
Abstract
Background:
Major lower limb amputation is occasionally required in the management of end-stage pathology where other treatment options have failed. The primary aim of this study was to determine the 30-day and 1-year mortality rates of patients undergoing nontraumatic major lower limb amputation. Secondary aims were to investigate risk factors for poor outcomes, incidence of previous minor amputation, and the rate of subsequent major amputation.
Methods:
All nontraumatic, major lower limb amputations performed at Toowoomba Hospital during an 18-year period were retrospectively reviewed. Mortality data were obtained from the Queensland Registry of Births, Deaths and Marriages. Kaplan–Meier analysis was performed to determine survival after amputation.
Results:
A total of 147 patients were included in the study, with 104 undergoing below knee and 43 undergoing above knee amputations. Ten patients identified as having an Aboriginal and Torres Strait Islander background. For all patients, the 30-day mortality was 4.1% and 1-year mortality was 21.1%. For Indigenous patients, 30-day mortality was 10%. Previous minor amputation had occurred in 40 patients. Twenty-nine patients underwent further minor surgery after their initial major amputation, with thirteen requiring subsequent major amputation. Factors that increased mortality risk were the presence of peripheral vascular disease, an American Society of Anesthesiologists score of four and age greater than 65 years.
Conclusion:
The morbidity and mortality following major lower limb amputation is significant. The findings of this study highlight the importance of preventative measures to minimize the incidence of lower limb amputations in the future.
Introduction
Hippocrates is credited with the aphorism, “for extreme diseases, extreme methods of cure…are most suitable.” Major amputation would certainly be viewed by many as an extreme method of cure. However, such surgery is occasionally necessitated for end-stage diabetic foot wounds and end-stage peripheral vascular disease (PVD), where attempts at limb salvage have failed. Morbidity and mortality rates following major lower limb amputations are significant. 1,2 There is a considerable psychosocial and economic burden of disease for the patient, family, and society. 3,4 Amputation rates are increasingly being used by health-care services as metrics of population demographics and quality of service delivery. 5,6
There are marked global differences in the incidence of major lower limb amputations. 6,7 In England alone, the incidence ranges from 5.1 to 176 per 100,000. 6,8 In Australia, 4402 lower limb amputations were performed between 2012 and 2013, at a rate of 23 per 100,000 population. 9
One of the main contributors to the amputation rate in Australia is the increasing incidence of type 2 diabetes mellitus. Approximately 1.2 million Australians live with diabetes, and this number is estimated to increase to 3.5 million by 2033. 10 –12 There is an increased prevalence of diabetes in men and women by geographical remoteness and almost double the rate in lower socioeconomic groups. 10,11 Despite advances in medical management, peripheral neuropathy and subsequent diabetic foot wounds are known complications of long-standing diabetes. End-stage diabetic foot wounds that fail salvage attempts often necessitate amputation.
Following a local increase in incidence, we undertook a retrospective review of all major, nontraumatic, lower limb amputations performed at Toowoomba Hospital since 2000. Our primary aims were to determine 30-day and 1-year mortality rates. Our secondary aims were to investigate demographic indicators, major comorbidities, risk factors, incidence of previous minor amputation, and the rate of subsequent major amputation.
Material and methods
Toowoomba Hospital is a Level Five regional health service, providing care to and receiving referrals from the Darling Downs region. The region covers a total area of 166,400 square kilometers and has a regional and remote population of about 128,800 people. 13 The Darling Downs Hospital and Health Service Human Research Ethics Committee approved this study.
A retrospective review of all major lower limb amputations performed at Toowoomba Hospital from January 1, 2000, to December 31, 2017, was conducted utilizing our operating theatre database (ORMIS v10.2). This database prospectively collects patient demographics, indication for surgery, and perioperative data. Patients were excluded from the study if they were younger than 18 years, if they had undergone a major amputation for trauma, or if their medical records were incomplete. Patients with primary bone and soft tissue malignancies are routinely referred to a tertiary center, so no amputations were performed for oncological reasons. A total of six patients were excluded (Figure 1). All major lower limb amputations performed were identified with International Classification of Diseases (ICD-10-AM) codes. Both electronic and paper medical records were reviewed by the primary author (VV). Major amputations were classified into below knee amputation (BKA) and above knee amputation (AKA) groups.

Flowchart of patient inclusion.
Patient demographic data, comorbidities, previous minor ipsilateral amputations, and subsequent major ipsilateral and contralateral amputations were recorded. Specifically, diabetes (type 1 or 2) and PVD were sought as key risk factors. 4,14 –16 Postoperative complicates were identified. Any prior amputation that involved the toe or part of the foot was recorded as a minor amputation. The initial major amputation was regarded as the primary amputation. Patient mortality was identified via an external audit conducted by the Queensland Registry of Births, Deaths and Marriages.
Data were entered into a spreadsheet (Microsoft Excel) and later transferred to SPSS (SPSS software®, 15.0; IBM Inc., Chicago, IL, USA) Version 26.0 for Microsoft for further analysis. Initially, continuous variables were assessed using Kolmogorov–Smirnov (K-S) test, histograms, and normal quantile–quantile plots. This demonstrated that age was normally distributed (K-S test, p = 0.11) and duration of surgery was not normally distributed (K-S test, p = 0.076). As a result, mean age was compared with independent t-test (2-tailed) and duration of surgery with Mann–Whitney U test. Nominal variables were analyzed with Fisher’s exact test (2-sided). Kaplan–Meier analysis was used to determine freedom from repeat major amputation and death.
Cox-proportional analysis was used to assess the effects of known risk factors on all-cause mortality. Categorical variables were dummy coded. Known risk factors, including age, ASA score, smoking status, diabetes mellitus, hypertension, dyslipidemia, ischemic heart disease, and peripheral vascular disease were examined for inclusion in the final model. Association of risk factors with all-cause mortality was examined using a stepwise selection procedure (backward and forward likelihood ratios). Variables not in the final stable model included smoking status, diabetes mellitus, hypertension, dyslipidemia, and ischemic heart disease.
Results
We identified 147 patients who underwent major amputation and met the inclusion criteria. Baseline characteristics are listed in Table 1. Mean patient age was 69 years (standard deviation (SD): 14 years; range: 32–95 years) and 67% were male. There were 10 patients (7%) who identified as having an Aboriginal and Torres Strait Islander background. Seventy patients (48%) were smokers. Many patients were considered ASA-3 or ASA-4 (n = 130). The index operation was a BKA in 104 patients (71%) and AKA in 43 patients (29%). The indications for amputation were infection (51.7%), PVD (22.4%), ischemic limb or gangrene (20.4%), failed fixation (3.4%), pantalar arthritis (1.4%), and chronic pain (0.7%). Prior minor amputation had occurred in 40 (27%) of patients. Mean operative time was 169 min (range: 84–264 min).
Baseline characteristics of cohort divided by amputation type.

BKA: below knee amputation; AKA: above knee amputation; ASA: American Society of Anesthesiologists; NA: not applicable; SD: standard deviation; IQR: interquartile range.
a Statistical analysis was independent t-test for continuous data.
b Statistical analysis was Fisher’s exact test for categorical variables.
c Statistical analysis was Mann–Whitney U test for continuous data.
d Statistical analysis was Pearson’s χ 2 for categorical variables.
There were 82 patients who died during the follow-up period. Cause of death included unspecified 53.7% (n = 44), myocardial infarctions 24.3% (n = 20), renal failure 7.3% (n = 6), sepsis 7.3% (n = 6), respiratory failure 3.7% (n = 3), and cerebrovascular accidents 3.7% (n = 3). Mortality rates for all patients at 30 days and 1 year were 4.1% (n = 6) and 21.1% (n = 31), respectively. Long-term projected analysis predicted mortality at 5 years and 15 years were 47% and 68%, respectively. For patients identified as Indigenous, mortality rate at 30 days was 10%.
There were 29 patients (20%) who underwent repeat surgery. Overall, repeat major amputation was performed in 8.8% (n = 13) (ipsilateral AKA 4, contralateral BKA 6, and contralateral AKA 3) for ongoing infection, wound dehiscence, and progressive PVD. Subsequent minor surgery included stump washout (10.2%), hamstring release (0.7%), and contralateral toe amputation (0.7%). No baseline characteristics were associated with repeat surgery; however, 30% of the Indigenous population had repeat operations.
Patients undergoing BKA were more likely male (72% vs 54%, p = 0.03), younger (mean 67 vs 73 years old, p = 0.03), diabetic (77% vs 51%, p = 0.003), and related to infective etiology (mean 55% vs 30%, p = 0.001). Operative time was longer for BKA compared to AKA (mean 173 min vs 155 min, p = 0.045). Mortality rates were similar between groups (Figure 2). The 30-day and 1-year mortality rate for the AKA and BKA cohort was 9.3% (n = 4) versus 1.9% (n = 2) (p = 0.061) and 25.6% (n = 11) versus 20.2% (n = 20) (p = 0.303), respectively.

Kaplan–Meier graph displaying all-cause mortality for AKA versus BKA. AKA: above knee amputation; BKA: below knee amputation.
The amputees’ major comorbidities were hypertension, ischemic heart disease, and diabetes mellitus, as seen in Table 1. Using cox proportional regression, we examined the association between risk factors and all-cause mortality. Patients with PVD, higher ASA score, and age greater than 65 years had increased risk of all-cause mortality (Table 2).
Cox proportional analysis examining prognostic factors for all-cause mortality.a
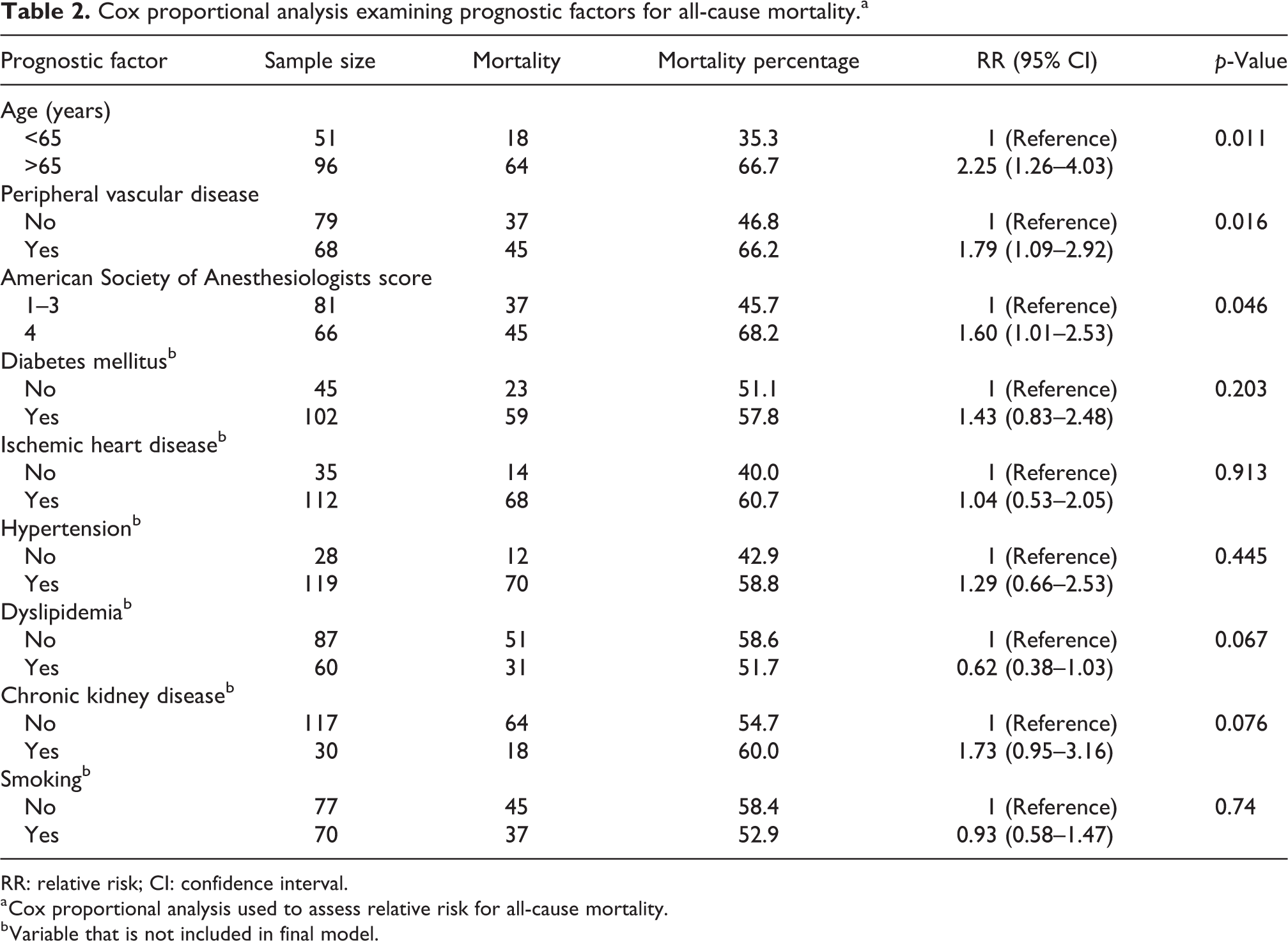
RR: relative risk; CI: confidence interval.
a Cox proportional analysis used to assess relative risk for all-cause mortality.
b Variable that is not included in final model.
Discussion
Major lower limb amputation is an “extreme method of cure” for end-stage pathology, where medical and surgical attempts at limb salvage have failed. Previous studies have shown that diabetic foot wounds and PVD are common indications for such surgery. 3 Our study supports this finding. Despite local and national attempts to improve the management of chronic disease, in particular type 2 diabetes, we have noticed an increased incidence in major, nontraumatic amputations at our facility. This trend is probably multifactorial. Our catchment area is large, with variable access to primary health-care facilities. Our region has a relatively low socioeconomic status, low levels of health literacy, high levels of obesity, and high levels of chronic disease. Late presentation with advanced disease is common.
Our study appears to be the first of its kind in regional Queensland. We identified a 30-day mortality of 4.1% and a 1-year mortality of 21.1% following major lower limb amputation. This finding is similar to previous research; however, we did have a lower 30-day mortality rate. This could be attributed to patient demographic and geographical differences. Aulivola et al. reported a 30-day mortality of 8.6% and a 1-year mortality of 30.3% in a series of 788 patients in the United States. 2 Belmont et al. reported a 30-day mortality of 7.0% in a series of 2911 patients, also in the United States. 17 Kelly et al. reported a 30-day mortality of 10.1% and a 1 year mortality of 43.1% in a series of 87 patients from the Royal Perth Hospital. 18 When looking at Indigenous patients, they had a 10% mortality rate at 30 days which is higher than the average population. As far as we are aware, this mortality rate has not been previously reported and can be highlighted perioperatively especially when advising of risks of lower limb amputations.
In our study, the 30-day mortality rate was higher for patients undergoing AKA compared with BKA, but this was not statistically significant (9.3% vs. 1.9%, p < 0.06). The 1-year mortality was similar between the AKA and BKA groups (25.6% vs. 20.2%, p < 0.3). Aulivola et al. reported a 30-day mortality of 16.5% following AKA and 5.7% following BKA, and a 1-year mortality of 49.4% following AKA and 25.5% following BKA. 2 In a systematic review by Thorud et al., there was a range of mortality after BKA of 40%–82% and after AKA of 40%–90%. 19 The relative 5-year survival rate in our study was 53%, which is lower than the relative survival of all cancers combined, at 58% for males and 64% for females. 20 This patient cohort has a high mortality risk, and strategies to facilitate early diagnosis and improve treatment are necessary.
The common comorbidities in our patient cohort included diabetes mellitus and PVD. This aligns with previous studies, both locally and internationally. 4,21,22 The majority of our patients (69%) had diabetes, which is substantially higher than the estimated prevalence of 7.4% of the adult population in Australia. 13 This finding supports previous studies that have shown diabetes to be the most common risk factor for major lower limb amputations. 4 Recognizing the extent of diabetes and PVD in our patient population is the first step in developing strategies to reduce the rate of major lower limb amputations. There is evidence that PVD is an independent risk factor for lower extremity amputation in patients with diabetes. 19,23 Using long-term models, patients with PVD had a higher risk of mortality. This indicates that PVD should be screened for in any patient undergoing an amputation to help minimize long-term sequelae.
Twenty-seven percent of our patient cohort had undergone previous ipsilateral minor amputations. This is similar to previous studies. Wrobel et al. reported a rate of 39%, Shah et al. reported a rate of 35%, and Lazzarini reported a rate of 44% in their respective cohorts. 4,7,24 There has been an increase in the rate of minor lower limb amputations compared to a steady rate of major lower limb amputations performed in Australia. 25 –27 While we did not investigate the overall rate of minor lower limb amputation at our center, our data suggest that limited amputation is not always successful.
Increasing levels of major amputation reflect failed limb salvage and increased mortality risk to patients. 19 There is a paucity of evidence in the literature regarding the risk of undergoing further major lower limb amputation. Amputations are generally performed as a last resort, but causative factors may include ongoing infection, poor diabetic control, and significant PVD. In our cohort, 13 amputees went on to have further major amputations. This has considerable psychosocial implications for the amputee and their family, not to mention economic costs to the healthcare system.
Our study does have a number of limitations. Being a retrospective review, we cannot confirm complete capture of all patients who underwent major lower limb amputation, and we are also limited to the data recorded in electronic and paper medical records. Accordingly, patient comorbidities, previous amputations, subsequent amputations, and complications may be underreported. Three patients were excluded from the study due to insufficient recorded data. However, our mortality data were obtained from the Queensland Registry of Births, Deaths and Marriages, so we are confident that this is accurate.
Toowoomba Hospital does not have a vascular or oncology surgery service, so some patients from our region may have received surgical care at a tertiary center in Brisbane. Additionally, minor general surgery procedures are performed at some of the smaller hospitals in our region (e.g. Roma and Kingaroy), and it is possible that amputations have been performed at these facilities. Hence, the overall major amputation rate for our region may be underreported. Since the inception of this study, Toowoomba Hospital has increased its podiatry service and initiated a high-risk foot service, with input from an endocrinologist, an orthopedic surgeon, podiatrists, wound care nurse specialists, diabetes educators, and Indigenous support officers. We are auditing the results of these interventions and we hope to see a reduction in our major amputation rate.
Conclusion
Major amputations are occasionally required for the management of end-stage lower limb pathology where salvage attempts have failed. We report a series of 147 cases performed at a regional Queensland hospital over an 18-year period. Morbidity and mortality following major lower limb amputation is high. We noted a 30-day mortality of 4.1% and a 1-year mortality of 21.1%. Thirteen amputees underwent subsequent (either ipsilateral or contralateral) major amputation. These findings highlight the importance of preventative measures to minimize the incidence of major lower limb amputations. These may include improving access to primary health-care facilities, improving health literacy and self-care, and improving access to specialist services such as endocrinology, multidisciplinary high-risk foot clinics, and vascular surgery.
Footnotes
Acknowledgments
The authors would like to thank the Toowoomba Hospital team who have been involved in this project; collecting the data and taking care of the patients. The authors also thank the Toowoomba Hospital Foundation for funding this project with AUD$3500.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Toowoomba Hospital Foundation.