
Abstract
Soccer players and athletes in high-impact sports are frequently affected by knee injuries. Injuries to the anterior cruciate ligament and menisci are frequently observed in soccer players and may increase the risk of developing an articular cartilage lesion. In high-level athletes, the overall prevalence of knee articular cartilage lesions has been reported to be 36% to 38%. The treatment for athletic patients with articular cartilage lesions is often challenging because of the high demands placed on the repair tissue by impact sports. Cartilage defects in athletes can be treated with microfracture, osteochondral grafting, and autologous chondrocyte implantation. There is increasing scientific evidence for cartilage repair in athletes, with more extensive information available for microfracture and autologous chondrocyte implantation than for osteochondral grafting. The reported rates and times to return to sport at the preinjury level are variable in recreational players, with the best results seen in younger and high-level athletes. Better return to sport is consistently observed for all repair techniques with early cartilage repair. Besides minimizing sensorimotor deficits and addressing accompanying pathologies, the quality of the repair tissue may be a significant factor for the return to sport.
Keywords
Introduction
Defects of the joint cartilage have a very limited healing capacity. Therefore, injuries resulting from trauma or repetitive loading can lead to osteoarthritis over time. Soccer players and athletes in high-impact sports are particularly susceptible to knee injuries (

(
Cartilage Injury in Athletes
The prevalence of articular cartilage defects in athletes has not been well studied in the literature. Given the demands placed on the lower extremity during typical sports training and competition, these defects are likely to be symptomatic and potentially career threatening for most athletes. Some studies have investigated this issue in the knee but there is little evidence for the hip or ankle.
A recent systematic review of the prevalence of chondral defects in the athletes’ knees provides an overview of the literature to date on this topic. 8 This review of 11 studies including 931 athletes from American football, basketball, and endurance running recorded the overall prevalence of knee articular cartilage lesions to be 36%.15-25 The most common location was patellofemoral (37%), followed by the femoral condyle (35%) and tibial plateau (25%). Among patellofemoral lesions, the patella was more commonly involved (64%) than the trochlea (36%). Tibiofemoral lesions more commonly involved the medial compartment (68%) than the lateral compartment (32%). Fourteen percent of the athletes, all of whom were basketball players or endurance runners, were asymptomatic at the time of diagnosis. Among these athletes, the overall prevalence of knee articular cartilage lesions was 59% (reported range 18%–63%).
A very recent study of elite American football athletes reported an incidence of 38.2% among those who underwent magnetic resonance imaging (MRI) at the National Football League combine. 26 Only 53% of athletes at the combine underwent MRI imaging, so the overall reported prevalence was 20.1%, but this assumes there were no lesions in the 47% of athletes who were not imaged. Given the demands of American football on the knee joint, it is likely that at least some of these athletes had asymptomatic cartilage defects that were not imaged.
Although there has been one study reporting outcomes after surgical treatment for articular cartilage injury to the knee in soccer players, 27 there is little data on the incidence or prevalence of such lesions in this population. Articular cartilage injury is likely to be common in this population for a number of reasons, including the demands placed on the knee joint by soccer (football), the high incidence of knee injury in soccer (football), and the increased risk for knee osteoarthritis in former elite soccer players. The association of articular cartilage injuries with other injuries to the knee such as ACL or meniscal tears has been well established in the literature for athletes and the general population but is not a focus of this review. There is no published data on the epidemiology of hip and ankle focal articular cartilage lesions in athletes.
The limited evidence to date suggests there is a high prevalence of focal chondral defects in the knee even in the asymptomatic athlete. Because the natural history of these lesions is not known, the management of such lesions in asymptomatic athletes is challenging. If these lesions are or become symptomatic, the evolving treatment options for articular cartilage defects may be applied as indicated below. More studies are needed to better define the incidence and prevalence of full-thickness cartilage defects in the knee, hip, and ankle of athletes.
Cartilage Repair in Athletes
In recent years, a number of surgical approaches, including microfracture (MF), 28 autologous chondrocyte implantation (ACI), 29 and osteochondral transplantation (OATS) 30 have been developed for the repair of cartilage defects. The evidence for these different treatment modalities has been widely published. In the recent literature, 2 independent systematic reviews, one with 1400 athletes in 20 clinical trials (787 undergoing MF, 362 ACI, 261 OATS) 31 and the other with 730 athletes in 11 trials (447 MF, 183 ACI, 28 OATS), 32 have been published. The studies were homogenous in respect to study quality according to the Coleman methodology score (average 69.8 points) in all the parameters evaluated. The outcome parameter investigated was “return to sports on preinjury level” of the 3 above-mentioned cartilage repair techniques in the treatment of International Cartilage Repair Society (ICRS) grade III/IV defects in athletes’ knee joints. Additional interventions, mostly ACL and meniscal surgery, were noted in 50% of the patients in the review by Mithoefer et al. 31 compared with 32% of the cartilage repairs in the review by Harris et al. 32 The femoral condyles and the patellofemoral joint were the most commonly treated locations in both publications.
Microfracture
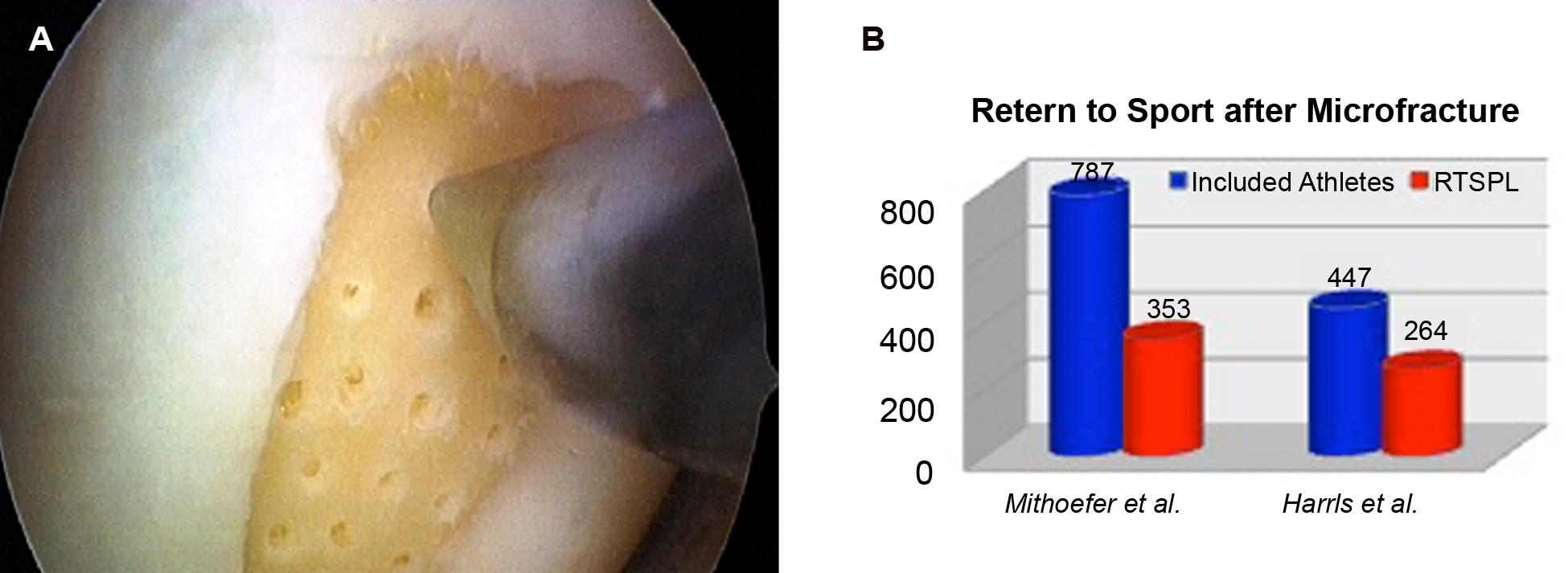
This method is one of the arthroscopic marrow stimulation techniques ( Figure 2A ) forming a clot of fibrin and precursor cells from the bone marrow. 28 Fibrous tissue with a histologic range from primitive scar tissue to fibrous–hyaline mixed cartilage tissue is generated under local biochemical and biomechanical factors.33,34 The advantage of this technique is the minimally invasive approach, which is easily executed in combination with the arthroscopic treatment of collateral injuries. Drawbacks of the technique are the inferior mechanical tissue properties, 35 and the formation of intralesional osteophytes,27,36 limiting midterm tissue durability.10,34,36,37 Active patients younger than 40 years with small defects, low body mass index, and a short duration of preoperative symptoms show the best results.27,33,38,41
(
Mithoefer and coworkers 31 evaluated the outcome of 787 patients with microfracture in 12 clinical trials. The mean Coleman methodology score in these studies equaled 65 (0–100) points. At a mean follow-up of 42 months and with a mean defect size of 3.6 cm2, an average of 66% (519 of 787) of the patients were able to participate in sports activities 8 months after surgery, 45% (353 of 787) of them at the preinjury level ( Figure 2B ). Harris and colleagues 32 in their review of 8 comparable publications with microfracture in 447 athletes arrive at slightly superior results, with 59% of the patients returning to their preinjury level of sports 17 months postoperatively ( Figure 2B ). Onset of symptoms of less than 12 months before surgery was associated with a significantly higher return to sports rate (67%) compared with a longer history of more than 12 months (14%). 10 The operative technique, follow-up, and patient’s characteristics as well as the rehabilitation protocols were comparable in both publications.
Autologous Chondrocyte Implantation
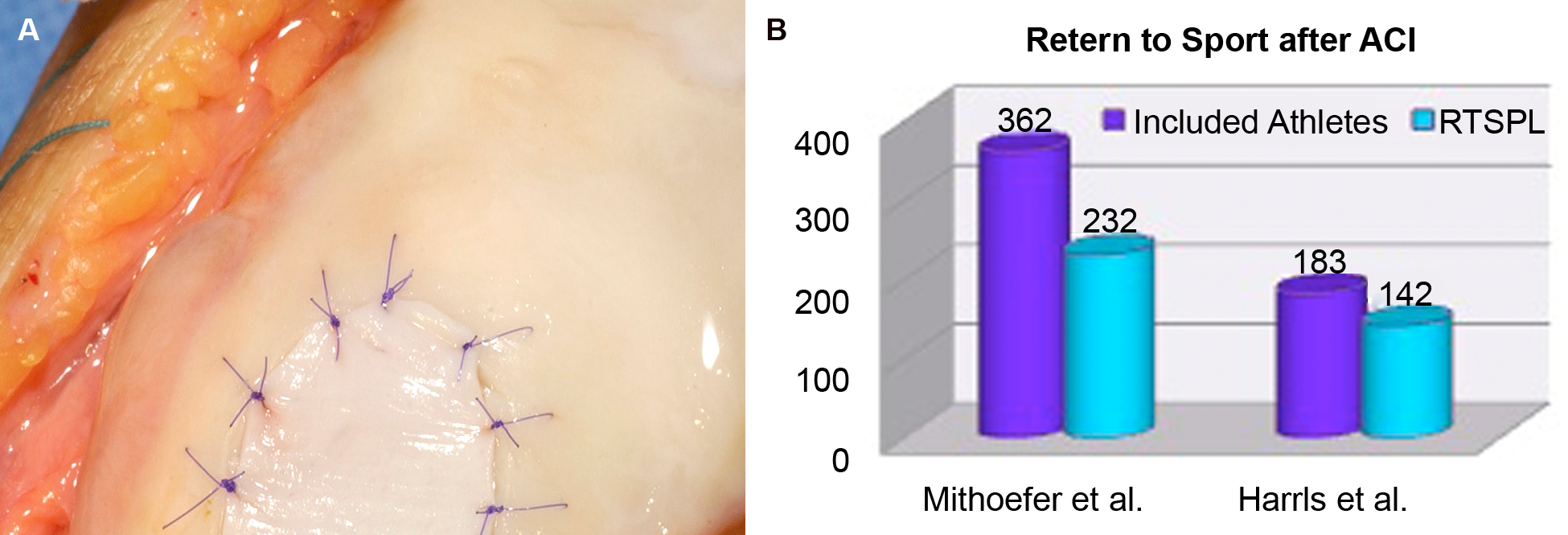
The technique developed by Lars Peterson 29 is based on tissue regeneration by isolated autologous chondrocytes. The native chondrocytes are harvested arthroscopically and cultured under standardized conditions. 42 During a second, open procedure, the cell suspension is implanted under a periosteum flap or a collagen membrane ( Figure 3A ).29,43,44 After a phase of adherence to the defect ground and proliferation of the cells, a primary tissue evolves that, during approximately 2 years, matures to histologically superior repair cartilage under the local biochemical and biomechanical conditions.45-47 Tissue specimens harvested from the regenerated areas demonstrate a histologic range from fibrous–hyaline mixed to hyaline-like repair tissue.33,34,38 More hyaline-like histologic quality seems to be essential for long-term durability of the tissue.34,35,48,49 Different modifications (ACT-P, ACT-C, MACT, etc.) of the original technique have been developed and evaluated short-term. The regeneration of the cartilage tissue can be described in 3 phases: I, Proliferation; II, Transition; III, Remodelling and Maturation. The rehabilitation process is adapted to this long process of tissue maturation, with impact sports being prohibited for 12–18 months after surgery.50,51 The advantage of this technique, besides the potential for histologically superior and stable repair tissue, is the capacity to address larger defects of more than 2 cm2. Disadvantages are the long rehabilitation process, high costs, and multiple procedures.
(
In the systematic review of Mithoefer et al., 31 7 ACI trials with 362 athletes and an overall mean follow-up of 42 months were identified. The mean Coleman methodology score was 77 points (0–100 points). Given an average defect size of 5.1cm2, 67% (242 of 362) of the patients were able to return to sports at 18 months, 64% (232 of 362) of them at the preinjury level ( Figure 3B ). Concomitant procedures were performed in 57% of the patients. The best durability of 96% (continued sport participation) was reported after ACI.
Harris and colleagues 32 analyzed 3 ACI trials with 183 athletes in their systematic review. An average of 78% (142 of 183) of the patients was able to participate in sports at their preinjury level 25 months postoperatively ( Figure 3B ). A short duration of symptoms (less than 1 year) and no previous interventions were associated with a significantly higher return to sports ratio.40,52
Osteochondral Transplantation
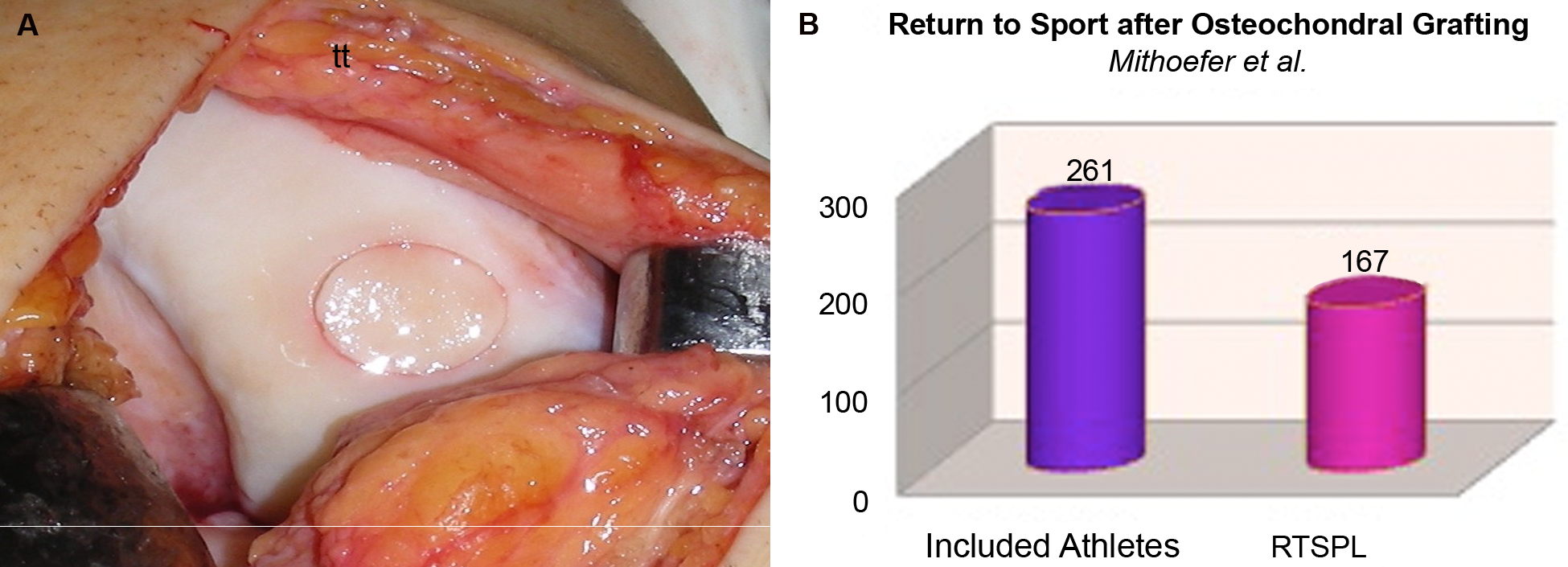
This technique uses osteochondral cylinders of 5 to 12 mm diameter and 15 to 20 mm length, harvested from low-stress areas of the joint to address small- and medium-sized chondral and osteochondral defects in a press-fit technique.53,54 The cartilage in this technique consists of hyaline tissue ( Figure 4A ). In contrast to the cell-based methods like microfracture and ACI, no maturation process of the tissue is required for establishing mechanical competence. After implantation, the transplanted tissue adapts structurally to the surrounding biomechanics. 55 As the osseous part of the cylinder has to be integrated, the rehabilitation protocol is similar to that established in fracture healing. For athletes, the advantages of this technique are the high tissue quality and the highly predictable integration of the cylinders besides a relatively short rehabilitation and limited costs. 54 Of disadvantage is the donor site morbidity, leading to complaints depending on the size and number of cylinders transplanted as well as the sometimes insufficient vertical integration of the cartilaginous component of the graft and the necessity for an open procedure. 56 Because of the limited number of available cylinders, this technique is suitable for defect sizes of less than 3 cm2.
(
Mithoefer and coworkers 31 analyzed 6 trials dealing with the OATS technique comprising 261 athletes with a follow-up of 42 months in their review. The Coleman methodology score equaled 71 points. Given a mean defect size of 2.4 cm2, 91% of the patients (238 of 261) were able to practice sports within 7 months of the operation, 64% (167 of 261) of them at the preinjury level ( Figure 4B ). The review of Harris et al. 32 comprises only 1 OATS trial that was evaluated in the Mithoefer et al. study.
Conclusion
Soccer players and athletes from other high-impact, pivoting sports are at risk for complex injuries involving the articular cartilage, ligaments, and menisci. Without differentiation by sport, the overall prevalence of knee articular cartilage lesions in professional athletes is estimated to be 36%. In athletes, the treatment of articular cartilage lesions is often challenging and associated with some limitations so that 45% to 78% of the athletes are able to return to sport at the preinjury level over a variable time period (7–25 months). The levels of evidence for ACI (mean Coleman methodology score 77 points), osteochondral transplantation (mean Coleman methodology score 71 points), and microfracture (mean Coleman methodology score 65 points) were acceptable, though limited for the autologous osteochondral grafting. The best evaluated technique is the microfracture (787 and 447 athletes), followed by the ACI (362 and 183 athletes) and the OATS (261 athletes). Superior results were found for ACI (64%–78% RTSPL), with the best durability but the longest mean time to return to sport (18 month), followed by OATS (64% RTSPL) and Microfracture (45%–67% RTSPL). The time from injury to surgery, the number of procedures and the quality of the repair tissue, as well as the successful treatment of accompanying pathologies, appears to be a significant factor influencing return to sport.
Footnotes
The authors received no financial support for the research, authorship, and/or publication of this article.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.