
Abstract
Recent population-based studies have suggested that migraine is a risk factor for the development of infarct-like lesions in the territory of the posterior circulation. These lesions are thought to be true vascular infarcts based on their size, location and magnetic resonance imaging (MRI) characteristics. However, as there are no postmortem studies identifying the pathology of these MRI findings, their true aetiology is unknown. A case patient with migraine is presented, who developed what appeared to be cerebellar infarcts on MRI, but these lesions vanished on repeat imaging 16 days later, questioning their aetiology as vascular ischaemic based infarcts.
Introduction
Recent population-based studies have suggested that migraine is a risk factor for the development of infarct-like lesions in the territory of the posterior circulation (1). The most common site of these supposed infarcts is the cerebellum (2). These lesions are thought to be true vascular infarcts based on their size, location and magnetic resonance imaging (MRI) characteristics. However, as there are no postmortem studies identifying the pathology of these MRI findings, their true aetiology is unknown. If indeed they are infarctions, what does that mean for the long-term neurological health of the millions of individuals with migraine? If they are not vascular insults, then what are they? A case patient with migraine is presented, who developed what appeared to be cerebellar infarcts on MRI, but whose lesions vanished on repeat imaging 16 days later.
Case
A 45-year-old woman had a history of migraine without aura. Headaches had begun episodically in childhood with slow progression to chronic daily headache in the face of analgesic overuse with over-the counter pain relievers. She started to be seen at our centre 3 years previously, with improvement of headaches on migraine prevention with topiramate and after getting out of analgesic rebound. For the past 2 years her baseline headache frequency was three mild headaches per week and one severe headache per month. Neurological examination, including neurovascular examination (auscultation for carotid, orbital and cranial bruits), had been normal. She had a personal history of mild hypertension with a borderline elevation in cholesterol and a family history of hypertension in a brother, and diabetes in her father. Recently, the patient's headaches had become more frequent and she developed a complaint of episodic blurred vision, together with nondescript dizziness (not vertigo) that had been present for the last 5 years intermittently, but had become slightly more frequent. Neurological examination with these new symptoms was normal. Her blood pressure over the past 1 year was stable on a single antihypertensive agent. Ophthalmological evaluation for the blurred vision was normal. A brain MRI was ordered to rule out a secondary cause for her increased headache frequency and questionable neurological complaints. This demonstrated two adjacent lesions within the right cerebellar hemisphere that appeared bright on T2, fluid-attenuated inversion recovery (FLAIR) image and diffusion weighted imaging (DWI), suggestive of subacute ischaemic infarcts (Fig. 1a,b,d) She had had two previous brain MRIs, one 6 years and one 3 years previously, that had both shown two stable focal white matter areas of increased T2 signal in the right centrum semiovale of unknown significance, with nothing noted in the cerebellum. Sixteen days after the MRI demonstrating probable cerebellar infarcts, magnetic resonance angiography of the intracranial and extracranial carotid circulation was completed to look for any significant posterior circulation abnormalities. This examination was within normal limits. A repeat brain MRI without diffusion was also completed and showed resolution of the previously seen cerebellar infarcts on both T2 and FLAIR weighted imaging (Fig. 1c,e). The only medication change in between the two scans was the addition of a baby aspirin 81 mg. A 2D-echocardiogram with bubble contrast study was completed and this was normal, with no evidence of a patent foramen ovale or right-to-left shunt.
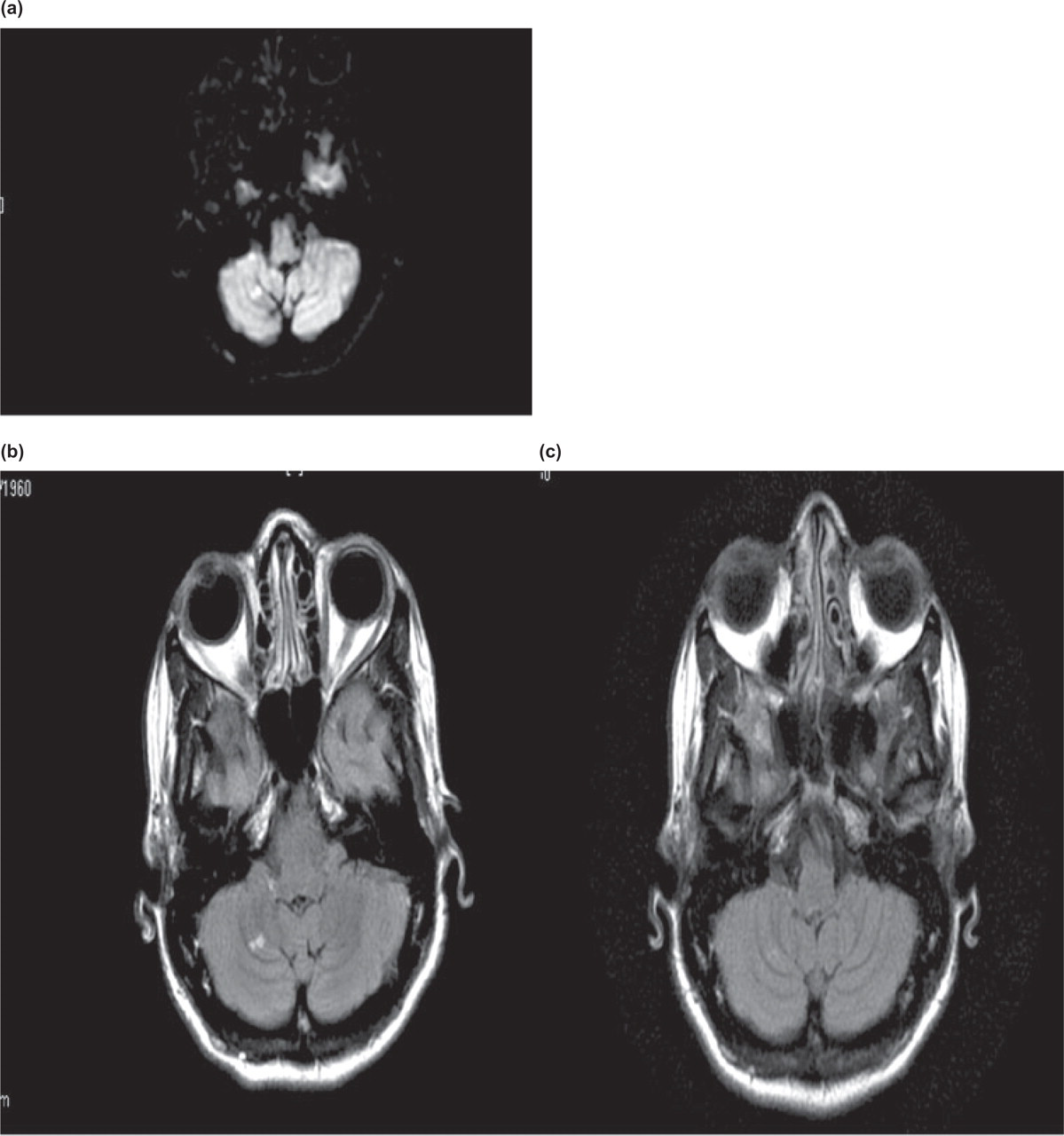
(a) Two adjacent lesions of bright signal on diffusion weighted images consistent with subacute infarcts. (Date of exam 18 Jan. 2006.) (b) Fluid-attenuated inversion recovery (FLAIR) image demonstrating two focal areas of bright signal intensity suggestive of focal infarcts. (Date of exam 18 Jan. 2006.) (c) Resolution of previously identified lesions on FLAIR imaging. (Date of exam 3 Feb. 2006.) (d) T2 weighted image demonstrating two focal areas of bright intensity suggestive of focal infarcts. (Date of exam 18 Jan. 2006.) (e) Resolution of previously identified lesions on T2 weighted image. (Date of exam 3 Feb. 2006.)
Discussion
Migraine appears to be a risk factor for the development of infarct-like lesions, especially involving the cerebellum (2). However, the true pathology of these infarct-like lesions is not known. In the CAMERA study, strict MRI imaging criteria were utilized to make a diagnosis of cerebral infarction (2). These same rigorous criteria, however, were not utilized to make a diagnosis of infarct for the presented case. The case patient appeared to have developed cerebellar infarcts based on the MRI characteristics of the lesions, but as the lesions vanished after 2 weeks, this questioned an ischaemic pathology. In some instances of true ischaemic stroke, MRI findings may be transient. DWI can detect early ischaemic changes. DWI lesions may reverse in some cases of stroke (3). In patients with transient ischaemic attacks, the majority of DWI lesions will not persist beyond 2 weeks from symptom onset (3). Thus, the reversal of DWI lesions on MRI cannot rule in or rule out true cerebral ischaemia. Interestingly, in animal models looking at brief episodes of focal ischaemia, there is histological evidence of ischaemic injury, even though there is early reversal of DWI lesions (4).
If the case patient's MRI findings were not from ischaemic infarcts, they could have been mitochondrial based stroke-like lesions, which are known to disappear on subsequent neuroimaging (5). Mitochondrial based strokes may reflect non-vascular mechanisms and thus behave differently from vascular strokes (6). It is known that migraineurs have changes on MR spectroscopy, both within and outside the central nervous system, suggesting mitochondrial dysfunction (7). The case patient did have stroke risk factors outside of migraine, but they were well controlled and no embolic source was identified on echocardiography.
The natural history of the infarct-like lesions of migraine has also not been established. We do not know if these lesions remain static or progress. The presented case suggests that these MRI lesions can reverse. In addition, the long-term neurological effects of these infarct-like lesions on migraineurs are unknown. Vanishing lesions may suggest an aetiology other than vascular ischaemia, so postmortem data are essential to define pathology.