
Abstract
Objectives: To explore job adjustments, job satisfaction, and health experience among employees with an upper limb amputation and to compare the results with those of lower limb amputees and control subjects.
Methods: Amputees were recruited from data files of a large European University Medical Centre and orthopaedic workshops. Controls were matched colleagues of the lower limb amputees. All participants filled out the VAG questionnaire (Vragenlijst Arbeid en Gezondheid), assessing job satisfaction and job adjustments, and the RAND-36.
Results: 28 upper limb amputees were compared to 144 lower limb amputees and 144 controls. Job adjustments were necessary in 38% and 28% of upper and lower limb amputees, respectively. All three groups were equally satisfied with their jobs (p = 0.90). Vocational rehabilitation was applied to 26% and 8% of upper and lower limb amputees, respectively. Upper limb amputees rated their general health worse (18 points, 95% CI: 12–25) compared to lower limb amputees, corrected for effects of confounders (age and co-morbidity).
Conclusions: Upper and lower limb amputees have high job satisfaction and a minority need job adjustments. In upper limb amputees, the causes of the worrisome general health experience need further investigation. In upper and lower limb amputees, vocational rehabilitation deserves additional attention.
Introduction
Job satisfaction and job participation play an important role in people's perception of well-being. Lower limb amputees show a relatively high grade of job participation compared to people with other diseases or handicaps or compared to healthy persons.1-3 Furthermore, lower limb amputees tend to be more satisfied with their occupational status than controls.2 After an upper limb amputation, job reintegration is high,4,5 but nothing has yet been revealed on job satisfaction after an upper limb amputation.
An amputation of an upper or a lower limb has also been associated with lost work time, loss of employment and loss of income, fewer possibilities for job promotion, hiring or job training.1,3,5,, 6-9 One of the factors related to these negative work consequences may be the amputee's physical limitations.9 The mobility impairment in lower limb amputees may result, among others, in decreased walking speed, lower endurance or decreased standing time.9 Upper limb amputees may encounter problems with executing two handed activities and fine motor skills or carrying heavy loads, despite the use of a prosthesis.9 To overcome these physical limitations, adjustments to the workplace, such as changes in working time, getting aids, changes in workload, other tasks or extra training could be necessary.3 In lower limb amputees, such adjustments appeared to be important for enabling them to continue their work.1,3,7 To what extent adjustments to the workplace facilitate the work of upper limb amputees, has been described only minimally.9
Upper limb amputations predominantly are of traumatic origin and occur mostly at a young age.4,10 In contrast, the majority of lower limb amputations are performed because of vascular problems, which generally take place at middle age or later.11 As a consequence, it may be expected that upper limb amputees will have many productive life years ahead after the amputation. Nevertheless, little is known about health-related problems upper extremity amputees encounter while fulfilling their job. The aim of the study is to explore the job satisfaction, job adjustments and health experience of upper limb amputees in comparison to historical data of lower limb amputees and controls.
Patients and methods
Patients
All upper limb amputees, registered at the centre for rehabilitation, the surgery clinic, the oncology clinic or the plastic surgery clinic of a large European University Medical Centre during the last two decades were eligible for the study. Furthermore, the regional orthopaedic workshops were asked to identify patients who were provided with arm prostheses. Finally, the website of the national association of limb amputees was used to contact amputees who were willing to participate in the study.
Included were patients between 18 and 65 years of age, with known addresses, who had a paid job or were performing a study at the time of amputation. All patients were unilaterally amputated at the level of the wrist or more proximally at least three months prior to the study. Patients who suffered from severe cognitive or psychiatric illnesses, patients who suffered from other illnesses which led to inability to work, and patients who had insufficient command of the national language and could not fill out the questionnaire, were excluded.
The findings in these upper extremity amputees were compared with historical data of 144 lower extremity amputees and their matched controls.2
Methods
All patients filled out a questionnaire concerning age, sex, hand dominance, level of education, co-morbidity, reason of amputation, level and site of amputation and the use of a prosthesis. To assess job characteristics, the questionnaire Vragenlijst Arbeid en Gezondheid (VAG) of the TNO (Organization for Applied Scientific Research) Vocational Handicap Research Program was used.12-15 The VAG assesses job demands, opinion on working conditions, social atmosphere at work and (dis)abilities of the subject, as well as adjustments at work and vocational handicaps. Eight aspects of job satisfaction were analyzed in the current study: the general judgement of the job, job content, physical and mental exertion, work organization, management and colleagues, relationship between work and private life, appreciation and job perspective, physical working conditions and safety. The TNO questionnaire has been validated in several research projects, where the internal consistency was reported as good.12,13,15
All items can be answered by ‘yes' or ‘no’, except for the first item, the general judgement of the job. This question could be answered with ‘good’, ‘reasonable’, ‘moderate’ or ‘bad’. The results of this question were dichotomized into two categories: good job satisfaction (good or reasonable) or insufficient job satisfaction (moderate or bad). Jobs were dichotomized in two groups: ‘white-collar’ (administrative, commercial, scientific and technical workers) and ‘blue-collar’ (agrarian, traditional, industrial, servicing and transport workers).
The general health status was assessed using the Medical Outcomes Study 36-Item Short Form Health Survey (SF-36), the RAND-36.16 The RAND-36 is a shortened version of the RAND Health Insurance Study Questionnaire. It measures perceived health status in nine dimensions: physical functioning, social functioning, physical role limitations, emotional role limitations, mental health, vitality, pain, general health and change of health. A higher score on the RAND-36 reflects a better health experience.
Statistical analysis
Statistical analyses were performed using Statistical Product and Service Solutions Software (SPSS 14.0). Differences in mean age and the domains of the RAND-36 between upper limb amputees, lower limb amputees and the control group were analysed using ANOVA and a Games-Howell post hoc analysis. Differences between upper and lower limb amputees in sex, present type of job, level of education, co-morbidity, reason of amputation, level of amputation, participation in vocational rehabilitation and job adjustments were analysed using Chi-square tests, Fisher's Exact Test or the Kruskal Wallis test as appropriate. To analyze differences in general health, a multi-variate regression analysis (backward) was performed with general health as outcome variable and age of amputee (in years), amputation (lower limb = 1, upper limb = 0), level of amputation (proximal from elbow/knee or through elbow/knee = 0, distal from elbow/knee = 1), traumatic amputation (yes = 1, no = 0) co-morbidity (yes = 0 no = 1) as predictor variables. A p-value of ≤0.05 was considered to be a statistically significant difference.
Medical Ethics Committee
The study was approved by the local medical ethics committee.
Results
Questionnaires were sent to 65 potential upper limb amputees with known address. Twenty participants reported that they were not willing to join the study without giving a reason. Seventeen patients did not return the questionnaire. In total, 28 patients were included in the study.
Patient characteristics
Demographic characteristics
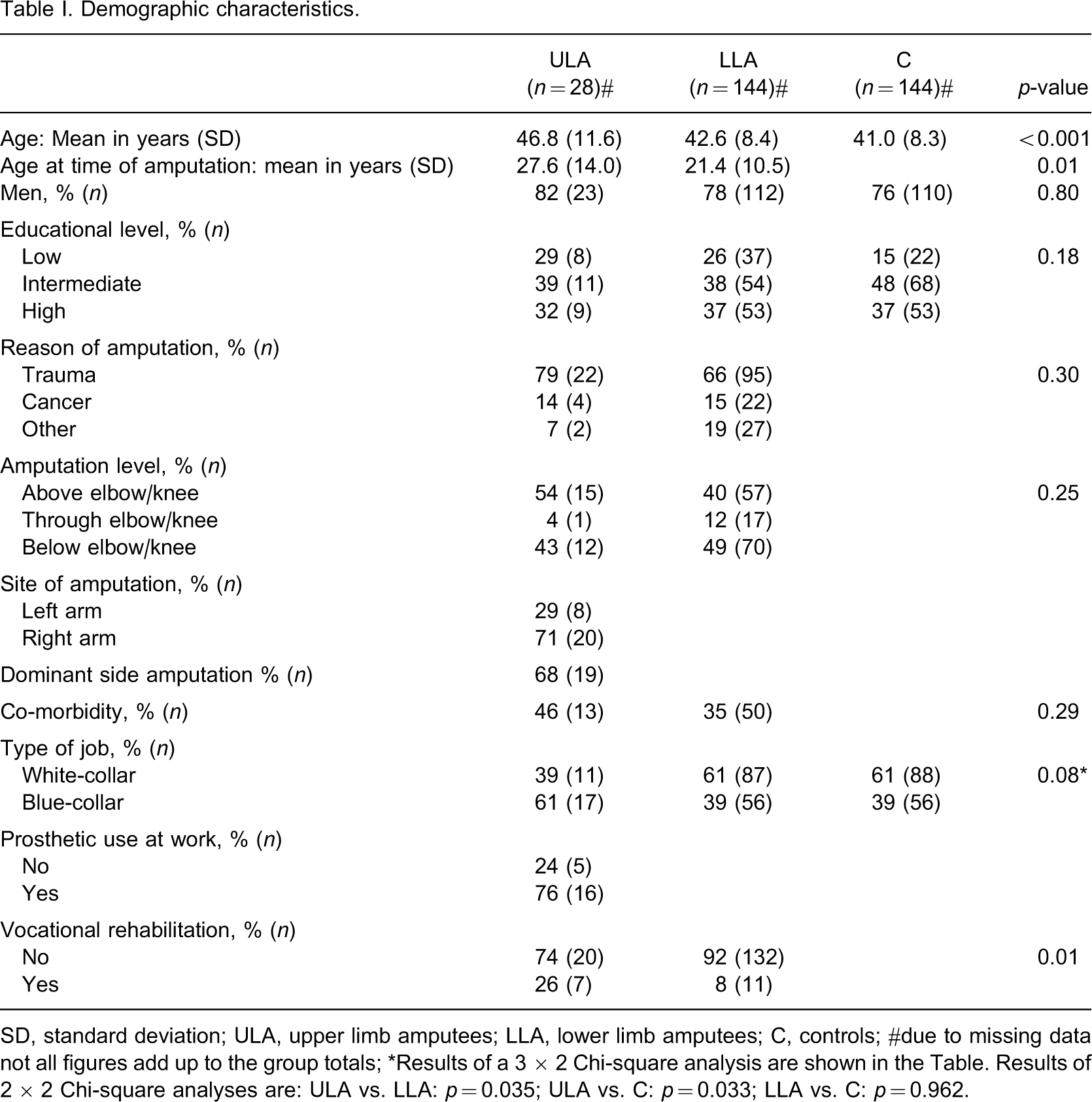
SD, standard deviation; ULA, upper limb amputees; LLA, lower limb amputees; C, controls; #due to missing data not all figures add up to the group totals; ∗Results of a 3 × 2 Chi-square analysis are shown in the Table. Results of 2 × 2 Chi-square analyses are: ULA vs. LLA: p = 0.035; ULA vs. C: p = 0.033; LLA vs. C: p = 0.962.
All 28 upper limb amputees were working at the time of amputation. Twenty-one of them (75%) were still working at the time of the study. Two participants were retired due to age and five received disability benefits. Eighty out of the 144 lower limb amputees were receiving an education at the time of the amputation. At the time of the study, all lower limb amputees and controls were working. A blue-collar status was found in 61% of the upper limb amputees (n = 17), and in 39% of the lower limb amputees (n = 56, p = 0.035), and 39% of the controls (n = 56, p = 0.033). No differences in blue or white collar status were found between lower limb amputees and controls (p = 0.962). After the amputation, three upper limb amputees and 16 lower extremity amputees revealed a change from a blue collar job to a white collar job (p = 0.662). Three quarters of the working upper limb amputees used a prosthesis during work (76%, n = 16). Twenty-six percent (n = 7) of the upper limb amputees and 8% (n = 11) of the lower limb amputees underwent vocational rehabilitation (p = 0.01).
Job adjustments
Job adjustments
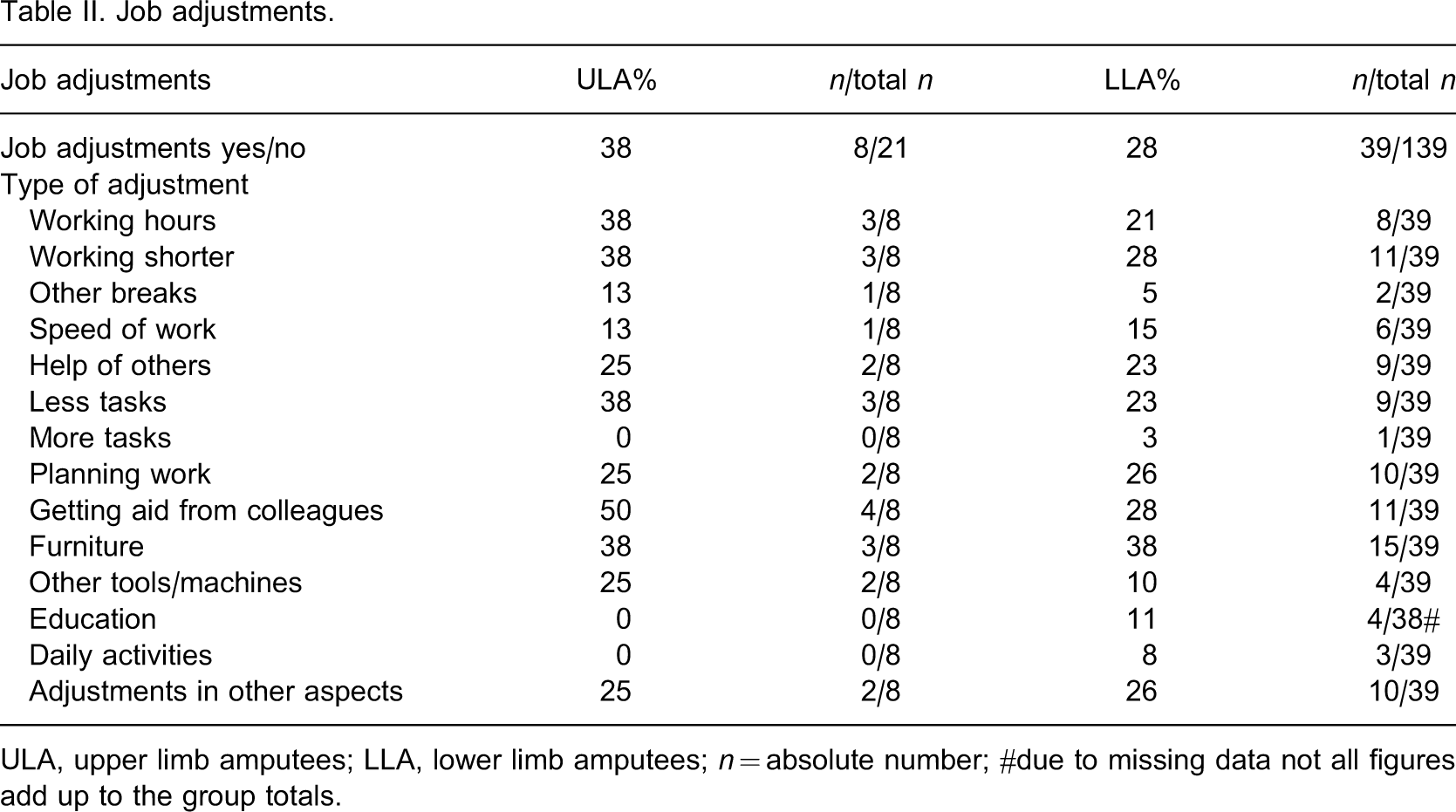
ULA, upper limb amputees; LLA, lower limb amputees; n = absolute number; #due to missing data not all figures add up to the group totals.
Job satisfaction
Job dissatisfaction
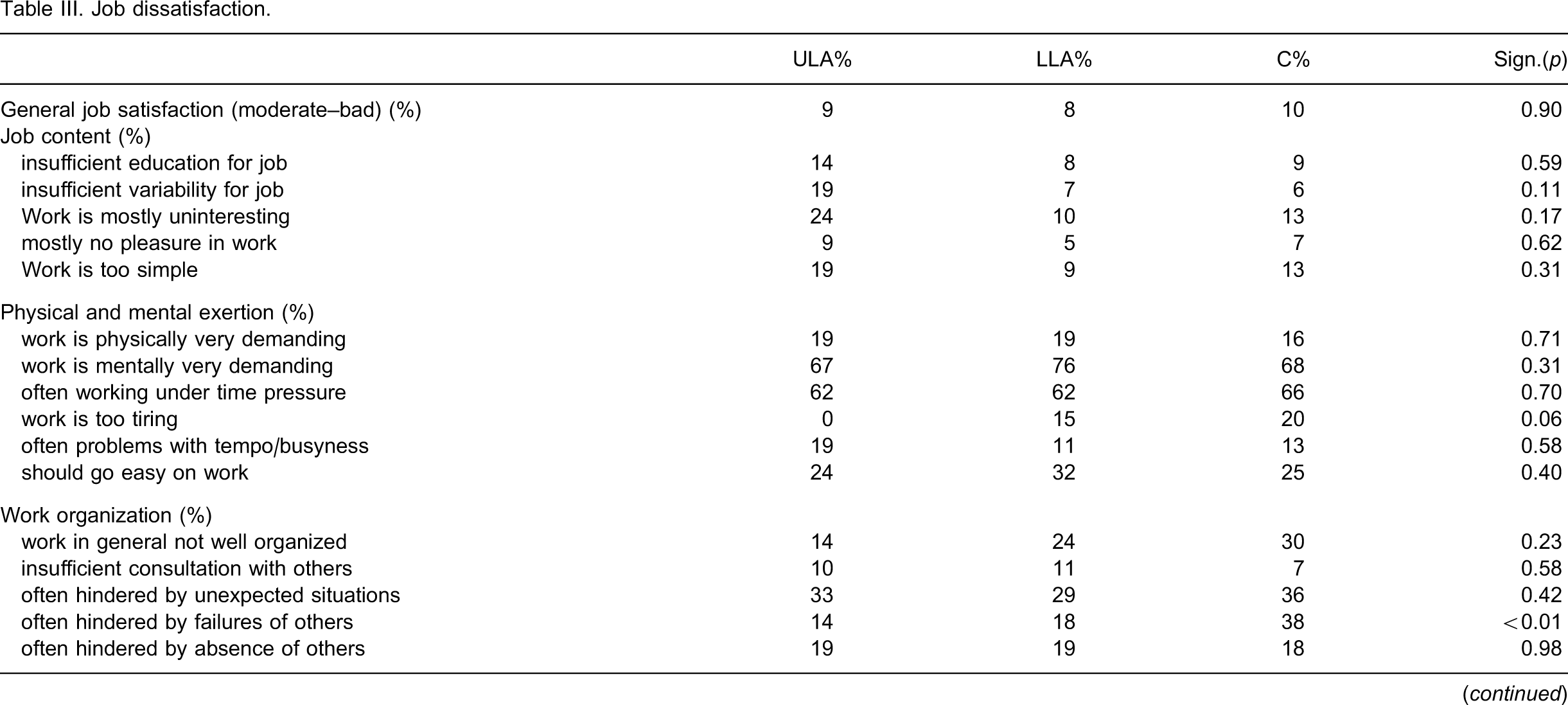
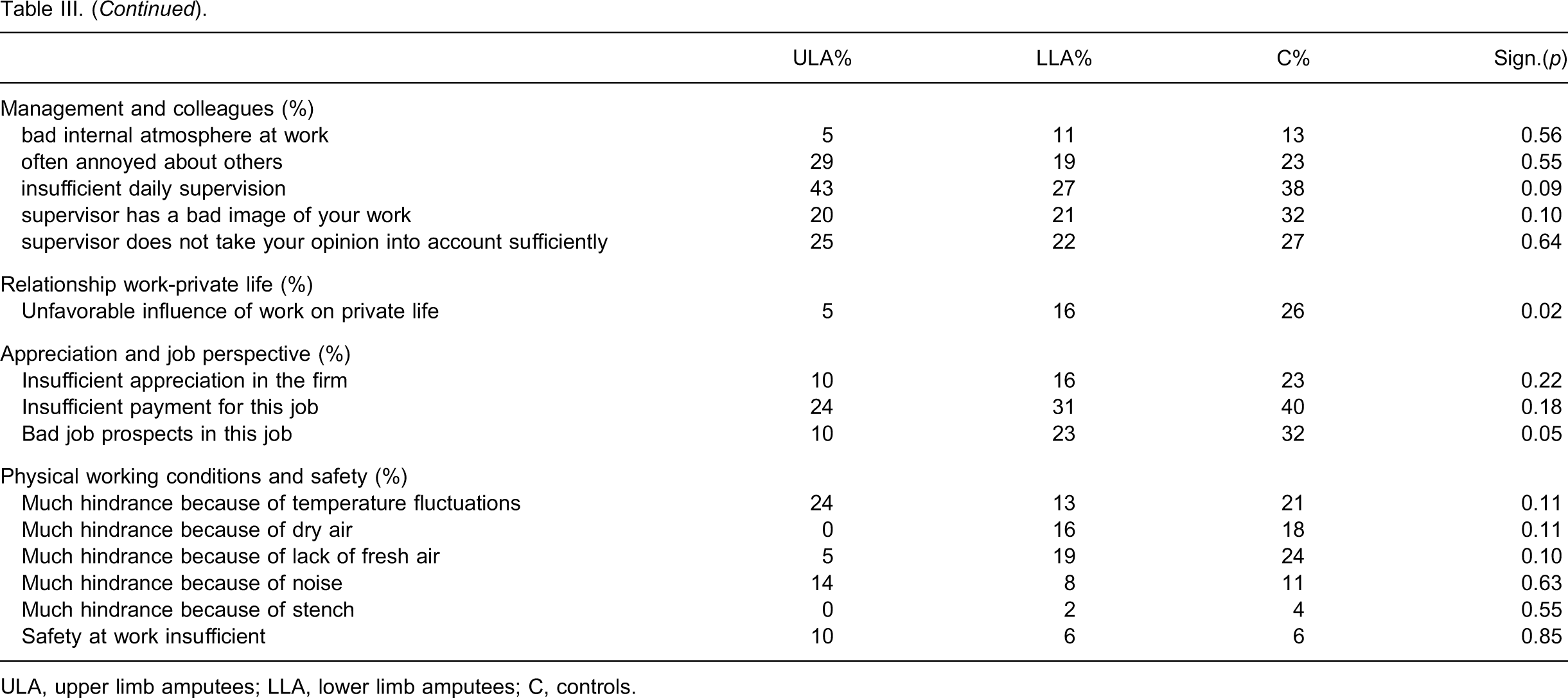
ULA, upper limb amputees; LLA, lower limb amputees; C, controls.
Health status
Health status
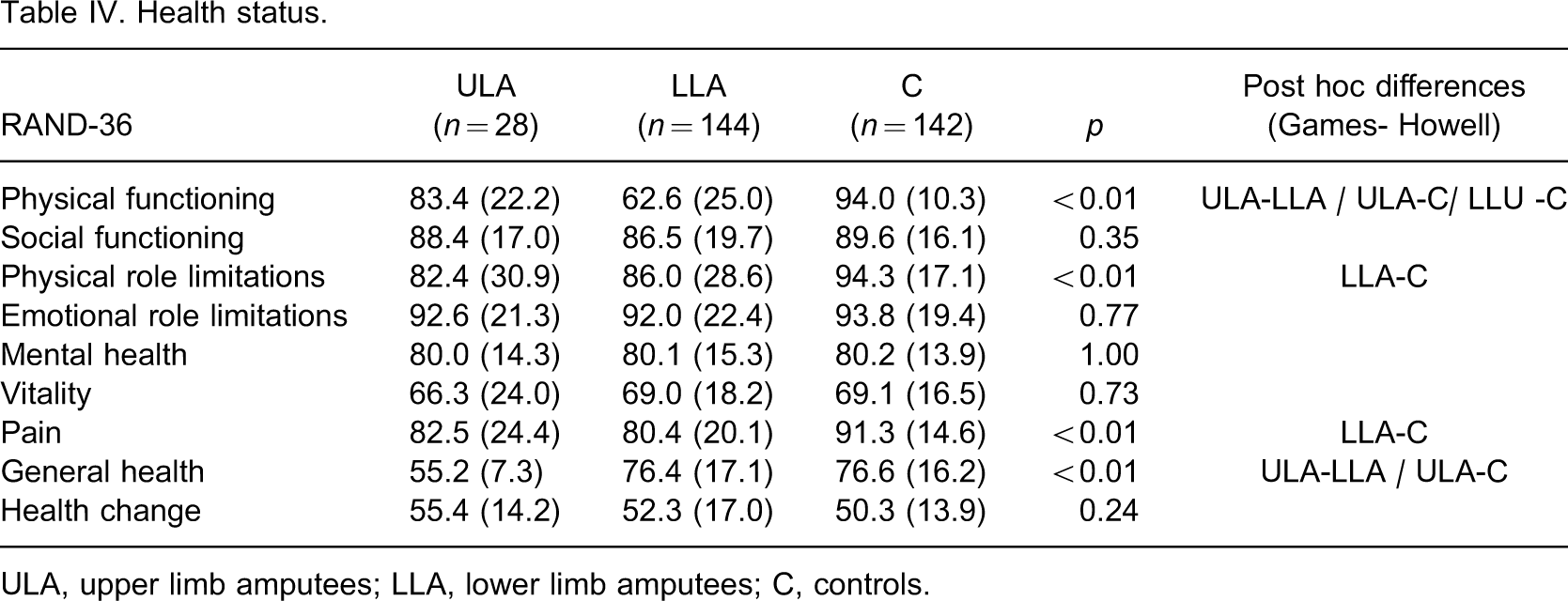
ULA, upper limb amputees; LLA, lower limb amputees; C, controls.
Results of regression analysis (backward) with general health as outcome variable and age, amputation, and co-morbidity as predictor variables
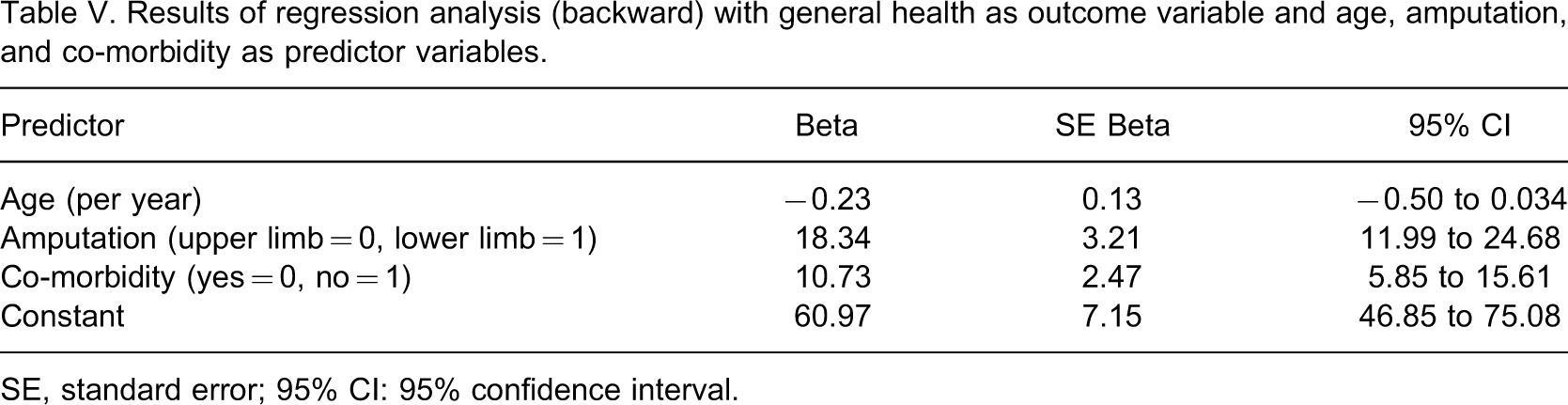
SE, standard error; 95% CI: 95% confidence interval.
Discussion
Job adjustments
Only in a minority of both upper and lower limb amputees job adjustments were needed. We expected a considerable need for job adjustments, especially in upper limb amputees of whom the majority was blue collar workers. Generally, blue-collar jobs are more physically demanding than white-collar jobs. Furthermore, we expected that the loss of an arm would be more of a hindrance when performing jobs than the loss of a leg. Our finding is important for employers, since it means that it is not necessarily a huge financial burden to employ an amputee.
In the current study a higher percentage (68%) of upper limb amputees suffered an amputation of the dominant arm, compared to previous data (51-59%).4,10 It seems plausible that loss of a dominant limb will lead to additional difficulties in work performance. However, loss of the dominant arm does not influence return to employment.5,17
Job satisfaction
General job satisfaction was comparable in all three groups. Although it is known that blue collar workers are generally less happy than white collar workers,18 the general job satisfaction was not influenced by the differences in proportions of blue and white collar workers among the three groups. Upper limb as well as lower limb amputees showed similar or better satisfaction rates than controls on all items. On three items of the VAG (hindered by failures of others, influence of work on private life, and job prospects) upper limb amputees were significantly less dissatisfied than lower limb amputees and controls. These findings confirm the tendency that disabled people appreciate their jobs more favorably than healthy people.13 Despite this tendency, in several items of the VAG substantial dissatisfaction was present among amputees, which needs further attention.
Strikingly, only a minority of both upper and lower limb amputees received vocational rehabilitation despite the fact that an amputation has consequences for job reintegration and job participation. It is conceivable that the amputees did not have a need for vocational rehabilitation, but such information was not gathered in the present study. Generally, vocational rehabilitation is financially beneficial for those who were re-integrated into working life, and successful vocational rehabilitation also leads to increased social well-being compared to those who did not receive vocational rehabilitation.19 In this respect, early prosthetic fitting, training, and early return to work will facilitate successful functional recovery.20 In future research it might be worth investigating the need for vocational rehabilitation and the effect of vocational rehabilitation on return to work, adjustments and social well-being in upper limb amputees.
Health status
Upper limb amputees experience better physical functioning compared to lower limb amputees. The physical functioning subscale of the RAND36 includes six items on walking, climbing flights of stairs, walking a specific distance, bending and kneeling and four items on upper limb activities such as carrying groceries, bowling, playing golf or dressing. As such, most items are less applicable to measure functional impairments in upper limb amputees and may have resulted in the (artificial) significant difference between upper and lower limb amputees on the physical functioning subscale.
Most striking was the finding that the upper limb amputees judged their general health worse than lower limb amputees and controls. This difference between upper and lower limb amputees was independent of the effects of co-morbidity and age. Differences in experiencing (phantom) pain probably are also not the explanation for this result, since pain scores on the RAND-36 of upper limb amputees did not differ significantly from both other study groups. An explanation for the worse general health experience of upper limb amputees might be the fact that an upper limb amputation leads to major restrictions in functioning.11 However, this assumption is not confirmed by the scores on physical role functioning. Furthermore, it is stated that adapting to functioning with one arm is a major challenge and often costs much effort to gain meaningful employment, which may lead to a deterioration of experienced general health.21 This finding is not confirmed by our results with respect to job adaptations, although five upper limb amputees stopped working after the amputation and received disability benefits. Previously, it has been described that upper limb amputees experience a better health status than lower limb amputees, measured by the Nottingham Health Profile (NHP).22 However, in concordance with the physical functioning subscale of the RAND-36, many items of the NHP inquire after lower limb-related disabilities. As such, health status results in upper limb amputees remain confusing. We emphasize the need to develop a specific instrument measuring the health status of upper limb amputees.
Limitations
A limitation of this study is the small number of upper limb amputees that participated in the study. The low incidence rate of upper limb amputations in The Netherlands may be one explanation for the small number of amputees that could be reached (the incidence of upper limb amputations in our country is estimated at 0.26 per 100.000 inhabitants).23 Secondly, a considerable group of potential participants were unwilling to participate, despite several efforts of the researcher. Reasons for not willing to participate were not mentioned in most of the cases. One possible reason might be aversion for filling out the questionnaire because of the relatively large size of the questionnaire.
Another limitation of the study is a point of statistical concern: the difference in group sizes between upper limb amputees and lower limb amputees on the one hand and the controls on the other hand. As such, a Games-Howell procedure was used in the post hoc analysis of the ANOVA results.
A final limitation of the study is the difference in age between both amputee groups. The upper limb amputees appeared to be older than the lower limb amputees, whereas upper limb amputees are generally younger than lower limb amputees.4,11 This difference in age between the amputees may have been the result of inclusion criteria of the lower limb amputees, since only working lower limb amputees were eligible for the study.2 As such, comparable inclusion criteria for all groups are advised in further research. The difference in age may have introduced some bias, although it is not easy to estimate the size or the direction of this bias.
Conclusions
Only a minority of upper and lower limb amputees need job adjustments and the amount of job adjustments between both groups was similar. This finding is relevant information for employers who may be reserved to engage amputees because of possible financial consequences. Upper limb amputees were equally satisfied with their jobs in general compared to lower limb amputees and controls. The need for vocational rehabilitation and the effect of vocational rehabilitation on job satisfaction of amputees need further attention, since only a minority of the amputees received vocational rehabilitation. Upper limb amputees experienced a worse general health compared to lower limb amputees and controls. To explain this worrisome finding, further research with health status measurements that are specifically applicable to upper limb amputees is needed.