
Abstract
Objective:
Early surgical intervention for articular cartilage disease is desirable before full-thickness lesions develop. As early intervention treatments are designed, native chondrocyte viability at the treatment site before intervention becomes an important parameter to consider. The purpose of this study is to evaluate native chondrocyte viability in a series of specimens demonstrating the progression of articular cartilage lesions to determine if the chondrocyte viability profile changes during the evolution of articular cartilage disease to the level of surface fibrillation.
Design:
Osteochondral specimens demonstrating various degrees of articular cartilage damage were obtained from patients undergoing knee total joint replacement. Three groups were created within a patient harvest based on visual and tactile cues commonly encountered during surgical intervention: group 1, visually and tactilely intact surfaces; group 2, visually intact, tactilely soft surfaces; and group 3, surface fibrillation. Confocal laser microscopy was performed following live/dead cell viability staining.
Results:
Groups 1 to 3 demonstrated viable chondrocytes in all specimens, even within the fibrillated portions of articular cartilage, with little to no evidence of dead chondrocytes. Chondrocyte viability profile in articular cartilage does not appear to change as disease lesion progresses from normal to surface fibrillation.
Conclusions:
Fibrillated partial-thickness articular cartilage lesions are a good therapeutic target for early intervention. These lesions retain a high profile of viable chondrocytes and are readily diagnosed by visual and tactile cues during surgery. Early intervention should be based on matrix failure rather than on more aggressive procedures that further corrupt the matrix and contribute to chondrocyte necrosis of contiguous untargeted cartilage.
Introduction
Articular cartilage disease defines a large disease burden afflicting our population.1-5 Significant efforts continue in developing and tracking treatment solutions for articular cartilage lesions at various stages of their progression. 6 A considerable interest exists for effective surgical interventions that address an earlier stage of disease progression rather than waiting for full-thickness articular cartilage lesions to develop. Early surgical intervention is appealing for an aging population to mitigate downstream disease burden associated with full-thickness defects. Surgical treatment of fibrillated partial-thickness articular cartilage lesions remains an important category because these lesions can be readily diagnosed and characterized by visual and tactile cues during surgery and hence remain an attractive therapeutic target for early surgical intervention modalities.
Surgical treatment for fibrillated partial-thickness lesions has been traditionally limited to debridement chondroplasty techniques developed to remove the damaged articular cartilage that causes a mechanical and inflammatory impairment of joint function and leads to a deterioration of joint health. Smoothing the articular surface can eliminate the mechanical stress risers that cause symptoms and propagate cartilage damage; removal of the loose surface debris associated with loss of cartilage function decreases the biologic load the joint needs to address.7-11 Although an attractive surgical approach, current debridement chondroplasty techniques are imprecise, are aggressive, and induce necrosis and collateral damage to contiguous untargeted cartilage tissue at the treatment site.12-23 Accordingly, widespread adoption of current debridement chondroplasty techniques as an early surgical intervention modality to treat fibrillated partial-thickness lesions has not emerged due to the fear of contributing to disease progression resulting from an attempt to provide disease burden relief.
Because it is difficult to imagine an early surgical intervention for articular cartilage that does not include in situ removal of damaged tissue present at the lesion locale, researchers have sought to create more targeted interventions that are based on lesion progression. As early surgical intervention techniques become more precise and allow tissue preservation of articular cartilage, native chondrocyte viability at the treatment site before intervention becomes an important parameter to consider. The purpose of this study is to evaluate native chondrocyte viability in a series of specimens demonstrating the progression of articular cartilage lesions to determine if the chondrocyte viability profile changes during the evolution of articular cartilage disease to the level of surface fibrillation.
Materials and Methods
Osteochondral specimens were harvested from patients undergoing total knee replacement under an approved Institutional Review Board protocol. The total knee replacement procedures were performed by a single surgeon in the normal course of his practice. The tissue to be normally discarded during the procedure was examined prior to harvest once the knee joint was entered surgically to determine if it met the requirements for study inclusion. Specimens were included that demonstrated an area of uniform normal or partial-thickness damage of sufficient size to obtain test samples wherein harvest margin artifact would not be a confounding variable. 24 Three groups were created within each patient tissue harvest based on visual and tactile characteristics of the specimens as customarily assessed during surgery: group 1 included visually and tactilely normal cartilage surfaces, group 2 included visually normal but tactilely soft (as judged by indentation pressure) cartilage surfaces, and group 3 included surface fibrillation of the cartilage surfaces.
Immediately after harvest, three 0.5-mm coronal sections of each cartilage sample were obtained referencing the center of the sample after removal of subchondral bone. The sections were prepared for staining by washing in HEPES buffered saline solution. Live/Dead® Reduced Biohazard Cell Viability Kit 1 “green and red fluorescence,” SKU #L-7013 (Invitrogen, Carlsbad, California), was used per the manufacturer’s specification to stain specimens. Specimens were gluteraldehyde fixed, transferred to standard flat glass slides, and flooded with VectaShield® fluorescence protection oil prior to the placement of #1.5 borosilicate glass coverslips over each specimen section.
The cartilage tissue and the articular surface were assessed by confocal fluorescence laser microscopy analysis performed by personnel blinded to the identity of the samples. Confocal imaging was performed with an Olympus IX-81 inverted microscope coupled to an Olympus FV300 confocal laser scanning unit (Center Valley, Pennsylvania) using 488-nm laser excitation. Live chondrocytes were captured under green fluorescent channel (505-525 nm), and dead chondrocytes were captured under red fluorescent channel (577-634 nm), generating a live image, a dead image, and an integrated image.
Results
Six separate osteochondral specimens originating from femoral condyle resection were included for study (n = 6), with 2 specimens per group.
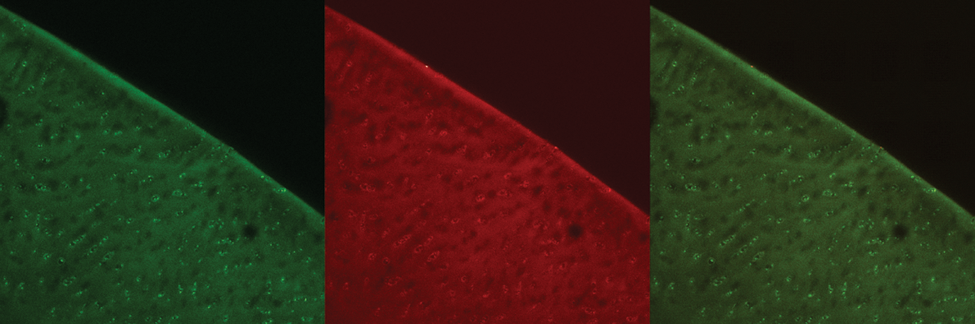
Confocal laser microscopy images, group 1. Representative images depicting live cell stain (green), dead cell stain (red), and a combined image with both live cell and dead cell stain. Original magnification 10x.
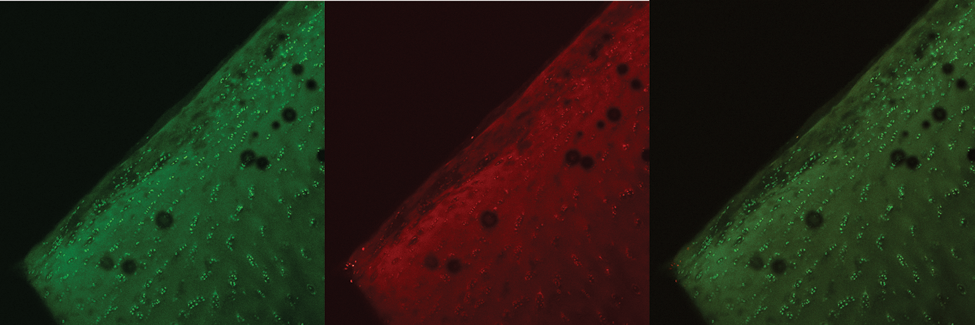
Confocal laser microscopy images, group 2. Representative images depicting live cell stain (green), dead cell stain (red), and a combined image with both live cell and dead cell stain. Original magnification 10x.
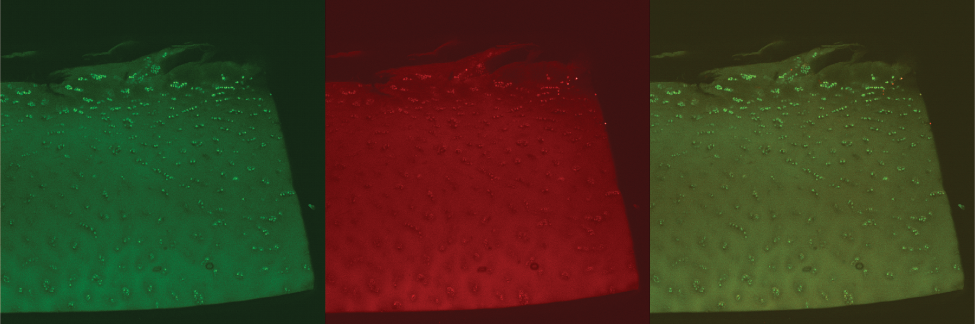
Confocal laser microscopy images, group 3. Representative images depicting live cell stain (green), dead cell stain (red), and a combined image with both live cell and dead cell stain. Original magnification 10x.
Group 1 specimens (
Group 2 specimens (
Group 3 specimens (
Discussion
This study explored chondrocyte viability in tissue specimens demonstrating various levels of articular cartilage lesion progression in patients undergoing joint replacement surgery. Although a small sample size, the results indicate that articular cartilage retains a very high percentage of native viable chondrocytes even when lesion progression has led to matrix failure and subsequent surface fibrillation within the same patient. Because of the predominant chondrocyte viability noted, surface fibrillation appears to be an important stage to consider for early surgical intervention—a stage that can be readily diagnosed by visual and tactile cues during surgery.
Matrix failure–based early intervention for articular cartilage disease should be considered a therapeutic target because preserving functioning cartilage tissue is important. Injury and loss of the superficial zone has been strongly associated with the progression of cartilage disease,25-29 and treatments that contribute to superficial zone injury accelerate the natural progression and disease burden of osteoarthritis.25,29-33 Once articular cartilage lesions have progressed to matrix failure leading to surface fibrillation, those chondrocytes within the fibrillation, although noted to be viable in this study, may be not be useful to retain considering that fibrillation matrix stress risers can cause additional chondrocytes to become extruded as untreated fibrillation lesions propagate in response to additional loading.34-41 Stabilizing superficial zone lamina flaps, cleavage planes, and the peeling or breaking of denatured collagen fibrils can be a reasonable matrix failure–based therapeutic target. From an early surgical intervention perspective, precisely removing this fibrillated tissue as a means to stabilize lesions is preferable, as long as the underlying intact chondrons are not injured, because it has been noted that spatial reorganization and proliferation of superficial zone chondrocytes occur in response to distant partial-thickness lesions and may serve as a mechanism to recruit metabolically active units to address focal disease. 42
Although many studies have supported the efficacy of debridement chondroplasty in relieving patient symptoms by smoothing the articular surface and decreasing the biologic load of joint cartilage debris,7-11 these benefits have yet to be shown to contribute to long-term joint health, to promote cartilage longevity, or to mitigate joint replacement surgery. This may be due to the nature of current interventions that are excessively damaging to these lesions and notably contribute to disease progression.12-23 If iatrogenic cartilage damage can be eliminated during debridement chondroplasty, whereby superficial zone chondrocytes at or around the lesion are preserved, the opportunity to effect beneficial changes in chondrocyte function remains in that resident cell function may be recruited to aid healing.42-47 Even though other experimental techniques have failed to show a significant repair response of native chondrocytes within partial-thickness lesions,48-50 further study is required to determine whether early surgical intervention treatments that preserve and stabilize tissue permit or even induce a normal healing response.
Footnotes
Acknowledgments and Funding
The work was performed at the Center for Integrated Nanotechnologies, United States Department of Energy, Office of Basic Energy Sciences User Facility, Los Alamos National Laboratory, Los Alamos, New Mexico (Contract DE-AC52-06NA25396) and Sandia National Laboratories (Contract DE-AC04-94AL85000) and Physicians Medical Center, Santa Fe, New Mexico. This study was supported by the New Mexico Small Business Grant Program WNM700, RO31, Los Alamos National Laboratory, Los Alamos, New Mexico, and by NuOrtho Surgical, Inc., Fall River, Massachusetts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.