
Abstract
A 64-year-old man with a history of diabetes mellitus and end stage renal disease presented with a several day history of cognitive decline, reduced right eye visual acuity accompanied with a complete right ophthalmoplegia in keeping with orbital apex syndrome. Initial MRI was unremarkable other than mucosal thickening in the frontal sinuses. He continued to clinically decline and repeat MRI revealed an edematous right optic nerve and a lack of enhancement within the sinuses was suspicion for invasive fungal infection. Given his history of diabetes, he was started on anti-fungal treatment and taken for debridement but passed away several days later. This case illustrates the importance of the orbital apex syndrome as a localization. Mucormycosis should be considered in acute onset ophthalmoplegia particularly in patients with diabetes and diabetic ketoacidosis. Empiric anti-fungal therapy should be started early for suspected rhino-orbital cerebral mucormycosis, although mortality remains high despite treatment.
Practical Implications
Orbital Apex syndrome is an important localization for neurologists, in addition to its differential diagnosis
Mucormycosis should be considered in acute onset ophthalmoplegia, with or without vision loss and reduced level of consciousness, particularly in patients with diabetes and diabetic ketoacidosis
The black turbinate sign on magnetic resonance imaging can be helpful in diagnosis of invasive fungal rhinosinusitis
Normal imaging with CT and MRI does not exclude invasive fungal rhinosinusitis and repeat imaging with gadolinium and dedicated orbital imaging should be considered if there is strong clinical suspicion
Empiric anti-fungal therapy should be started early for suspected rhino-orbital cerebral mucormycosis, although mortality remains high despite treatment
A 64-year-old male with poorly controlled type 2 diabetes and end-stage renal disease on peritoneal dialysis was admitted to a peripheral hospital with increasing shortness of breath and hyperosmolar hyperglycemic state (HHS). Past medical history otherwise included treated latent tuberculosis and hypertension. The patient was previously functioning independently at home but presented with 3 to 4 days of shortness of breath with exertion as well as general confusion including leaving the stove on more than once. He was treated with an insulin infusion for HHS and transferred to our institution for peritoneal dialysis.
The neurology service was consulted for worsening level of consciousness over the course of a day after admission. On examination, he was afebrile with an elevated blood pressure of 180/90 mmHg. He was drowsy but able to respond to basic orientation questions andd was obeying commands with stimulation. His right pupil was 3-4 mm and left 2-3 mm, otherwise reactive to light, and he was tending to visual stimuli with roving eye movements in all directions. He was moving all 4 limbs spontaneously and had no evidence of meningismus. Reflexes were normal aside from absent ankle reflexes, with flexor plantar responses. CT head was unremarkable other than chronic small vessel ischemic changes. MRI brain (Figure 1A and B) revealed no acute parenchymal abnormality and again demonstrated mild microvascular changes.
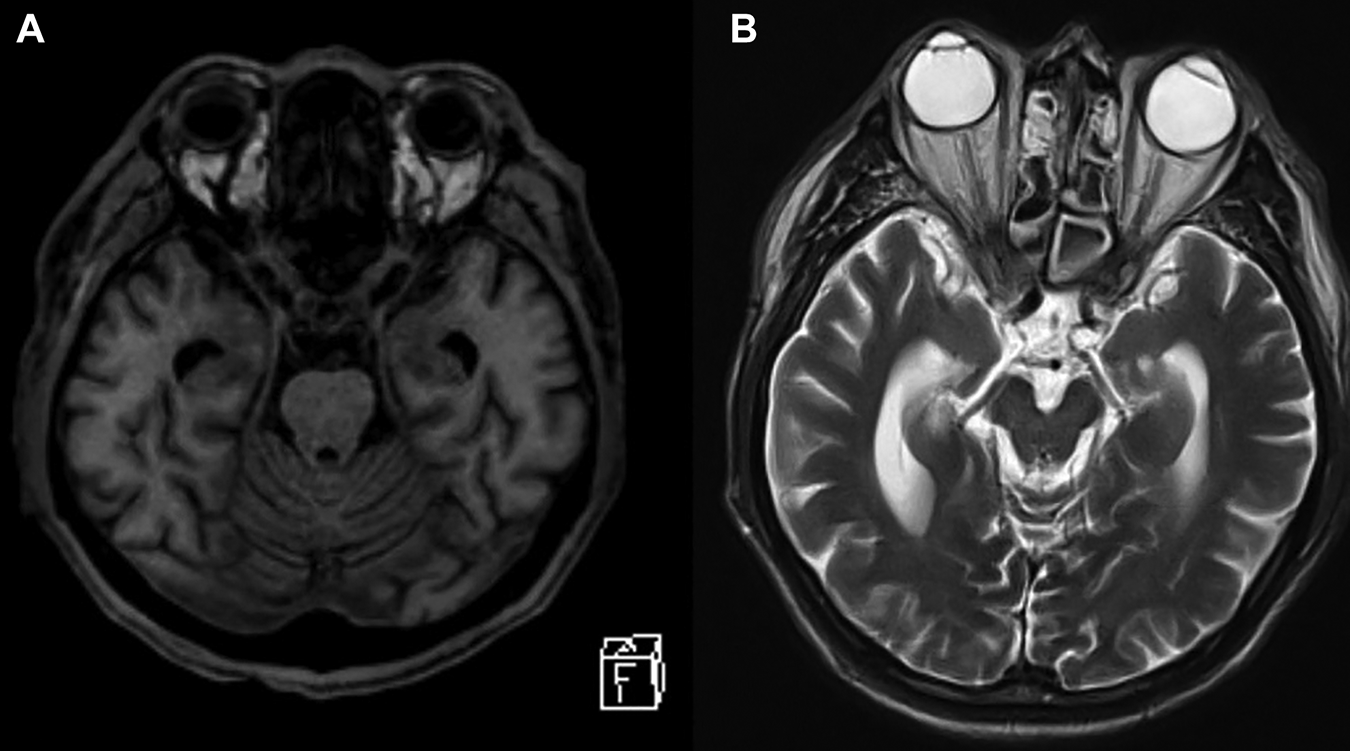
Initial MRI with axial T1 (A) and T2 (B) weighted sequences shortly after admission. There was no parenchymal, cavernous sinus or orbital apex abnormality, although moderate mucosal thickening in the paranasal sinuses can be visualized (B).
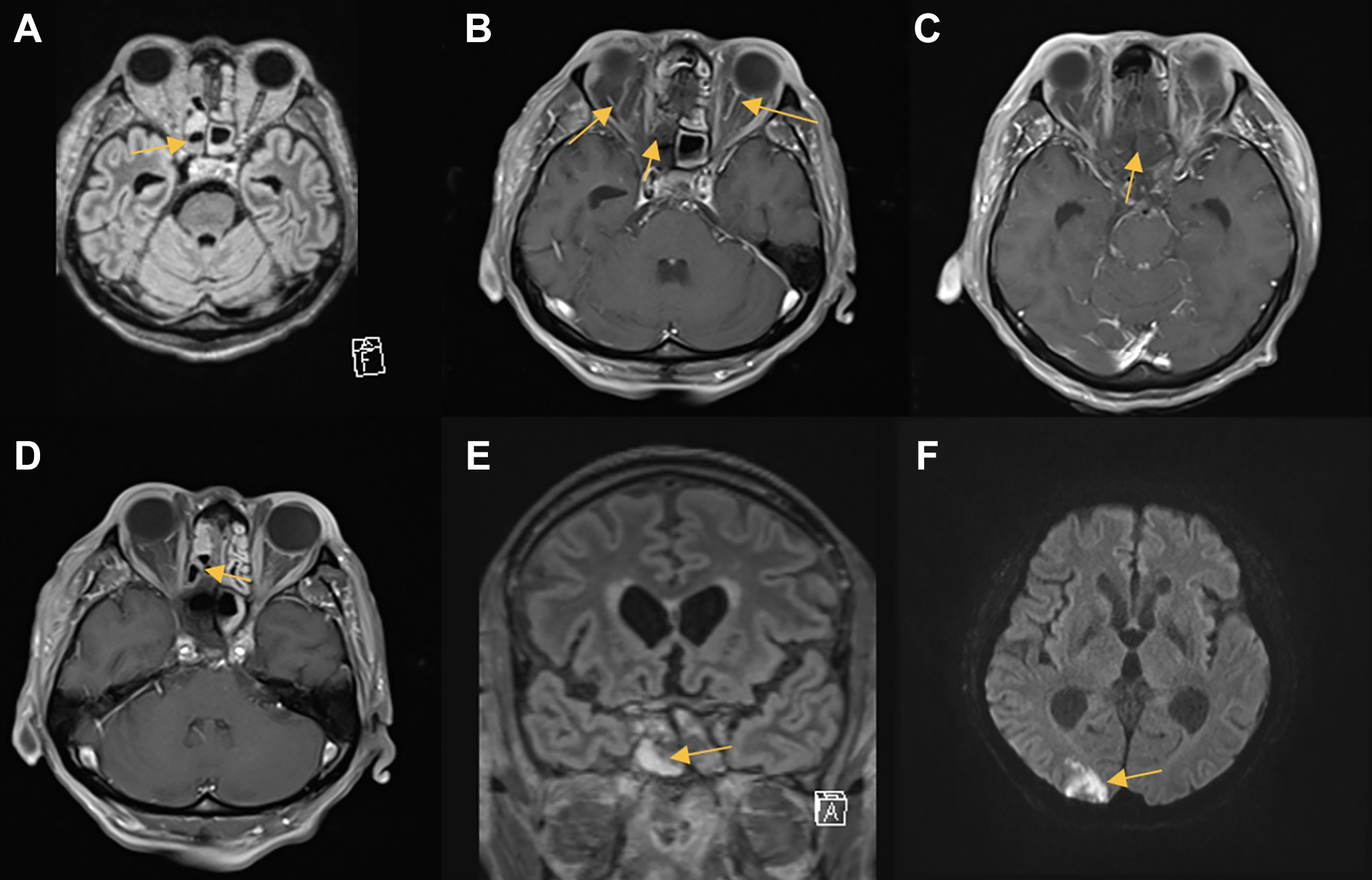
Second MRI with axial T2-FLAIR (A) and T1 post-contrast (B-C) sequences and third MRI post-debridement with axial T1 post-contrast (D), coronal T2-FLAIR (E), and axial DWI (F) sequences. The lack of enhancement in the moderately thickened mucosa of the right sphenoid sinus is suggestive of invasive fungal infection (B-D). The right optic nerve is edematous with diffusion restriction (E). An area of restricted diffusion in the right occipital lobe is consistent with infarct (F).
Over the next several days, he had progressive decreasing level of consciousness with increasing leukocytosis and elevated C-reactive protein (CRP) of 106 mg/L, although no clear infectious source was identified on cultures including spinal and peritoneal fluid. On repeat neurological examination he was obtunded with no eye opening to pain and not blinking to visual threat in the right eye. His right pupil was fixed at 5 mm, unreactive to light, and he had complete right ptosis and ophthalmoplegia.
Given these findings, the lesion was localized to the orbital apex and he was started on empiric antifungal treatment with amphotericin B for suspected mucormycosis. The differential diagnosis included vascular (cavernous sinus thrombosis, carotid artery aneurysm, carotid-cavernous fistula), inflammatory (sarcoidosis, Tolosa-Hunt syndrome, IgG4-related disease, vasculitis), trauma, metabolic (thyroid orbitopathy), infectious (bacterial, fungal, viral), and neoplastic (orbital and skull-based tumors) causes. Repeat MRI with gadolinium and dedicated orbital imaging (Figure 2A-D) revealed sphenoid sinus thickening, right optic nerve enhancement and edema and bilateral scattered infarcts with the largest in the right occipital lobe. There was lack of enhancement of the anterior right cavernous sinus and the thickened mucosa of the right sphenoid sinus concerning for invasive fungal sinusitis and cavernous sinus thrombosis.
Given his presentation of orbital apex syndrome and these imaging findings, he was taken urgently to the operating room for surgical debridement of the sinuses and endoscopic nasal septal reconstruction. Intraoperatively, there was minimal bleeding of the posterior ethmoid and right sphenoid sinuses suggestive of necrotic tissue and biopsies confirmed angioinvasive mucormycosis on frozen section, however the extent of necrosis was beyond resection. Repeat MRI (Figure 2C-F) showed persistent disease at the base of the skull and further bilateral focal cortical infarcts in an embolic and watershed distribution. His clinical status worsened considerably over the next few days at which point his family requested transition to comfort care. The patient died 11 days after admission to hospital.
Discussion
Mucormycosis is an infection by fungi belonging to the order Mucorale 1 and characteristically causes host tissue infarction and necrosis due to invasion of vasculature by fungal hyphae and their interaction with endothelial cells. 2 As a result of their direct involvement with invasion of the vasculature, multifocal strokes in various vascular territories can be a finding in patients with invasive fungal infection,1,2 as was the case with our patient. Mucormycoses cause severe, life threatening infections that primarily affect immunocompromised individuals such as those with solid organ transplants or diabetes, but can also affect immunocompetent patients. 2 Major risk factors include uncontrolled diabetes mellitus particularly with diabetic ketoacidosis, metabolic acidosis, iron overload or iron chelation therapy, as an acidic environment (pH 7.3-6.8) and increased iron availability are known to support the growth of the fungus. 2 Additional risk factors include immunosuppression due to corticosteroids or solid organ transplantation, neutropenia, trauma, burns, and malignant hematological disorders.2,3 Mucormycosis can present as rhino-orbital cerebral or pulmonary syndrome, the former which typically affects diabetics and the latter in patients with hematological malignancies. 4 With invasion of the paranasal sinus mucosa, the fungus can spread directly to the orbital apex and gain intracerebral access. 5
The orbital apex is an important localization in neurology and is characterized by vision loss from involvement of the optic nerve, ophthalmoplegia with involvement of the ocular motor nerves (namely CN III, IV, VI) and involvement of the first division of the trigeminal nerve (V1). 6 As a result of anatomical proximity, overlapping syndromes include the superior orbital fissure and cavernous sinus syndrome which may have similar findings but without optic nerve involvement.
When suspected, rhino-orbital cerebral mucormycosis is a medical emergency requiring treatment with antifungals and emergency surgical debridement in addition to correction of risk factors. 5 Clinical features include any patient with risk factors presenting with an acute deterioration in their respiratory status and features suggestive of orbital apex involvement. Imaging findings include soft tissue thickening of the paranasal sinuses and MRI may show T1 isointense lesions with low signal on T2. As in this case, an unremarkable MRI brain does not rule out invasive fungal infection. Specifically in our case, it is not surprising that the initial MRI scan was mostly unremarkable given that it was done without contrast and was not dedicated orbital imaging. MRI with gadolinium can reveal devitalized mucosa as contiguous foci of non-enhancing tissue which is known as the black turbinate sign. 7 Treatment should be started immediately, even if empirically, and is typically with amphotericin B (Amb) and posaconazole. 2 Unfortunately, even with early empiric treatment and surgical debridement, prognosis is poor with a mortality of around 25% to 60% with those with rhino-orbital cerebral syndrome and as high as 87% with those with pulmonary involvement.2,3
This case illustrates an orbital apex syndrome which is highly localizing, and combined with knowledge of the patient’s risk factors and pathophysiology, a diagnosis of mucormycocis was suspected even in the absence of initial imaging findings. It is good practice to self-review images, especially in cases where clinical localization and imaging are discordant, and to be aware of the limitations of initial diagnostic tests with follow-up studies where indicated. Although the black turbinate sign on MRI can be helpful in diagnosing invasive fungal rhinitis, in this case, dedicated orbital MRI with gadolinium was revealing and should be the preferred mode of imaging for highly suspected cases. A case series on imaging findings in mucormycosis revealed some degree of enhancement in 3 out of 5 cases demonstrating that dedicated orbital imaging with gadolinium is the preferred imaging modality. 7 A key take-home point is that even in the absence of imaging findings it is important to maintain a high degree of suspicion when patients present with clear localizing signs and risk factors, in this case orbital apex findings and risk factors for fungal infection.
Footnotes
Abbreviations
Authors’ Note
Dr. Marzoughi and Dr. Chen were both involved with concept, acquisition of data, and writing and revision of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.