subsurface necrosis through resistive tissue heating and tissue electrolysis; also, because of its high water content, articular cartilage is inherently at risk for efficiently pooling electrothermal energy to a detrimental level. Some have advocated manually positioning the active electrode away from healthy tissue to target diseased tissue34,35; however, this technique significantly increases the amount of current required to overcome the effects that the fluid flow and convective forces present during surgical application exert on exposed device electrodes. Others have offered that intentional current-based damage serves as a barrier to additional current deposition without demonstrating damage efficacy. 20 Still others utilize current to create ionizing electromagnetic radiation associated with high temperature plasma formation,36-39 which has raised further concerns regarding iatrogenic chondrocyte DNA fragmentation and nuclear condensation that can induce apoptosis, 40 cellular senescence, 41 decreased 42 progenitor cell populations,43-47 diminished cellular differentiation potential, 42 and altered extracellular matrix structure and production. 48 Additional effects of ionizing electromagnetic radiation on chondrocyte behavior important for in situ healing responses49-57 remain worrisome.
Nonablation technology enables selective targeting of diseased tissue traits by utilizing a protected electrode architecture that prohibits electrode-to-tissue contact as a means to eliminate volumetric and functional overresection that further impairs contiguous healthy tissue from retaining and displaying differentiated phenotypes.2,3,58-60 The protective housing creates a primary reaction zone that is shielded from the large physical fluid flow and convective forces present during surgical application, enabling deployment of low-level radiofrequency energy delivery into interfacing media rather than into tissue to create physiochemical conversions that can be used for surgical work. This process creates an engineered irrigant that physiochemically loads tissue surfaces in a manner uniquely suited to effect the accessible and degenerate surface matrix structure of damaged articular cartilage tissue preferentially rather than the intact chondron and matrix tissue deep to the surface lesion level. As an illustration, pH shifts can be generated, such as preferential sodium hypochlorite precipitation akin to production through neutrophil myeloperoxidase catalysis, and configured to react oxidatively with a wide variety of biomolecules at tissue surfaces including the exposed proteoglycan aggregates of damaged articular cartilage.61-63 Such proton charge shifts have been shown to produce mechanical alterations at articular cartilage surfaces2,3 through electrochemomechanical coupling via site-specific hydrogen and disulfide bond alterations within constituent proteoglycan and collagen.64-69 These targeted gradients at tissue surfaces modulate mechanical and electrochemical tissue matrix properties by altering fixed and variable charge densities while effecting consequent extracellular intrafibrillar hydration and osmotic character.70-79 This physiochemical loading of accessible surface-based diseased tissue can alter the relative ratio of tension compression nonlinearity toward a state amenable to gentle shear deformation mechanical debridement of tissue already characterized by the deteriorating surface-layered shear properties of collagen fibril disruption and orientation changes, weak collagen-to-proteoglycan bonds, proteoglycan and lipid depletion, aberrant water content, and decreased fixed charge density.80-84 Optimizing the surface shear properties of early articular cartilage damage through cleavage plane stabilization is an important parameter for overall lesion stabilization relative to perturbation specificity 58 particularly because these mechanisms do not impair residual chondrocyte viability.2,3,85 These layered surface properties exploited for cleavage plane shear stabilization have been observed in other tissue types and locales requiring shear mitigation during surface degeneration and normally represent a back-up mechanism to boundary lubrication regime failures associated with perturbation exceeding homeostasis and tissue repair for reversible lesions.56,86
It has been demonstrated previously that nonablation technology selectively targets diseased tissue for removal without causing necrosis in contiguous healthy cartilage tissue while producing the chondrosupportive matrix modification of increased live chondron density in the superficial zone.2,3 Because chondrocyte viability in subadjacent tissue is not altered, the opportunity presents to evaluate chondrocyte behavior in response to lesion stabilization. The purpose of this study was to examine the focal effects upon residual articular cartilage surface chondrocytes during lesion stabilization with nonablation technology by evaluating time-dependent chondrocyte viability, nuclear morphology and cell distribution, and temporal response kinetics of matrix and chaperone gene transcription indicative of differentiated chondrocyte function.
Materials and Methods
Study Design, Human Tissue Specimens, and Nonablation Treatment
Because eliminating articular cartilage overresection has been enabled for patients only recently, this study was designed as an exploratory assessment of an experimental explant model that represents human disease while not requiring in vivo biopsies of preserved tissues (contrary to the goal of eliminating overresection) to simultaneously evaluate intrapatient measures of both volumetric and functional overresection. Mutually confirmatory testing methods across 3 investigational categories were included with paired controls in order to gather a broad and interrelated data range representing residual contiguous chondrocyte viability and differentiated function. As an exploratory assessment, and prior to extending to other human subjects an experimental tissue injury model that includes access to a patient’s personal genetic information, 87 this study sought to evaluate the model in a single patient displaying the opportunity for uniform articular cartilage lesion sampling of a sufficient combined geographic area necessary to complete the multiple testing procedures with appropriate model test-method repeatability replicates. As an initial benchmark, articular cartilage samples were evaluated at 1 hour (earliest postharvest treatment-processing time) through 96 hours (after which chondrocyte responses can be more reflective of incubation environment rather than the treatment method 88 ).
Osteochondral specimens were harvested from patients undergoing total knee replacement under an approved Human Subjects Research and Institutional Review Board protocol that included informed written patient consent. The total knee replacement procedures were performed by a single surgeon in the normal course of his practice. The tissue to be normally discarded during the procedure was examined prior to harvest once the knee joint was entered surgically to determine if it met study inclusion requirements. Specimens were included that demonstrated an area of uniform partial-thickness surface fibrillation of sufficient size from which matched-pair test samples could be obtained from each specimen. Specimens were divided into smaller test sample parts after harvest by sharp sectioning and were immediately transferred to an ex vivo saline arthroscopic treatment setting. The individual specimens of each matched pair were randomized as to which remained untreated or became treated.
A nonablation radiofrequency device designed for cartilage lesion stabilization was used per the manufacturer’s specifications (Ceruleau, NuOrtho Surgical Inc., Fall River, MA). Lesion stabilization was performed by one surgeon accustomed to device use. The goal of the procedure was to remove the fibrillated cartilage damage and smooth the articular surface as determined by visual and tactile cues. Standard saline arthroscopic fluid was deployed at 20 °C with a fluid flow rate of 30 mL/min ± 5 mL/min, which created consistent fluid dynamics in the setup typical of in vivo arthroscopy. Energy delivery (Valleylab Force FX-C, Covidien Inc., Mansfield, MA) was standardized at 25 W with an 8,500-V peak-to-peak setting (4,250 peak voltage) and 390-kHz damped sinusoid bursts with a repetition frequency of 30 kHz into 500 ohms (i.e., COAG, fulgurate). Lesion stabilization treatment time was 5 seconds for all specimens, with a technique of moving the probe tip tangentially across the tissue surface with a consistent application pressure and speed as judged by the surgeon to mimic in vivo treatment conditions. The protective housing edge was used to gently shear-debride the fibrillated tissue concurrent with energy delivery for the allotted treatment time. This technique did not deploy the heat delivery capabilities of nonablation technology available through electrosurgical plenum positioning or increased energy levels that can be used 58 for the more demanding lesion stabilization associated with less fibrillated tissue displaying a different degeneration-based collagen fibril-to-water structure (see Discussion); as deployed in this study, the delivery of heat to tissue surfaces is limited by a triphasic nature to low temperature changes (i.e., Δ 0-7 °C) of interfacing media, 58 which is design appropriate for the low thermal requirements that would be necessary to manipulate exposed surface type II collagen, which begins to denature at 39 °C. Paired sample explants served to generate untreated samples to serve as control that remained in an identical treatment bath during the procedure. After treatment, the matched-pair samples were randomly divided into 3 groups for evaluation of time-dependent chondrocyte viability, nuclear morphology and cell distribution, and temporal kinetics of versican, COL2A1, and HSPA1A gene expression in surface chondrocytes.
Evaluation of Time-Dependent Chondrocyte Viability
The samples allocated to this group were evaluated at 1-hour and 96-hour intervals after treatment for alterations in chondrocyte viability. Samples were prepared by thin sectioning to isolate the surface region containing superficial and transitional zone chondrocytes and matrix from the remainder of the tissue (sample dimensions: 3-mm thick by 7-mm square). These surface cartilage specimens were left as bulk tissue and incubated at 37 °C in Dulbecco’s Modified Eagle’s Medium (Invitrogen Inc., Carlsbad, CA) with fetal bovine serum and 1% penicillin-streptomycin (10,000 U and 10,000 µg, respectively). No equilibration period was used, and the specimens were incubated in 95% air with 5% CO2. At 1 hour and 96 hours, three 0.5-mm coronal sections of each sample referencing the center of the untreated and treated sites were created and prepared for staining by washing in HEPES buffered saline solution. Live/Dead Reduced Biohazard Cell Viability Kit #L-7013 (Invitrogen Inc.) was used per the manufacturer’s specification to stain samples. Samples were gluteraldehyde fixed, transferred to standard flat glass slides, and flooded with VectaShield fluorescence protection oil (Vector Laboratories, Inc., Burlingame, CA) prior to the placement of No. 1.5 borosilicate glass cover slips over each sample section.
Confocal fluorescence laser microscopy analysis was performed by personnel blinded to the identity of the treatment groups for each sample. Confocal imaging was performed with an IX-81 inverted microscope coupled to a FV300 confocal laser-scanning unit (Olympus Inc., Center Valley, PA) using continuous-wave 488-nm laser excitation (Sapphire 488HP, Coherent Inc., Santa Clara, CA). Live cells were captured under the green fluorescence channel (505-525 nm), and dead cells were captured under the red fluorescence channel (577-634 nm), generating a live image, a dead image, and an integrated image. Histological characteristics and cell viability between untreated and treated samples were assessed by comparative image evaluation for change in live and dead cell populations.
Nuclear Morphology and Cell Distribution
The samples allocated to this group were evaluated at the 1-hour posttreatment interval to determine alterations in nuclear morphology and cell distribution. Samples were maintained after treatment in the arthroscopic saline bath and prepared by thin sectioning and incubated as above. Because significantly altered nuclear characteristics would not be expected in the presence of continued differentiated nucleic acid production over time, incubated samples would only be evaluated at 96 hours should continued gene expression not be observed in both untreated and treated samples (as described below) in order to assess possible transcriptional failure modes. Three 0.5-mm coronal sections of each sample referencing the center of the treatment site and control were created and prepared for staining by washing in HEPES buffered saline solution. Hoechst 33342 stain, trihydrochloride FluoroPure (#H-21492, Invitrogen Inc.), was used per the manufacturer’s specification to stain samples. Samples were fixed and prepared for imaging as above.
Two-photon excitation microscopy was performed with an IX-81 inverted microscope coupled to a FV300 confocal laser-scanning unit (Olympus Inc.) using a 60x 1.2-NA water immersion objective (UPLSAPO 60XW, Olympus Inc.) for imaging. A dichroic mirror that reflected the near-infrared laser excitation light and transmitted the visible (~460 nm) bisbenzimide emission was used as the excitation dichroic. The excitation source was a mode-locked titanium sapphire laser (Broadband Mai Tai, Spectra Physics, Newport Inc., Irvine, CA) operating at 800 nm with a pulse width of approximately 100 fs and a pulse repetition rate of 80 MHz. An average power of approximately 30 mW (measured at the back aperture of the microscope objective) was used to excite the sample emission. A short-pass filter with a cut-off wavelength of 680 nm (FF01-680/SP, Semrock Inc., Rochester, NY) was used to filter residual 800-nm excitation laser light from the emission. Water was used as an immersion fluid to optically couple the sample and objective to the cover slip.
Serial x-y plane tomographic images along the z-axis were generated to evaluate nuclear morphology and cell distribution. Dye exclusion properties were not evaluated. These images were compressed into a single x-y image combining the nuclear contents along the z-axis image planes into a single composite view to facilitate additional interchondrocyte nuclear comparisons. BioView open-source cross-platform application software (Center for Bio-Image Informatics, University of California, Santa Barbara, CA) was used to evaluate cell distribution patterns because all sample chondrocyte nuclei stain with bisbenzimide. Axis rotations were performed to evaluate matrix modifications of treated versus untreated samples that may affect cell distribution patterns as noted previously. 3
Evaluation of Matrix and Chaperone Gene Expression by Real-Time Polymerase Chain Reaction (RT-PCR)
The samples allocated to this group were prepared by thin sectioning (sample dimensions: 2-mm thick by 5-mm square) and incubated as above. Untreated and treated samples were randomly assigned to incubation intervals of 1, 24, 48, 72, and 96 hours. At the end of each incubation interval, the samples were frozen in liquid nitrogen and stored at –80 °C prior to RT-PCR testing. At testing, the samples were thawed and mechanically homogenized in lysis reagent (QIAzol #79306, Qiagen Inc., Valencia, CA). The homogenate was separated into aqueous and organic phases by centrifugation, and mRNA was subsequently isolated by spin column elution (RNeasy Lipid Tissue Mini Kit #74804, Qiagen Inc.).
Quantitative reverse transcriptase RT-PCR was performed (7300 Real-Time PCR System, Applied Biosystems Inc., Carlsbad, CA) by monitoring the increase in reporter fluorescence of Taqman gene expression assays (Applied Biosystems Inc.) for versican (#Hs00171642_m1), COL2A1 (#Hs00264051_m1), and HSPA1A (#Hs00359163_s1). RNA concentration obtained was determined for both untreated and treated samples and evaluated for significant differences; sample purity was evaluated for each specimen by determining R260/280 values (ultraviolet absorbance ratio at 260 nm and 280 nm). Expression changes were quantified by the comparative CT method to calculate relative fold changes normalized against 18s rRNA, calculated as the difference (ΔCT) between the CT value of the target and 18s rRNA control. Each sample was assayed in duplicate with relative expression calculated and tabulated as 2–ΔΔ CT relative to each incubation interval sample group. The mean and standard deviation were calculated for each fold change grouping. Curve fit regression analysis for mRNA expression temporal kinetic fold change was performed (TableCurve 2D, version 5.01.02, Systat Software Inc., Chicago, IL) for the treated sample groups compared to the average ΔCT of the 1-hour untreated sample group serving as control and as time zero designed to demonstrate the relative scale of expression responses over time.
Results
Study Design, Human Tissue Specimens, and Nonablation Treatment
The tissue samples for this study were donated by a 59-year-old female patient diagnosed with symptomatic bilateral knee primary osteoarthritis and without prior surgical cartilage treatment. Articular cartilage tissue sampling was generated from femoral condyle, tibial plateau, and patella locations that demonstrated consistent intersite surface fibrillation as judged by arthroscopic-magnified visual and tactile cues and that retained a gross harvest site cartilage thickness of at least 3 mm, conditions indicative of the diseased state studied. Matched-pair samples were successfully created and randomized into the 3 investigational categories. The general results across these categories demonstrated corroborating model validation of the mutually confirmatory testing methods included in this experimental explant model, signifying residual contiguous chondrocyte viability and differentiated behavior without evidence of volumetric or functional overresection.
Evaluation of Time-Dependent Chondrocyte Viability
Four matched-pair samples were allocated to this group, 2 for each time interval. The untreated samples demonstrated surface fibrillation consistent with gross visual inspection of the tissue at the time of harvest. The superficial zone was disrupted by the fibrillation, but chondron appearance typical of this zone remained present in and around the fibrillation. Live cells were abundantly observed with only occasional dead cells residing in extruded positions at the frayed margins of the fibrillated tissue. Treated samples displayed elimination of the fibrillated tissue and smooth surfaces at the treatment site. No evidence of necrotic tissue was present with the surfaces subadjacent to the removed damaged tissue retaining superficial zone characteristics typical of the intact superficial zone regions of the untreated samples. An increase in dead cell populations was not evident in either the 1-hour or the 96-hour treated samples over the untreated sample groups, nor was a decrease in chondrocyte viability observed relative to incubation time.
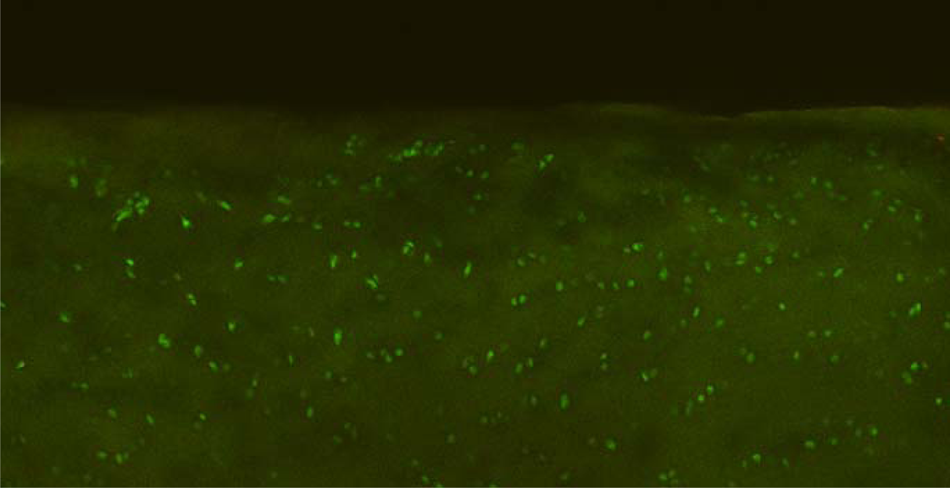
Representative posttreatment integrated live/dead cell viability stain section image, demonstrating viable chondrocytes. Note the lack of dead chondrocytes and a smooth surface in the tissue subadjacent to the targeted removal of surface-fibrillated tissue damage. Original magnification, 10x.
Nuclear Morphology and Cell Distribution
Four matched-pair samples were allocated to this group, 2 for each time interval. Due to the presence of continued gene expression in both untreated and treated samples (as described below), evaluation was not performed at the 96-hour time interval. The serial tomographic images demonstrated no evidence of altered nuclear morphology when compared to untreated samples. As depicted in
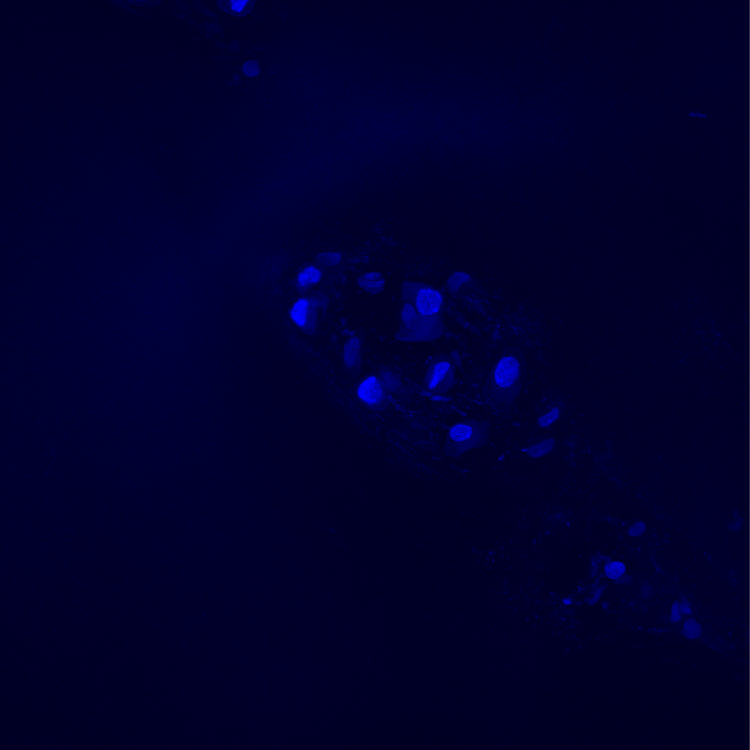
Representative 2-photon confocal composite image of Hoechst-stained chondrocytes with the tomographic z-axis images compressed into a single image. Note the similar staining intensities and lack of nuclear fragmentation or condensation. Original magnification, 60x water.
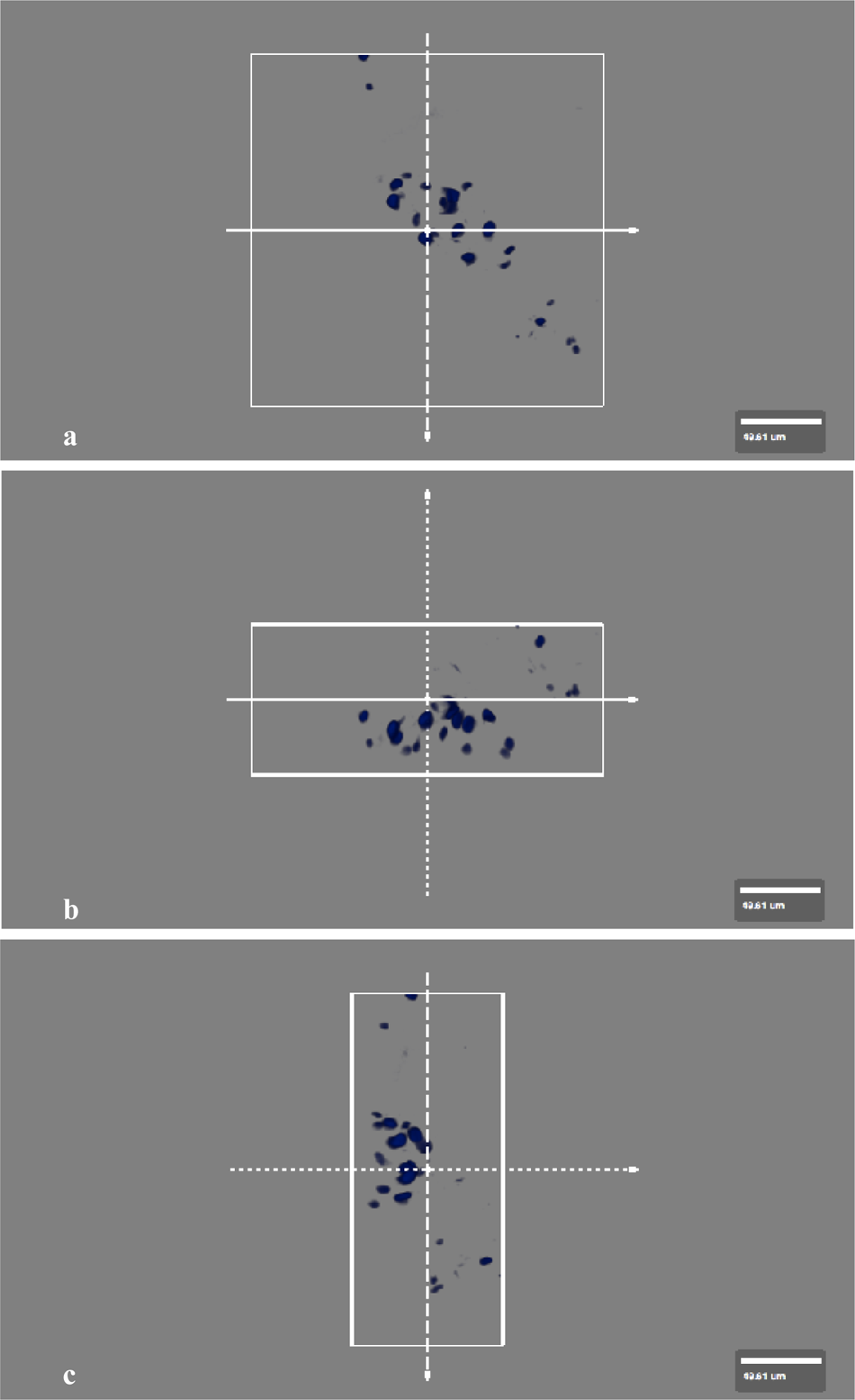
Representative BioView images used to assess 3-dimensional chondrocyte distribution patterns. (
Evaluation of Matrix and Chaperone Gene Expression by Real-Time Polymerase Chain Reaction (RT-PCR)
Twenty samples were allocated to this group, generating 2 untreated and treated paired sample explants for each incubation interval. The RNA quantity obtained included an untreated group concentration of 29.8 ± 9.3 ng/µL and a treated group concentration of 29.7 ± 8.6 ng/µL, with no statistical differences between groups. As depicted in
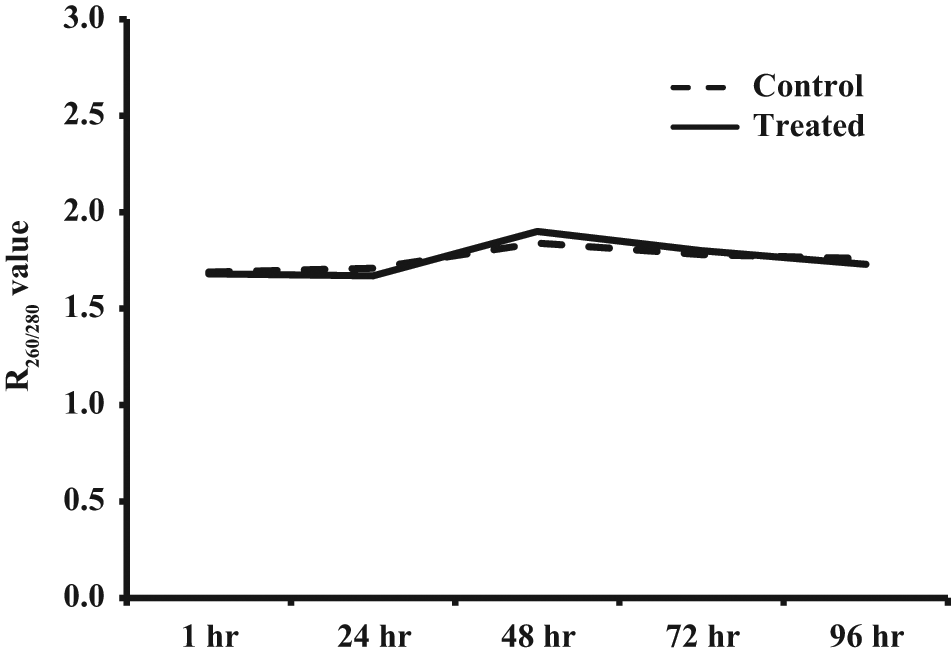
R260/280 values versus time. Note the stability of RNA sample purity produced during the testing period for each incubation interval.
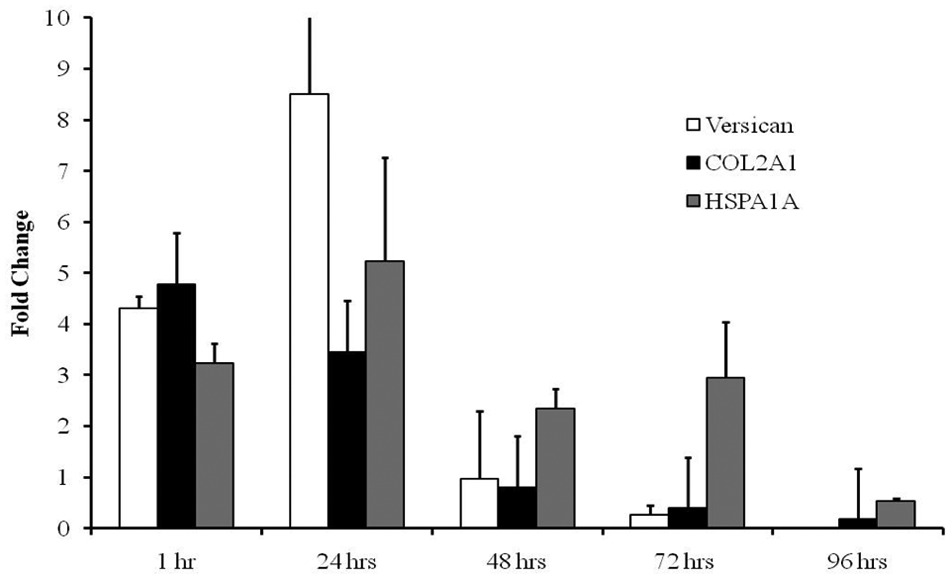
RT-PCR results depicting mean fold changes in transcriptional expression of versican, COL2A1, and HSPA1A mRNA in subadjacent surface chondrocyte after nonablation radiofrequency lesion stabilization. Data reflect fold change relative to the untreated samples at each incubation interval.
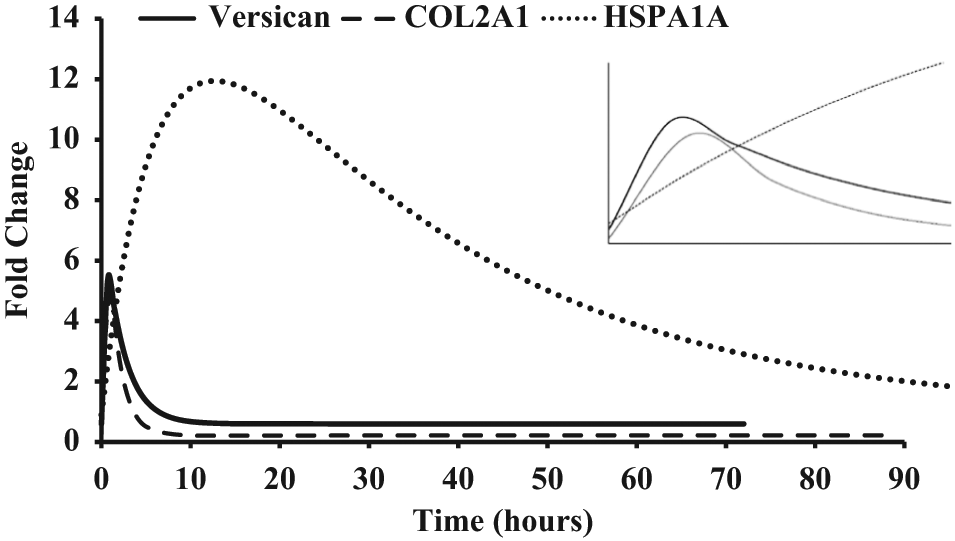
Curve fit regression depicting transcriptional up-regulation in subadjacent surface chondrocytes after nonablation radiofrequency lesion stabilization. Note that the high statistical fit reflects a biological phonomenon of damped exponential activation and deactivation/reaction exhaustion. Inset depicts an enlarged view of the modeled temporal expression kinetics after treatment. Data reflect treated sample groups compared to the average ΔCT of the 1-hour untreated sample group serving as control and as time zero.
Discussion
Because early posttreatment chondrocyte viability is not effected within tissue contiguous to the treatment site during nonablation radiofrequency lesion stabilization,2,3 this study was designed to further delineate treatment efficacy through an exploratory assessment of chondrocyte experiences during and in reaction to lesion stabilization. Subadjacent surface articular cartilage chondrocytes demonstrated continued viability for 96 hours after treatment, a lack of increased nuclear fragmentation or condensation, persistent nucleic acid production during incubation reflecting cellular assembly behavior, and a transcriptional up-regulation of matrix and chaperone genes indicative of retained biosynthetic differentiated cell function. These results add to the emerging efficacy of early surgical intervention, namely, to safely eliminate the irritant of damaged tissue without iatrogenic injury to contiguous tissue,2,3 to stabilize the remaining healthy tissue through chondrosupportive matrix modifications, 3 and to induce an appropriate in situ biosynthetic cellular response within the tissue subadjacent to the lesion that retains differentiated function. While removing the irritant of damaged tissue may slow lesion progression26-33 and permit local homeostatic and repair responses 57 to occur less encumbered, the results of this study suggest that it is possible to manipulate or induce cellular function, thereby recruiting local chondrocytes to aid lesion recovery. As additional information is generated, early surgical intervention may become viewed as a tissue rescue, allowing articular cartilage to continue displaying biological responses appropriate to its function rather than converting to a tissue ultimately governed by the degenerative material property responses of matrix failure. If so, early intervention would impact the late changes and disease burden of damaged articular cartilage.
Versican mRNA expression was evaluated in this study because it is translated into a chondroitin sulfate proteoglycan that resides as aggregates within the interterritorial matrix at articular surfaces.89,90 This site specificity reflects its functional role in the superficial zone extracellular matrix structure89,91 and therefore influences matrix failure–based lesion stabilization of early cartilage damage. Versican displays low chondroitin sulfate density and sulfation levels,89,91 a property reflected in the fixed charge density inherent in surface cartilage amenable to modification by physiochemical loading during nonablation treatment. Because surface-damaged articular cartilage displays an altered fixed charge density due to layered proteoglycan depletion,83,92 this exposed and accessible charge density is an important therapeutic target during the surface events of lesion stabilization because the normal charge barrier 93 associated with the amorphous layer is functionally abolished in damaged articular cartilage surfaces. 94 Boundary lubrication regimes95,96 at normal articular cartilage surfaces provide a unique charge density barrier due to surface-active phospholipids, which is remarkably resistant to the physiochemical loading deployed during lesion stabilization particularly at sites bathed in sodium chloride97-100 as during arthroscopy. This charge density serves as a physiochemical loading barrier to and an intrinsic margin during the surface events of lesion stabilization at intact surfaces, a barrier that is robust enough 95 to require enzymatic digestion, trauma, or other means like ablation energy to transgress in order to reach a collagen layer. The transient versican mRNA transcriptional up-regulation noted in response to lesion stabilization is consistent with prior studies demonstrating posttreatment superficial zone phenotype characteristics2,3 and may be important in the reconstitution of cartilage surface properties by chondrocytes43-47,51-57 after removal of the damaged tissue irritant. More intriguing, however, is that various isoforms of versican have been implicated in actions related to chondrogenesis through mesenchymal condensation, cell aggregation, chondroprogenitor cell promotion, and chondrocyte gene expression.91,101-104 Because the adult isoform core protein size does not seem to change with osteoarthritis, 90 and combined with the evidence for superficial zone progenitor cell populations43-47,91 and chondrocyte proliferation and clustering in early and fibrillated cartilage damage,91,92 versican’s posttranslational role during early tissue responses to lesion stabilization may relate to a protective, and possibly transitional, matrix construct during tissue assembly repair events by modulating chondrocyte adhesion, morphology, proliferation, differentiation, or migration105,106 similar to its function noted during repair and self-assembly events in other tissue types.
The COL2A1 gene encodes the α-1 chain of type II collagen, the major collagen constituent of articular cartilage matrix and a good marker of an activated functional phenotype. The transcriptional enhancement of COL2A1 after targeted lesion stabilization demonstrated in this study serves as an assessment of the generalized chondrocyte function to promote articular cartilage–specific matrix synthesis. Chondrocytes at the site of lesion stabilization retain the ability to produce mRNA reflective of their differentiated phenotype and characteristic of mature cartilage, indicating that the responses are not limited to a fibroblastic-like dedifferentiation and low matrix gene expression reflective of the phenotypic alterations of diseased tissue 92 or other cartilage interventions 107 during which chondrocytes continue to express synthetic activity after treatment. 108 Further evaluation of this response, such as splice variants indicative of a chondroprogenitor phenotype, 109 would be interesting in light of the corresponding versican response temporal kinetics noted in this study.
HSPA1A codes for highly conserved nonsteric molecular chaperones that participate in protein stabilization and assembly by mediating folding and transport of existing or newly translated proteins. Chaperone levels are modulated to reflect the status of protein folding requirements within the cell such as preventing newly synthesized proteins and assembled subunits from aggregation into nonfunctional structures that can occur due to natural macromolecular crowding. Chaperone levels reflect cellular requirements related to biosynthetic responses as a means to monitor changes in cell environment.110-112 In chondrocytes, HSPA1A proteins induce chondroprotection against apoptosis113,114 and help resist the extracellular matrix destruction of osteoarthritis.115,116 HSPA1A is constituently expressed in chondrocytes, 117 while its inducible expression has been related to the terminal differentiation of chondrocytes 118 and is increased in osteoarthritis as an early marker.119,120 Although it is presently uncertain if the translational products of versican and COL2A1 are routine protein clients of HSPA1A chaperones within human articular chondrocytes, HSPA1A expression in this study is consistent with the temporal expression kinetics similar to other studies that have linked HSPA1A up-regulation with active matrix production and the reconstruction of chondrons. 121
It is possible that removal of damaged tissue itself can enable biosynthetic activity in vivo as an unburdened homeostatic or repair response. By removing a biological and mechanical irritant, the lesion site can be altered to a more favorable perturbation-specific mechanotransductive environment supportive of differentiated gene expression.122-128 However, because the tissue in this study was incubated in an unloaded state not reflective of physiological perturbation specificity, 129 it remains unclear whether the removal of the damaged tissue itself is a signaling mechanism responsible for the increased biosynthetic activity observed. Although the untreated group reflected responses of surface-fibrillated articular cartilage incubated in an unloaded environment without significant alteration in baseline mRNA expression studied, the treated samples reflected differentiated biosynthetic function consistent with normal physiological responses. The signaling mechanisms for these responses are unlikely directly related to the physiochemical loading of the cartilage surfaces utilized during lesion stabilization. For instance, because the physiochemical loading deployed in this study did not include heat delivery,58,59 HSPA1A induction should not be related to temperature stress, as up-regulation in chondrocytes does not occur until temperatures exceed 39 °C, 130 a temperature that interestingly is consistent with when exposed but normal extracellular matrix type II collagen begins to denature 131 and that can be deployed in a controlled manner by nonablation technology 58 for more demanding lesions. 132 Further, and although extracellular pH changes can effect chondrocyte metabolism in culture, 133 chondrocytes are not subjected to extracellular alterations in pH during short-term topical loading in sodium chloride environments.97-100 Because nonionizing electromagnetic forces are generated by nonablation devices to promote therapeutic biological responses in tissues unencumbered by necrosis-inducing current deposition,2,3,56,134 these forces should be considered a plausible induction mechanism at least partly responsible for the biosynthetic temporal response kinetics observed in the treated samples.60,134-140 Such fields influence dipole moments, charge movements, and ion transporters that regulate cell function, proliferation, differentiation, and migration135,141-143 and, when applied to cartilage, have been shown to be chondroprotective, to reduce lesion progression, and to increase chondrocyte proliferation, lacuna formation, gene expression, protein synthesis, and extracellular matrix production.144-152 Electromagnetic forces demonstrate activity at independent gene initiation promoter domains through signaling pathways that enable short exposures to induce rapid DNA activation, a mechanism linking protein synthesis to electron charge transport acceleration induced by electromagnetic forces.153,154
Early intervention for articular cartilage damage remains an attractive approach to decrease disease burden because it is this setting that retains the elements in situ for normal cartilage homeostasis and repair. Studies examining chondrocyte behavior in culture provide important insight into concepts for in situ cartilage treatment108,121,155; maintaining chondrocytes in their normal in vivo position preserves their interactions with their extracellular matrix,156,157 an important factor to consider for specific disease-state interventions. While the hallmarks of nonreversible articular cartilage lesions are more obvious, the characteristics of self-repair and regeneration at reversible lesion sites and those relative to salvageable lesions are not yet as recognizable as specific disease states.158-160 Despite the heterogeneity of articular cartilage lesions, chondrocyte viability and a differentiated and healing phenotype at the site of safe damaged tissue removal remain inextricably related to the reversibility of early lesions. Removal of this irritant relative to perturbation specificity is necessary to provide a more favorable environment to express mechanotransductive genes for biosynthesis while interrupting phenotypic shifts persuaded by loading an unhealthy site and, furthermore, for targeted in situ manipulation of those genes. Even more exciting is the potential to allow boundary lubrication regimes that are depleted with damage161,162 to reconstitute over a nonirritated site via self-assembly 163 that may ultimately become a regional substrate for cell-homing techniques reflective of tissue assembly, homeostasis, and repair54,57,164 enabled by eliminating volumetric and functional overresection.
Footnotes
Acknowledgements
The work was performed in part at the Center for Integrated Nanotechnologies and at the Bioscience Division, United States Department of Energy, Office of Basic Energy Sciences User Facility, Los Alamos National Laboratory, Los Alamos, New Mexico (Contract DE-AC52-06NA25396) and Sandia National Laboratories (Contract DE-AC04-94AL85000) and Physicians Medical Center, Santa Fe, New Mexico.
a
Although this technology platform is a derivative of alternating current redox magnetohydrodynamics4, 5 adapted for therapeutic wound healing interventions, it has been colloquially referred to as “nonablation radiofrequency” technology due to its use of standard electrosurgical generator power and cosmetic similarities to palliative tissue resection ablation devices.
This study was supported by the New Mexico Small Business Grant Program WNM700, RO122010, Los Alamos National Laboratory, Los Alamos, New Mexico and by NuOrtho Surgical, Inc., Fall River, Massachusetts. The authors wish to thank Sofiya N. Micheva-Viteva, PhD for assistance in RT-PCR assay design.
The authors IDM, REM, and WKA have declared potential conflicts of interest with respect to the authorship and/or publication of this article.