
Abstract
Objective
The objective of the study was to compare postoperative patient-reported outcomes and reoperation rates following unicompartmental knee arthroplasty (UKA) between patients with full-thickness cartilage loss (FTCL) and partial-thickness cartilage loss (PTCL).
Design
Multiple databases, including PubMed, Embase, Cochrane Library, and CNKI, were searched until October 2019 for studies comparing the Oxford Knee Score (OKS), American Knee Society (AKS) score, and reoperation rates between patients with FTCL and PTCL following UKA. Data analysis was performed using Review Manager software.
Results
A total of 613 UKA cases from 5 retrospective cohort studies were included. The mean difference in postoperative OKSs was significantly higher by 2.92 in FTCL group than in PTCL group (95% confidence interval [CI] = −5.29 to −0.55; P = 0.02). Improvement in OKS was significantly higher by 2.69 in FTCL group than in PTCL group (95% CI = −4.79 to −0.60; P = 0.01). However, the differences in OKSs were not clinically significant. The mean difference in AKS knee scores was similar between the 2 groups (95% CI = −9.14 to −3.34; P = 0.36), whereas the pooled mean difference in AKS function scores was higher by 5.63 in FTCL group than in PTCL group (95% CI = −9.27 to −1.98; P = 0.002), which was clinically relevant. The reoperation rates were statistically higher in PTCL group than in FTCL group (odds ratio = 2.24; 95% CI = 1.15 to 4.38; P = 0.02).
Conclusions
Patients with FTCL achieved superior postoperative patient-reported outcomes and lower reoperation rates following UKA compared with those with PTCL. Thus, we believe this procedure should only be applied to end-stage medial osteoarthritis of the knee joint.
Keywords
Background
Knee osteoarthritis (KOA), which is one of the most common diseases worldwide, is a leading cause of disability and decreased quality of life in older adults. 1 With the rapid increase in the proportions of obese and older adults, the prevalence of KOA has also increased. Approximately 18% of the Chinese population suffers from KOA, and >70% of older adults (aged >60 years) have shown different degrees of KOA. Consequently, the social burden due to KOA has been increasing.1,2 So far, several methods have been proposed to prevent or treat different stages of KOA, such as functional exercise, avoiding weightbearing, oral nonsteroidal drugs, Chinese herbal medicine, joint injection, arthroscopy, knee osteotomy, and joint replacement. 3
Among the abovementioned methods, unicompartmental knee arthroplasty (UKA) is a feasible alternative for treating KOA and spontaneous osteonecrosis of the knee (SONK).4 -7 As patients with partial-thickness cartilage loss (PTCL) may have inferior postoperative patient-reported outcomes and high reoperation rates, we usually recommend performing UKA in patients with full-thickness cartilage loss (FTCL) in the medial compartment of the knee, which is a condition staged as grade 4 in the Kellgren and Lawrence classification (as indicated by obliteration of the joint space and “bone-to-bone” abrasion on a standing anterior-posterior [AP] radiograph). 8 Goodfellow stated that compared with patients with FTCL, those with PTCL have variable outcomes, and some of them do not benefit from the operation in the short term8,9 although there is no evidence to support this finding. Some surgeons have also performed UKA in KOA patients with PTCL and indicated that they achieved acceptable outcomes. 10
This meta-analysis aimed to compare postoperative patient-reported outcomes and reoperation rates following UKA between patients with FTCL and PTCL. We surmised that patients with FTCL were associated with better patient-reported outcomes and lower reoperation rates than those with PTCL.
Methods
This meta-analysis was conducted in accordance with the recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-analyses guidelines. 11
Search Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement was followed. 12 Two investigators (Y.Y. and J.M.) independently searched multiple comprehensive databases, including PubMed, Embase, the Cochrane Library, and CNKI, until October 2019 for studies comparing postoperative patient-reported outcomes and reoperation rates between patients with FTCL and PTCL following UKA. The following 3 categories of keywords (and related synonyms) were used to develop a sensitive search strategy and provide a systematic review: “unicompartmental knee arthroplasty,” “cartilage loss,” and “outcome.” There were no restrictions on language, year of publication, or type of publication. These terms were searched in the “all fields” item to expand the literature search. We used Medical Subject Headings words when searching PubMed and combined all synonyms relevant to the keywords by applying the Boolean command “OR.” Furthermore, search terms were truncated with a “*” symbol to obtain all terms beginning with a specific word. After the initial electronic search, relevant articles and their bibliographies were manually assessed. These articles were then evaluated individually for inclusion.
Inclusion Criteria and Study Selection
All studies included in this meta-analysis were independently reviewed and selected by 2 authors according to predefined inclusion criteria. Titles and abstracts were screened for eligibility; if suitability could not be determined, the full article was evaluated. The inclusion criteria were as follows: (1) published, full-text, peer-reviewed articles; (2) randomized controlled trial or cohort study; (3) studies comparing the postoperative patient-reported outcomes or reoperation rates between patients with various degrees of cartilage injury or joint space loss following UKA; (4) postoperative outcome assessed using at least 1 of the 3 parameters: Oxford Knee Score (OKS), American Knee Society (AKS) score, or reoperation rate; (5) number of patients in each group (FTCL and PTCL) and the means and standard deviations of the abovementioned parameters were fully reported; (6) use of adequate statistical methods to compare the parameters between the 2 groups; and (7) eligible for pooling data for meta-analysis. The exclusion criteria were as follows: (1) unpublished articles or those with unavailability of full text; (2) case-control studies, case series or reports, or reviews; (3) animal, cadaver, or laboratory studies; and (4) studies with incomplete, inconsistent, or irreproducible data. Where there was disagreement or doubt, the full article was reviewed by 2 authors. Disagreements were resolved by discussion with each other. The corresponding author was consulted in cases of unresolved disagreement.
Methodological Quality
The Jadad score was used to assess the methodological quality of each study. This score consists of items related to randomization appropriateness, blinded outcome assessment, and complete description of loss to follow-up, all of which were used to assess the quality of the 5 included studies. 13 We then examined each component of the Jadad score as a study-level factor to determine whether it affected the heterogeneity of the results. The corresponding author was consulted in cases of unresolved disagreement.
Data Extraction
Two authors independently extracted the following information from the included studies: (1) author, year, country/region, and number of references; (2) study design and time of follow-up; (3) study population, cohort, age, sex, body mass index (BMI), and comorbidities; (4) scoring scale used to evaluate rehabilitation; (5) definition of different outcomes; and (6) confounding factors related to postoperative outcomes and reoperation rates, such as sex, BMI, complications, preoperative function of sports, surgeon implication, or other psychosocial influencing factors.
Statistical Analysis
Heterogeneity among studies was evaluated using I 2 tests. If I 2 was ≤50%, the study was considered to have low heterogeneity and a fixed-effects model was employed; otherwise, the random-effects model was used. The mean difference and 95% confidence intervals (95% CIs) were calculated for continuous outcomes, whereas odds ratios (ORs) and 95% CI were calculated for binary outcomes. A P value of <0.05 was considered to indicate statistical significance. Potential publication bias was assessed using the Egger regression asymmetry test. All statistical analyses were performed using the Review Manager software from the Cochrane Collaboration (version 5.3.) and Stata software (version 16.0.).
Results
Study Inclusion
In total, 381 studies were obtained through the initial search (376 via an electronic database and others via other sources). After the removal of duplicates, 364 records remained, 352 of which were excluded for 2 reasons: no direct comparison between PTCL and FTCL cases (n = 351) and a lack of uniformed outcome measurement (n = 1). The full text of the remaining 12 articles was further reviewed for more details, and 7 of them were excluded as they could not distinguish PTCL and FTCL cases with conceivable criteria. Thus, 5 studies were included in this meta-analysis. The flow diagram of the study selection procedure is shown in Figure 1 .
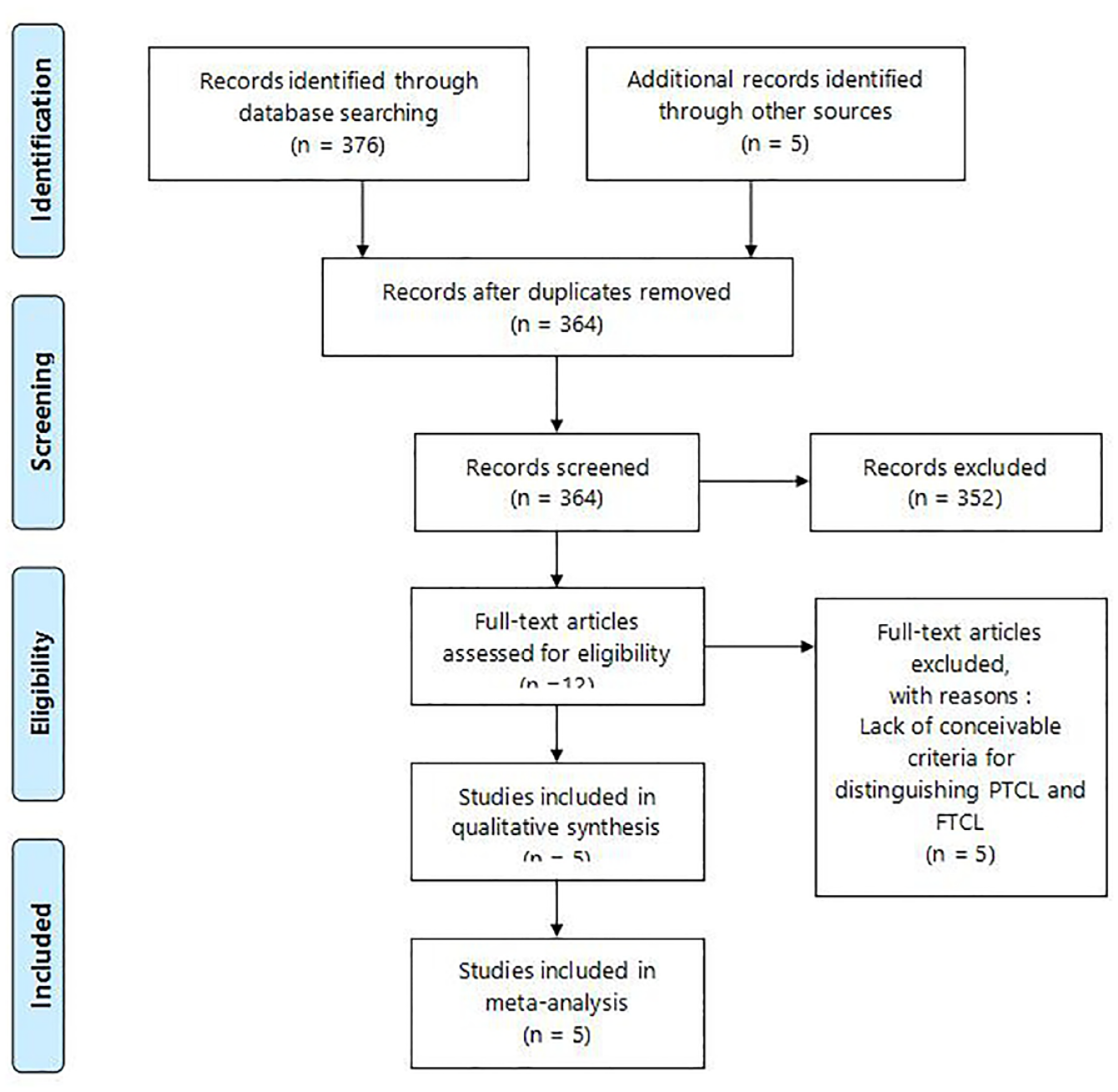
Flow chart of the literature search. FTCL = full-thickness cartilage loss; PTCL = partial-thickness cartilage loss.
Study Characteristics and Patient Populations
The 5 selected studies included 233 knees with PTCL and 380 knees with FTCL who underwent medial compartment UKA. Three studies compared OKSs, among which 2 studies also compared the AKS knee and function scores. Furthermore, the reoperation rates in all 5 studies were compared. The detailed sample size and measured parameters are presented in Table 1 .
Characteristics of the Included Studies.
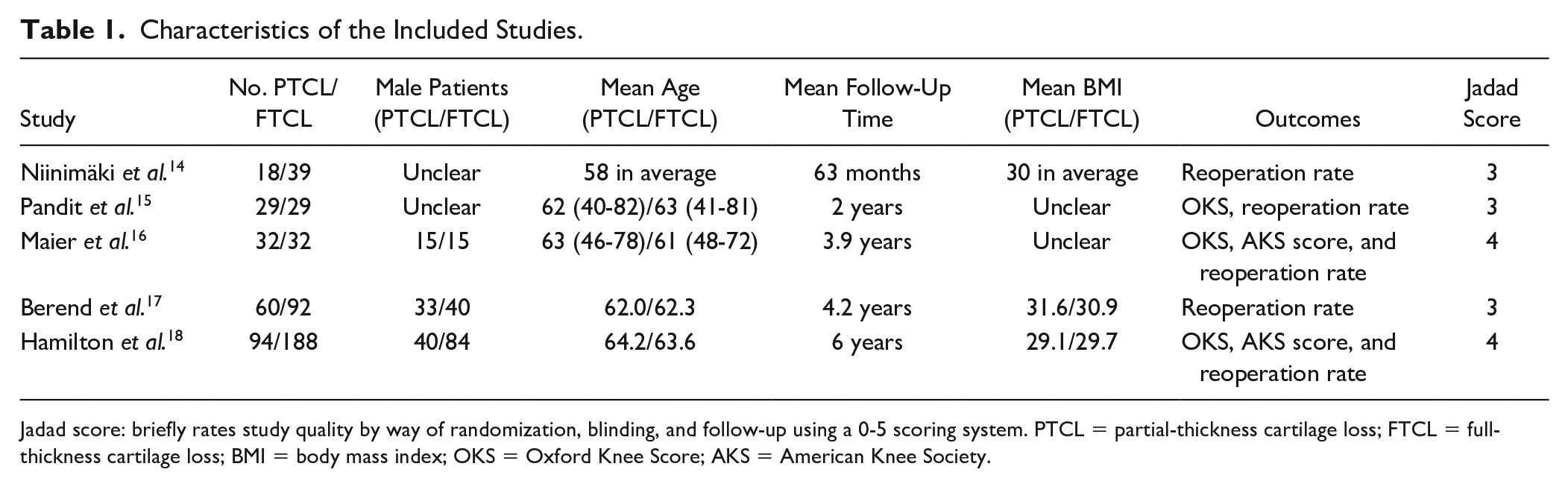
Jadad score: briefly rates study quality by way of randomization, blinding, and follow-up using a 0-5 scoring system. PTCL = partial-thickness cartilage loss; FTCL = full-thickness cartilage loss; BMI = body mass index; OKS = Oxford Knee Score; AKS = American Knee Society.
Quality of the Included Studies
All 5 studies included in this meta-analysis showed a low risk of selection bias. Considering that the number of patients who underwent UKA with PTCL was lower than that who underwent UKA with FTCL,19,20 2 studies (Niinimäki et al. 14 and Berend et al. 17 ) compared consecutive UKA cases. One study (Hamilton et al. 18 ) followed consecutive PTCL-defined UKA patients and matched them with those who had FTCL in the knee in a ratio of 1:2 by age, sex, and preoperative OKS. Two other studies (Pandit et al. 15 and Maier et al. 16 ) reviewed a hospital database to identify patients with PTCL and created a matched control group according to sex, preoperative OKS, age at operation, and time to follow-up. However, 2 studies (Berend et al. 17 and Hamilton et al. 18 ) had a high risk of attrition bias because of the high proportion of patients lost to follow-up (13% and 44% each in the second year). All 5 studies were assumed to have a moderate level of comparability, considering the existence of controls for additional factors. Table 2 summarizes the quality assessment of the included studies in this meta-analysis. In addition, the Egger regression asymmetry test was used to evaluate publication bias, revealing that the possibility of file drawer bias was extremely low (P > 0.05).
Risk of Bias Summary: Review Authors’ Judgment About the Risk of Bias for Items in Included Studies.
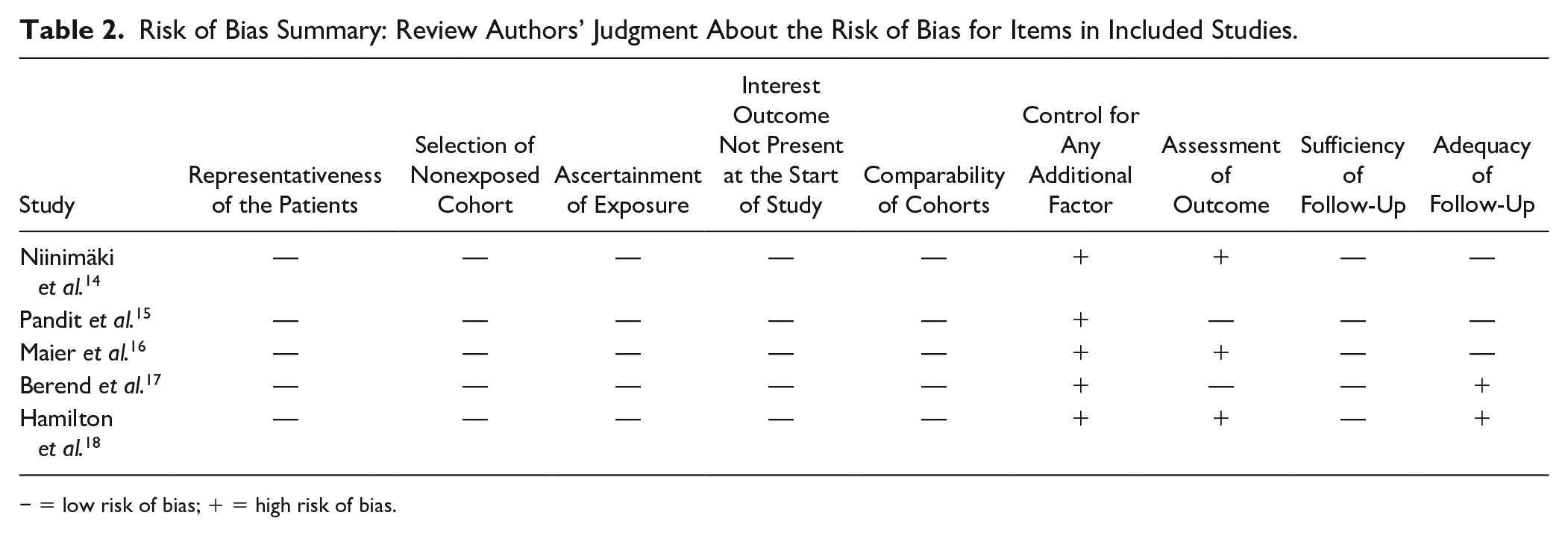
− = low risk of bias; + = high risk of bias.
OKS
Three studies compared postoperative OKSs in PTCL and FTCL groups at a follow-up of ≥2 years.15,16,18 The pooled mean difference in postoperative OKSs was −2.92 (95% CI = −5.29 to −0.55; P = 0.02; I 2 = 53%; Fig. 2 ), indicating that the postoperative OKS in FTCL group was significantly higher by 2.92 than that in PTCL group. However, the difference was not clinically significant as the minimal clinically important difference (MCID) for OKS was 5 points.

Forest plots of studies comparing postoperative OKSs between PTCL and FTCL groups. OKS = Oxford Knee Score; PTCL = partial-thickness cartilage loss; FTCL = full-thickness cartilage loss; IV = intravenous; CI = confidence interval.
AKS
Two studies assessed AKS knee and function scores in PTCL and FTCL groups, at a mean follow-up of >3.9 years.16,18 The pooled mean difference in AKS knee scores was −2.90 (95% CI = −9.14 to −3.34; P = 0.36; I 2 = 67%; Fig. 3 ), indicating that it was similar between the 2 groups. In contrast, the pooled mean difference in postoperative AKS function scores was 5.63 higher in FTCL group than in PTCL group (95% CI = −9.27 to −1.98; P = 0.002; I 2 = 0%; Fig. 4 ), which was also clinically relevant.

Forest plots of studies comparing postoperative AKS knee scores between PTCL and FTCL groups. AKS = American Knee Society; PTCL = partial-thickness cartilage loss; FTCL = full-thickness cartilage loss; IV = intravenous; CI = confidence interval.

Forest plots of studies comparing postoperative AKS function scores between PTCL and FTCL groups. AKS = American Knee Society; PTCL = partial-thickness cartilage loss; FTCL = full-thickness cartilage loss; IV = intravenous; CI = confidence interval.
Reoperation Rate and Revision Surgery
All 5 studies presented data on reoperation rates, which included arthroscopy, replacement of meniscal bearing, revisions to total knee arthroplasty (TKA), and open exploration.14 -18 Accordingly, 39 reoperations were reported in 613 knees (21 [9%] in 233 knees with PTCL and 18 [4.7%] in 380 knees with FTCL, respectively). The pooled results showed that the reoperation rate was statistically higher in the PTCL group than in the FTCL group (21/233 vs. 18/380; OR = 2.24; 95% CI = 1.15 to 4.38; I 2 = 0%; Fig. 5 ).
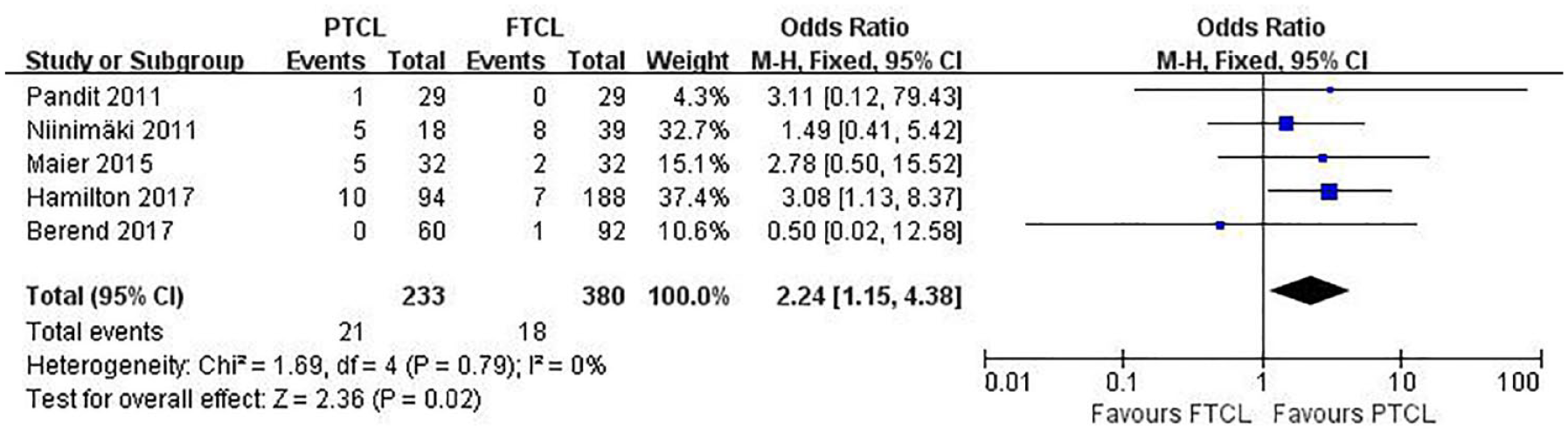
Forest plots of studies comparing reoperation rate between PTCL and FTCL groups. PTCL = partial-thickness cartilage loss; FTCL = full-thickness cartilage loss; CI = confidence interval; M-H = Mantel-Haenszel.
Although the distribution of revision surgeries was not available in the retrospective study by Niinimäki et al., 14 the other 4 studies reported 12 revision surgeries (9 and 3 revision surgeries in PTCL and FTCL groups, respectively). In the PTCL group, Maier et al. 16 reported 5 revisions, including an exchange of polyethylene inlay because of early infection (21 days), a TKA because of infection (44 weeks), a TKA after clinically and radiologically detected loosening with associated pain (12 months), and 2 arthroscopic procedures for associated pain (12 and 13 months each). 16 Hamilton et al. 18 reported 4 revisions at a mean follow-up of 5.9 (range = 0.9-10.3) years. Of these, 2 revisions were performed for the progression of OA, one of them involved the addition of a lateral UKA (6.3 years) and the other involved revision to a TKA (10.3 years); one revision was performed for loosening of the femoral component (7.2 years); and one was performed for persistent pain (0.9 years). The latter two revision surgeries were converted to TKA. 18 The FTCL group reported 3 revisions in total, including an open revision because of fixed Redon drainage (3 days), a TKA because of loosening of the femoral component (7.9 years), and a TKA for arthrofibrosis.
Changes in OKS
Based on the data regarding preoperative and postoperative OKS available in 3 studies,15,16,18 we compared the improvement in OKS between the PTCL and FTCL groups after a follow-up of ≥2 years. The pooled mean difference in the change in OKS was −2.69 (95% CI = −4.79 to −0.60; P = 0.01; I 2 = 50%; Fig. 6 ), indicating that the improvement in OKS was significantly higher by 2.69 in FTCL group than in PTCL group. However, the difference was not clinically significant according to the MCID for OKS.
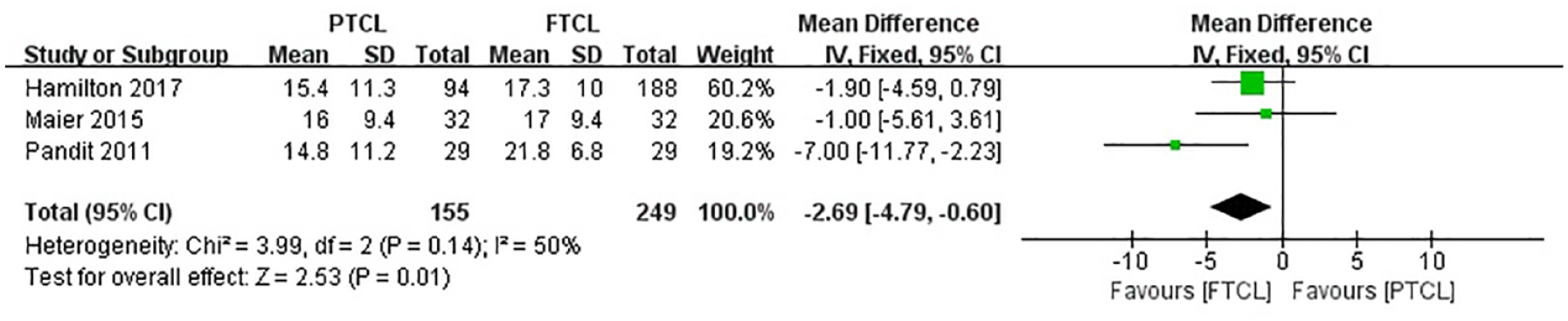
Forest plots of studies comparing the change in OKS between PTCL and FTCL groups. OKS = Oxford Knee Score; PTCL = partial-thickness cartilage loss; FTCL = full-thickness cartilage loss; IV = intravenous; CI = confidence interval.
Discussion
This meta-analysis aimed to compare postoperative patient-reported outcomes and reoperation rates following UKA between patients with FTCL and PTCL. We revealed that patients with FTCL were associated with better patient-reported outcomes and lower reoperation rates than those with PTCL. To the best of our knowledge, no similar meta-analysis has been conducted to compare the outcomes of patients with PTCL and FTCL following UKA. The findings of this meta-analysis indicated that the postoperative OKSs and AKS function scores were significantly higher in the FTCL group than in the PTCL group after UKA. Based on the change in OKS, UKA procedure was more beneficial in the FTCL group than in the PTCL group. The pooled mean difference in postoperative AKS knee scores was also higher in FTCL group than in PTCL group, but the difference was not statistically significant. However, the reoperation rate was higher in the PTCL group than in the FTCL group.
Goodfellow believed that the concept of no “bone-to-bone” abrasion (FTCL) in the medial compartment of the knee was a contraindication of UKA; therefore, orthopedists were recommended to evaluate cartilage loss thickness in the medial compartment of the knee using varus-stressed radiographs. If these radiographs failed to demonstrate “bone-to-bone” abrasion between the medial femoral condyle and medial tibial plateau, UKA should not be performed.8,9 The results of this meta-analysis supported the abovementioned finding. Accordingly, we concluded that patients with PTCL are not equally suitable for treatment with UKA as patients with “bone on bone” abrasion, which was consistent with the findings reported by Hamilton et al. 18 and Maier et al. 16
Surgeons routinely assess the severity of OA in the medial compartment using AP weightbearing radiographs. UKA is recommended when “bone-to-bone” abrasion is observed within the knee. 8 However, several patients with severe pain and limited function have extensive and substantial cartilage damage in the medial compartment but do not have “bone on bone” abrasion. If these patients continuously exhibit severe symptoms despite conservative and arthroscopic interventions, the next logical therapeutic intervention would be high tibial osteotomy or UKA. 15 Thus, further assessment using Rosenberg radiographs, 21 varus stress radiographs, and arthroscopy may be required when dealing with FTCL. 22 In addition, in several other institutions, when patients have persistent pain and PTCL is detected on the radiograph, arthroscopy is performed. When severe cartilage damage is noted in the medial compartments and the remainder of the knee is in good condition, UKA is performed. 14 The worse patient-reported outcomes and higher failure rates in patients with PTCL may be attributed to patient-related factors or the indication for UKA. 15 We assumed that patients who sought operative treatment with only partial cartilage damage had lower levels of tolerance to pain and higher expectations for postoperative outcomes,15,23 which may have led to the differences in postoperative recovery. Another possible explanation for worse patient-reported outcomes and higher failure rates in patients with PTCL is that the cause of knee pain in the early phase of OA was different from that in the end stage. 24 We believe that the mere thinning of the cartilage and surface fibrillation with marginal osteophytes cannot reliably explain the disabling pain. Synovial inflammation and the release of biological mediators instead of cartilage damage could primarily explain the association of pain with PTCL. 25 However, severe KOA mechanical factors are a more significant source of pain.26 -28 When FTCL in the medial compartment of the knee cannot be proved, we should consider other causes for the persistent pain (e.g., spine pathology, hip OA, or rheumatics). 22
Furthermore, we should only consider anteromedial OA as the probable cause of persistent intolerable knee pain when the cartilage buffering ability between the medial femoral condyle and medial tibial plateau lessens significantly. Then, UKA should be performed to treat end-stage KOA and SONK and be expected to provide a superior outcome. When performing UKA in patients with PTCL, we cannot remove the source of knee pain and consequently achieve an unacceptable outcome, which may necessitate one or more reoperations. 18 In fact, the main reason for reoperation in the 5 included studies was unresolved knee pain.14,16,18 When a patient’s main complaint (pain in the majority) is not resolved, they may request further treatment (reoperation). This may be the reason for higher OKSs and AKS knee scores in the FTCL group, although the differences were not significant. Furthermore, alleviation of knee pain will certainly accelerate the recovery of knee function and return to physical activity,29,30 as indicated by higher AKS function scores in FTCL group.
Historically, indications for UKA have been controversial.8,31 Although FTCL in the medial compartment of the knee has been widely accepted as an indication of UKA,6,7 some orthopedists believe that this operation can achieve good and similar outcomes in patients with PTCL to those in patients with FTCL. 17 Several studies have reported varying conclusions based on different designs.14 -18 Our meta-analysis indicated that the differences between the outcomes of the 2 groups were significant, suggesting that UKA should be performed in patients with “bone-to-bone” abrasions, which is the end stage of KOA. Based on the results of this meta-analysis, we recommend performing other operations such as high tibial osteotomy instead of UKA to treat patients with PTCL.
There were certain inevitable limitations in this study. First, some studies may have been overlooked. To avoid this problem, we performed an extensive search with sensitive keywords and synonyms in multiple comprehensive databases and used the expertise of a clinical librarian. Furthermore, the Egger regression test was performed to identify potential file drawer bias. Second, all included studies were cohort studies, which will inevitably inherit the defects of observational comparison studies and result in some inherent heterogeneity because of uncontrolled bias. 32 In addition, the heterogeneity among studies may have been due to slight differences in other confounding factors such as BMI, follow-up time, and diagnostic methods for FTCL and PTCL. Although systematic reviews with meta-analysis are usually considered to be “high-quality evidence,” we believe that our findings are, at most, of moderate quality when considering the limitations above. Finally, according to the outcome measures, several patient-reported questionnaires such as OKS and AKS were used. Because of the high dependency on the patients’ abilities to describe their daily activities several years ago, this type of research is prone to “recall bias.” Moreover, most of the descriptions of outcomes were not and probably could not be validated.
Conclusion
Our systematic review and meta-analysis showed that patients with FTCL achieved superior postoperative patient-reported outcomes and lower reoperation rates compared with patients with PTCL. We believe that patients with PTCL in the medial compartment of the knee should not be an indication for UKA.
Footnotes
Author Contributions
BW and WW conceived and designed the study. JM and YY searched and selected relevant studies. BW and WW extracted and interpreted data. JM and YY analyzed the data. JM and YY wrote the paper. DY and WG critically reviewed and approved the final manuscript.
Acknowledgment and Funding
The project was supported by grants from the Fundamental Research Funds for the Central Universities (No.3332021088) and Elite Medical Professionals project of China-Japan Friendship Hospital (No. ZRJY2021-TD01).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Consent for Publication
All the authors have approved the manuscript for publication.
Availability of Data and Material
All data generated and analyzed during the study are available from the corresponding author upon request.