
Abstract
Background
Although amputation rates, morbidity, and mortality have been established for select populations, the impact of general demographic factors on postoperative surgical complications remains little studied.
Methods
The American College of Surgeons’ National Surgical Quality Improvement Program database was searched for leg amputations from 2012 to 2017 using CPT codes 27881, 27882, 27884, and 27886, identifying 4162 patients. A total of 29 demographic variables with 4 complications (surgical infection, additional service, and deep-vein thrombosis [DVT], and sepsis) were analyzed.
Results
Preoperative open, contaminated, or dirty/infected wounds; longer intraoperative times; development of sepsis prior to surgery; and admission of patients from home or another hospital influenced postoperative infection rates. Preoperative open, infected, or dirty/infected wounds; height; weight; total length of hospital stay; and ethnicity affected postoperative additional service incidence. Preoperative congestive heart failure, large decreases in body weight, and total length of hospital stay influenced postoperative DVT rates. Preoperative functional heath status, total length of hospital stay, amputations conducted as emergency cases, preoperative acute renal failure, open or infected wounds, sepsis, and contaminated or dirty/infected wounds affected postoperative sepsis rates.
Background
Conclusion. Understanding these risk factors may allow providers to anticipate and address higher rates of complications in certain patient populations.
Level of evidence:
Level III: Prognostic
“Similarly, the incidence of major amputation in patients with peripheral artery disease is elevated relative to the general population, ranging from 500 to 1000 amputations per 100 000 person-years.”
Introduction
Previous research suggests that certain demographic groups undergo leg amputation more frequently than the general population.1-6 Individuals with diabetes mellitus, for example, have a 10- to 12-fold increased risk of lower extremity amputation when compared with individuals without diabetes. 1 Similarly, the incidence of major amputation in patients with peripheral artery disease is elevated relative to the general population, ranging from 500 to 1000 amputations per 100 000 person-years. 7 Despite advances in the management of those with lower extremity complications, below-the-knee amputation (BKA) rates have remained between 9 and 12.5 per 100 000 person-years since 1990.1,8 Whereas amputation rates and amputation-related morbidity and mortality have been established for select populations, the impact of general demographic factors on a patient’s postoperative surgical complication incidence remains little studied. Therefore, this study aims to analyze the influence of numerous demographic variables on specific surgical complications.
Methods
We extracted data from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database from January 2012 to December 2017 and searched for leg amputations using CPT codes 27881, 27882, 27884, and 27886, whereby 4162 patients were identified. We selected 29 demographic variables and analyzed their association with each of 4 complications (surgical infection, additional service, deep-vein thrombosis [DVT], and sepsis) using t tests or χ2 tests. For each complication, we then conducted a logistic regression to determine independent risk factors for that outcome, based on results from the bivariate analyses. Specifically, variables found to have P <.2 on bivariate analysis were subsequently included in the multivariate analysis of the corresponding surgical complication.
Results
Supplementary Table 1 lists patient demographics of identified amputees. These patients had an average age of 59.76 ± 12.89 years; 68.57% were Caucasian (n = 2629), 29.08% were African American (n = 1115), 1.17% were Asian (n = 45), 0.63% were American Indian or Alaskan Native (n = 24), and 0.55% were Native Hawaiian or Pacific Islander (n = 21). Additionally, males comprised 69.7% of the population (n = 2816).
During the 30-day postoperative period, 8.15%, 18.27%, 0.99%, and 13.24% of those undergoing leg amputation returned with a surgical infection, additional service, DVT requiring therapy, and sepsis, respectively (Supplementary Table 2). To be categorized as a postoperative surgical infection, conditions had to involve the skin and subcutaneous tissue at the incision site of the principal operative procedure. From these criteria, it was found that 339 patients (8.15%) developed a postoperative surgical infection within the 30-day period following leg amputation. In particular, multivariate analysis indicated that when compared with patients without these comorbidities, patients who had a preoperative open wound or wound infection were 1.3851 times more likely to return with a postoperative surgical infection (P = .02). Likewise, when compared with individuals whose wound was classified as clean preoperatively, those with wounds classified as contaminated, or dirty/infected preoperatively (odds ratio [OR] = 1.533, P = .02, and OR = 1.5298, P = .002, respectively) were more likely to return with a postoperative surgical infection. Additionally, patients who returned with a postoperative surgical infection had a mean operation time of 59.84 ± 56.47 minutes, whereas those without surgical infections during the postoperative period had a mean operation time of 54.3 ± 43.3 minutes. From the multivariate analysis, it was found that for each additional minute spent in surgery, the likelihood of developing a surgical infection increased by a factor of 1.0024 (P = .02). Conversely, patients who had sepsis within 48 hours before surgery were 0.70698 times less likely to present with a postoperative infection than those who did not experience sepsis prior to surgery (P = .01). Furthermore, patients who were admitted directly from home or from another hospital’s emergency room were 0.71363 times less likely to return with a postoperative surgical infection than those who were transferred from an inpatient facility or nursing home (P = .04). Table 1 describes the relationships of variables included in the multivariate regression with surgical infection rates following leg amputation.
Relationships of Variables Included in Multivariate Regression With Surgical Infection Rate a .
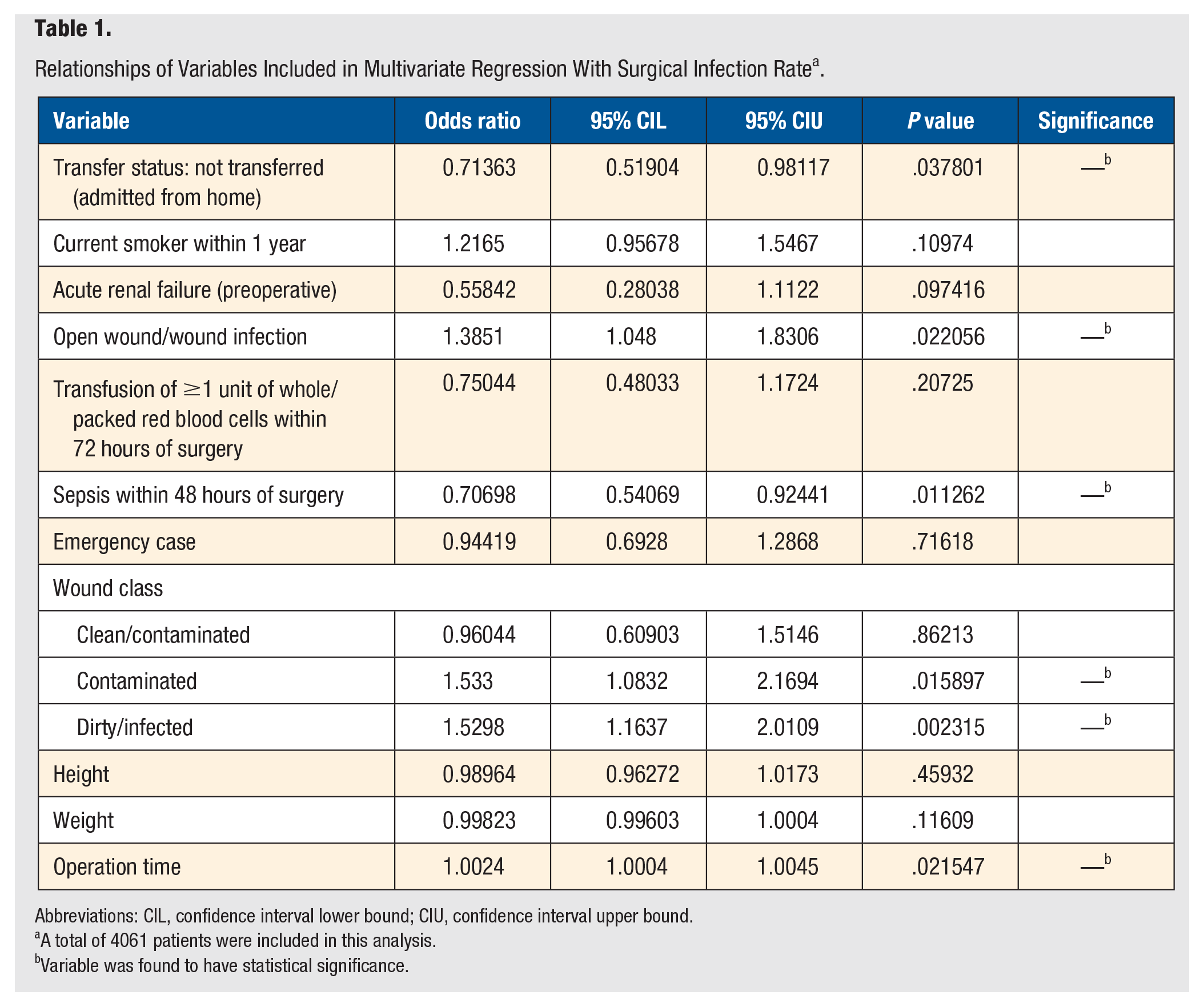
Abbreviations: CIL, confidence interval lower bound; CIU, confidence interval upper bound.
A total of 4061 patients were included in this analysis.
Variable was found to have statistical significance.
Within the 30-day period following amputation, 760 patients (18.27%) returned for an additional service related to the principal procedure. From the multivariate analysis, we determined that, when compared with individuals whose wound was classified as clean preoperatively, patients whose wound was classified as dirty/infected were 1.2936 times more likely to return for an additional service postoperatively (P = .01). Additionally, individuals with open wounds or wound infections preoperatively were found to be 1.2533 times more likely to require an additional service postoperatively than those without these risk factors (P = .04). Furthermore, patients who required an additional service postoperatively had a mean total length of hospital stay of 13.8 ± 11.77 days, compared with 11.65 ± 11.08 days for those not requiring an additional service. It was found that for each additional day spent in the hospital, the likelihood of returning for an additional service increased by a factor of 1.0101 (P = .01). In contrast, it was established that Hispanics were 0.7543 times less likely than non-Hispanics to return for an additional service (P = .05). Additionally, we determined that patients presenting for an additional service had an average height of 67.5 ± 4.21 inches, whereas those without this complication had an average height of 68.14 ± 4.53 inches. From the multivariate analysis, it was found that every additional inch of height decreased a patient’s likelihood of presenting for an additional service by a factor of 0.97244 (P =.03). Finally, patients who returned for an additional service had an average weight of 191.41 ± 59.05 pounds, whereas those without this complication had an average weight of 198.74 ± 60.83 pounds. The multivariate analysis showed that every additional pound of body weight reduced a patient’s likelihood of returning for an additional service by a factor of 0.99775 (P = .008). The relationships of variables included in the multivariate regression with the additional service incidence can be found in Table 2.
Relationships of Variables Included in Multivariate Regression With Additional Service Rate a .
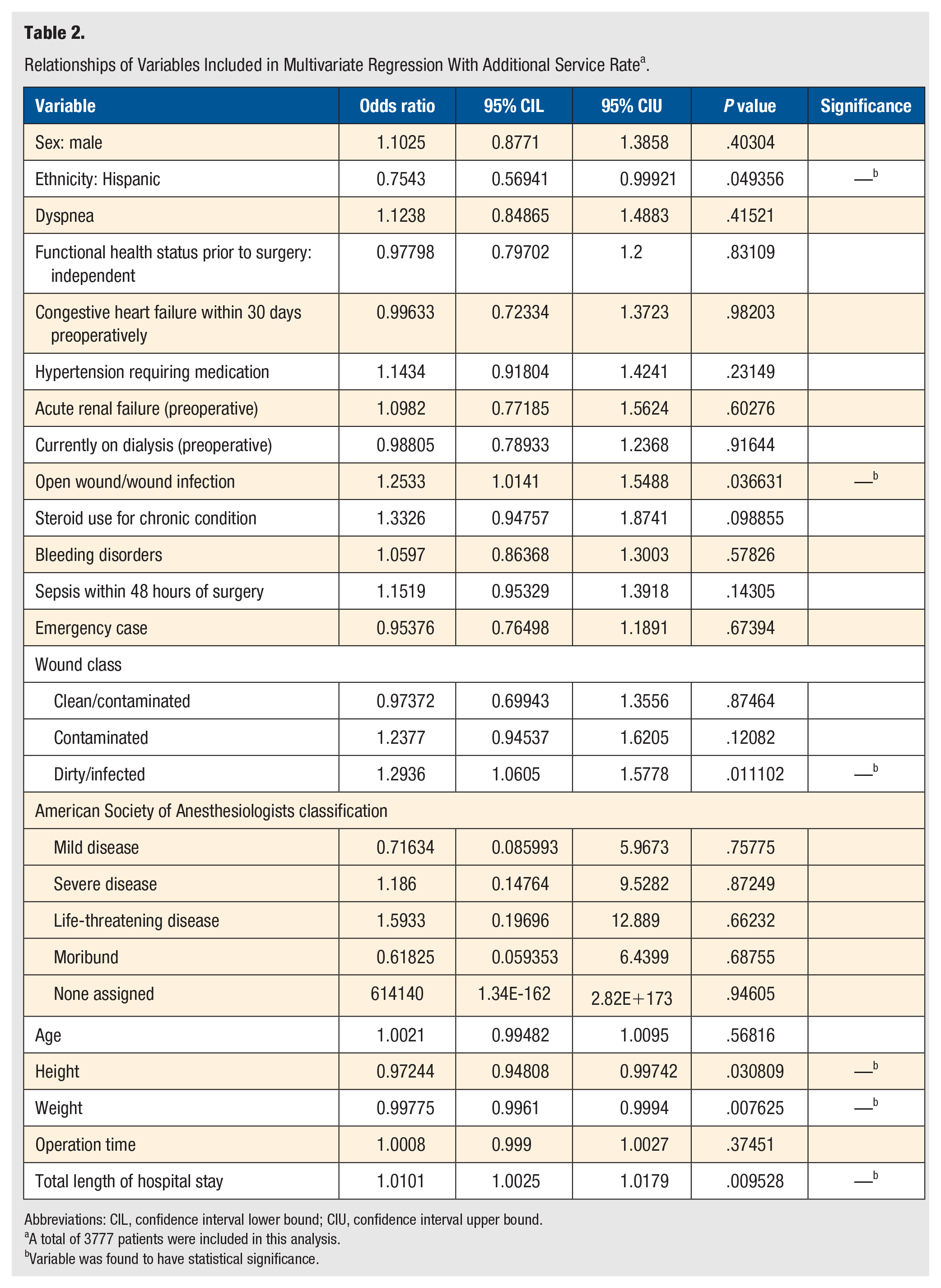
Abbreviations: CIL, confidence interval lower bound; CIU, confidence interval upper bound.
A total of 3777 patients were included in this analysis.
Variable was found to have statistical significance.
Individuals presenting with new-onset blood clots, or thrombi, that were confirmed by imaging and treated with anticoagulation therapy and/or placement of an inferior vena cava filter were classified as having a DVT, per NSQIP’s definitions. Of the 4162 patients undergoing leg amputation, 41 (0.99%) presented within the 30-day postoperative period with a new-onset DVT. It was found that patients who lost >10% of their total body weight in the 6 months prior to surgery (OR = 3.048; P = .03) or who had newly diagnosed congestive heart failure (CHF) or chronic CHF with new symptoms in the 30 days prior to surgery (OR = 2.3805; P = .04) were more likely to return with a new-onset DVT, when compared with those who did not have these risk factors. Additionally, patients who returned with a new-onset DVT postoperatively had a mean total length of hospital stay of 19.46 ± 14.19 days, whereas those not returning with a new-onset DVT had a mean total length of hospital stay of 11.96 ± 11.18 days. From the multivariate analysis, it was found that for each additional day spent in the hospital, the likelihood of returning with a new-onset DVT requiring therapy increased by a factor of 1.0258 (P = .001). The relationships of variables included in the multivariate regression with DVT incidence may be viewed in Table 3.
Relationships of Variables Included in Multivariate Regression with New-Onset Deep-Vein Thrombosis Rate a .
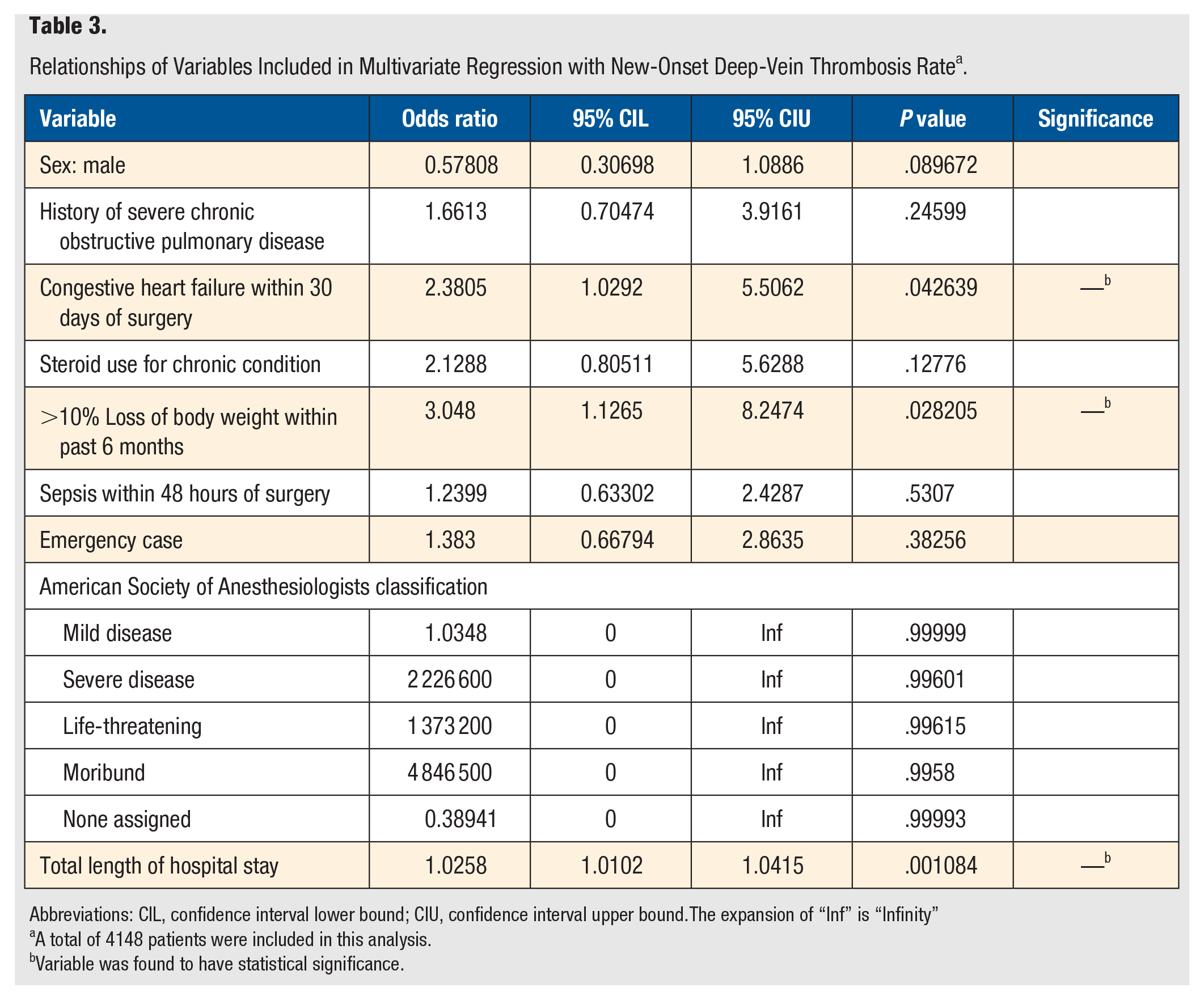
Abbreviations: CIL, confidence interval lower bound; CIU, confidence interval upper bound.The expansion of “Inf” is “Infinity”
A total of 4148 patients were included in this analysis.
Variable was found to have statistical significance.
Of the 4162 leg amputation patients, 551 (13.24%) presented within the 30-day postoperative period with sepsis. Patients who had acute renal failure preoperatively (OR = 1.6813; P = .004), who had an open wound or wound infection (OR = 1.4507; P = .01), who developed sepsis within 48 hours of surgery (OR = 3.8319; P < .001), and whose leg amputation was classified as an emergency case (OR = 1.7524; P < .001) were more likely to return with sepsis than those without these risk factors. Additionally, when compared with individuals with wounds classified as clean preoperatively, patients whose wound was classified as contaminated were 1.6033 times more likely to return with postoperative sepsis (P = .02), whereas those with wounds classified as dirty/infected were 2.5449 times more likely to return with postoperative sepsis (P < .001). Moreover, patients who developed sepsis postoperatively had a mean total length of hospital stay of 17.7 ± 13.69 days, whereas those without sepsis complications had a mean length of hospital stay of 11.17 ± 10.55 days. From the multivariate analysis, it was found that for each additional day spent in the hospital, the likelihood of returning with sepsis during the 30-day postoperative period increased by a factor of 1.0332 (P < .001). Finally, those whose functional health status prior to surgery was classified as independent, meaning that they did not require assistance from others for activities of daily living, were 0.73768 times less likely to return with sepsis than individuals who were either completely or partially dependent (P = .02). The relationships of variables included in the multivariate regression with sepsis incidence may be found in Table 4.
Relationships of Variables Included in Multivariate Regression With Sepsis Rate a .
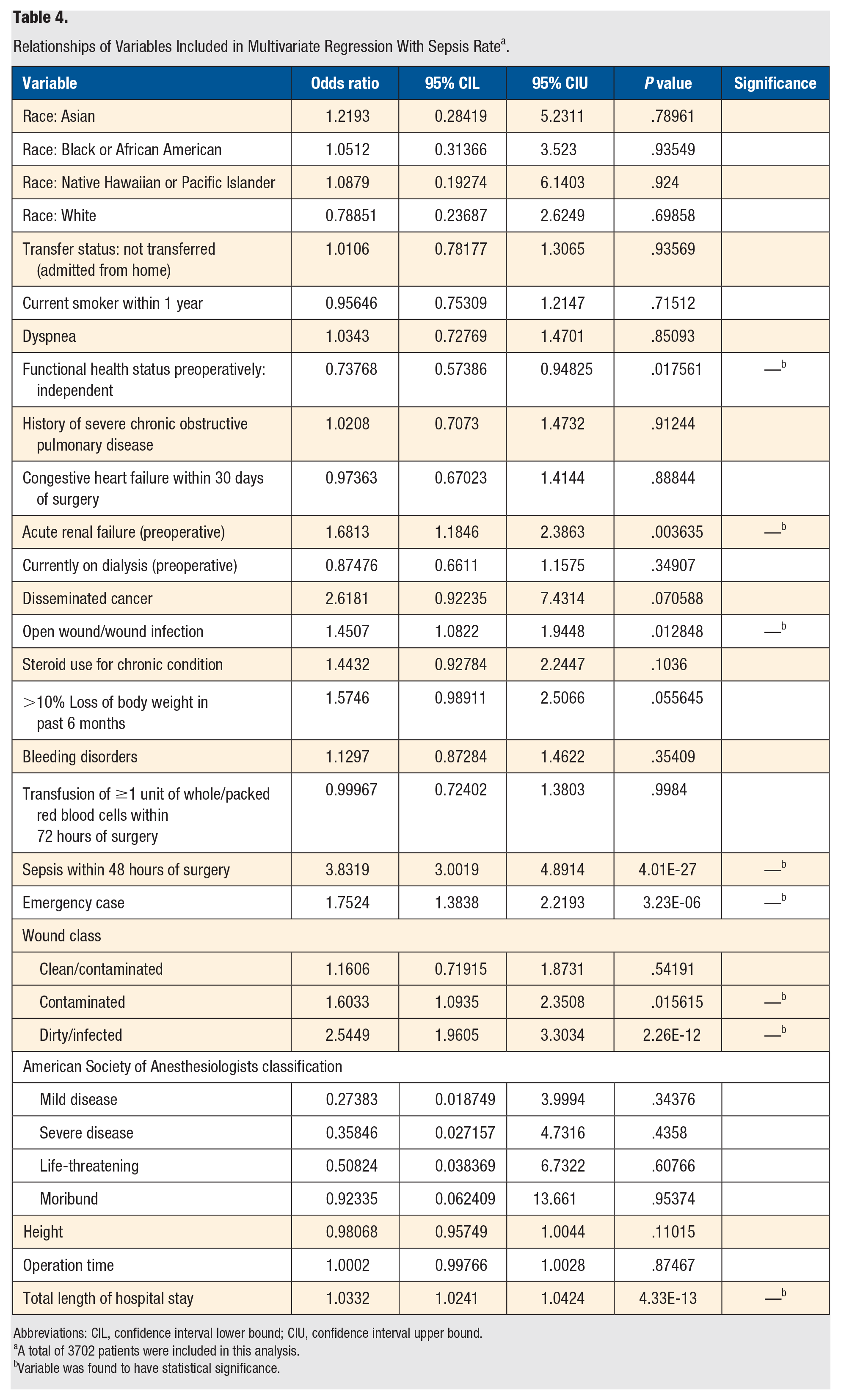
Abbreviations: CIL, confidence interval lower bound; CIU, confidence interval upper bound.
A total of 3702 patients were included in this analysis.
Variable was found to have statistical significance.
Discussion
Literature has established steroid use, renal insufficiency, smoking, and infected wounds as risk factors for complications following leg amputation. 1 However, whereas previous studies regarding leg amputation complications have focused on specific risk factors,1,2 our study sought to analyze a broader range of demographic variables that may predispose to 4 specific complications within the 30-day postoperative period.
A 2011 NSQIP study found that preoperative sepsis was the most important risk factor for developing 1 or more complications in the 30-day period following BKA. 1 Although results from our study indicated that patients developing sepsis within 48 hours of surgery were 3.8319 times more likely to develop sepsis postoperatively, our analysis also showed that these individuals were 0.70698 times less likely to develop surgical site infection complications within the 30-day postoperative period. This result is interesting and may be attributable to expedient treatment of the underlying preoperative infection, with residual sepsis symptoms during the postoperative period.
Wound status and the presence of preoperative open wounds or wound infections were found to factor into the risk of developing postoperative complications. Prior to leg amputation, the primary surgeon classified the wound site as clean, clean/contaminated, contaminated, or dirty/infected. The phrase contaminated suggested that the wound was open, fresh, and accidental. This classification also included operations with major breaks in sterile technique or incisions in which acute, nonpurulent inflammation was encountered. It was noted that when compared with individuals with clean wounds preoperatively, the presence of a preoperative contaminated wound increased the likelihood of presenting during the 30-day postoperative period for a surgical infection or sepsis by 1.533 and 1.6033, respectively. Additional service or new-onset DVT incidence did not appear to be affected by the presence of a contaminated wound. Similarly, the phrase dirty/infected suggested that the cause of the infection was present in the operative field before the amputation began. We found that those with wound sites classified as dirty/infected were at 1.5298 times higher risk of developing a surgical infection, 1.2936 times more likely to need an additional service, and 2.5449 times more likely to develop sepsis within 30 days of amputation when compared with individuals with wounds classified as clean. The incidence of new-onset DVT did not appear to be affected by the preoperative presence of a dirty/infected wound. Furthermore, it was noted that patients with preoperative open wounds or wound infections were at increased risk of developing complications following leg amputation. Specifically, when compared with those without these risk factors, these individuals were 1.3851 and 1.2533 times more likely to develop surgical infections or require additional services during the postoperative period, respectively.
Emergency cases, notable weight loss in the 6 months prior to surgery, and increased operation times and lengths of hospital stay were associated with a higher incidence of complications in the 30-day period following leg amputation. Cases in which leg amputation was performed shortly after symptom onset were classified as emergency cases. Our multivariate analysis established that, when compared with the rest of the population, those undergoing leg amputation as an emergency case were 1.7524 times more likely to return with postoperative sepsis. Additionally, patients who lost >10% of their body weight in the 6 months prior to surgery were found to be 3.048 times more likely to present with postoperative DVT without significant changes in surgical infection, additional service, and sepsis incidence. Moreover, we found that every extra minute of operative time increased the risk of presenting during the 30-day postoperative period with a surgical infection by a factor of 1.0024. Finally, it was noted that prolonging the hospital stay increased the likelihood of presenting during this period for an additional service, new-onset DVT, or sepsis by 1.0101, 1.0258, and 1.0332 per extra day, respectively. These findings correlate with those reported in the literature, which stress the importance of timely hospital discharge and limited operation durations to reduce complications.9,10
Ethnicity, weight, and height had varying effects on the postoperative complication incidence. Our multivariate analysis showed that patients who identified as Hispanic were 0.7543 times less likely than non-Hispanics to return for an additional service postoperatively, although there were no significant differences in surgical infection, new-onset DVT, or sepsis rates between the 2 groups. Additionally, patients with increased height or weight were less likely to present during the 30-day postoperative period for an additional service, displaying a 0.97244 times lower likelihood for each additional inch of height and a 0.99775 times lower likelihood for each additional pound of weight. We found that neither a patient’s height nor weight had a significant impact on the surgical infection, new-onset DVT, or sepsis incidence.
Patients with CHF or renal insult were identified as groups with increased rates of leg amputation complications. Our multivariate analysis revealed that patients with preoperative acute renal failure were 1.6813 times more likely to return with postoperative sepsis. Additionally, patients with a CHF exacerbation within 30 days of surgery were 2.3805 times more likely to present with a new-onset DVT following leg amputation. It was noted that preoperative CHF exacerbations did not predispose to postoperative sepsis or additional service complications. From these results, we conclude that the reduction in cardiac function and chronic inflammatory states associated with CHF, paired with immobilization of the patient following amputation, may increase a patient’s likelihood of pathological thrombogenesis.11,12 Therefore, patients with CHF would likely benefit from postoperative thromboprophylaxis to reduce the risk of DVT development.
Finally, an individual’s preoperative functional and transfer status were found to affect postoperative complication rates. Patients were categorized as functionally independent if they did not require assistance for activities of daily living. Our multivariate analysis showed that this group was 0.73768 times less likely to return with postoperative sepsis than patients who were dependent to some extent. Additionally, patients who were admitted to the hospital from home or another hospital’s emergency department were 0.71363 times less likely to return with a surgical infection than patients who were admitted from an inpatient facility or nursing home. This finding agrees with that from established literature, which suggests that interhospital transfer may decrease the quality of care a patient receives.13,14
The current study has several limitations. First, there were missing values for surgical infection (n = 101), additional service (n = 385), DVT (n = 14), and sepsis (n = 460) because of imperfections in data collection within the chosen database. Missing values may have skewed the results of our analysis, potentially decreasing the validity of this study’s conclusions, though these numbers are relatively small. Additionally, we selected 4 complications from the NSQIP database that were of interest, but various other complications can also occur. Expanding the scope of this study to include other complications may provide further insight into how certain demographic factors predispose to leg amputation complications. Moreover, our study did not analyze above-the-knee amputations and BKAs independently, which may reduce the generalizability of the study because of differences in the procedures’ risk factors and complication rates. Finally, the NSQIP database provides no information on complications that may occur after the 30-day postoperative period. Therefore, the findings of this analysis may not apply to more long-term patient care.
Conclusions
Despite advances in patient care, rates of leg amputation have remained relatively constant since 1990. As such, this study sought to identify independent risk factors for specific complications during the 30-day postoperative period. Understanding these risk factors may allow providers to anticipate and address higher rates of complications in certain patient populations.
Supplemental Material
sj-docx-1-fas-10.1177_19386400211001980 – Supplemental material for Predisposing Factors for 30-Day Complications Following Leg Amputation
Supplemental material, sj-docx-1-fas-10.1177_19386400211001980 for Predisposing Factors for 30-Day Complications Following Leg Amputation by Joseph V. Villarreal, Doha G. Hussien, Vinod K. Panchbhavi and Daniel C. Jupiter in Foot & Ankle Specialist
Supplemental Material
sj-docx-2-fas-10.1177_19386400211001980 – Supplemental material for Predisposing Factors for 30-Day Complications Following Leg Amputation
Supplemental material, sj-docx-2-fas-10.1177_19386400211001980 for Predisposing Factors for 30-Day Complications Following Leg Amputation by Joseph V. Villarreal, Doha G. Hussien, Vinod K. Panchbhavi and Daniel C. Jupiter in Foot & Ankle Specialist
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vinod K. Panchbhavi is a consultant for Stryker Orthopaedics as well as an editor for Lippincott Williams and Wilkins Publishing. The other authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.