
Abstract
Background:
Through play, children develop motor, cognitive, social, and other life skills. Play barriers can impede physical and psychosocial benefits.
Objectives:
We describe participation in active play, fundamental movement skills, play environment characteristics, and potential play barriers for school-aged children (6–12 years) who use lower extremity prostheses.
Study design:
Cross-sectional questionnaire study.
Methods:
A questionnaire was developed and administered online to parents of children 6–12 years who use lower extremity prostheses. Questions focused on children’s valued play activities, participation in active play, fundamental movement skills, body positions for play, and characteristics of play environments.
Results:
Parents (n = 26) reported their children who use lower extremity prostheses participated in a range of activities including active play (e.g. playgrounds, swimming). Fundamental movement skill limitations were identified (e.g. walking long distances, running fast, hopping on one foot, and skipping). Mobility limitations with floor positions, movement transitions, and uneven or sloped surfaces were reported. Active play with equipment such as roller skating, climbing structures, and bicycling presented challenges.
Conclusion:
Parents of children who use lower extremity prostheses reported participation restrictions associated with mobility limitations, activity type, and built environment characteristics (e.g. surfaces and equipment). Challenges made it difficult for children who use lower extremity prostheses to keep up with peers in schools and communities.
Clinical relevance
Understanding potential barriers to participation in active play of children who use lower extremity prostheses may contribute to enhanced prosthetic design, rehabilitation strategies, universal design of play and built environments, and improved outcome measures ultimately enabling these children to participate fully in active play in diverse contexts.
Background
Play is a vital developmental activity for children. The United Nations Convention on the Rights of the Child recognizes play as a human right in that “every child has the right to rest and leisure, to engage in play and recreational activities appropriate to the age of the child and to participate freely in cultural life and the arts.” 1 Participation in play is a cornerstone of contemporary models of health-related rehabilitation such as the World Health Organization’s International Classification of Functioning, Disability, and Health—Child and Youth (ICF-CY) framework. 2
Participation is defined as a person’s “involvement in life activities.” 2 Participation in active play is essentially participating in physical activity with spontaneous and occasional bursts of high energy. It can occur indoors or outdoors, alone, or with friends and family. Even before children can walk, they start playing. As they get older and learn more skills, opportunities for active play increase. 3
Participation in active play is an important indicator of function, health, and quality of life. 4 Through participation in active play children develop motor, cognitive, social, and other life skills that have physical and mental health benefits. 5 Active play, such as movement games and playing in playgrounds, engages gross motor functions, stimulates physical development, and the growth and use of fundamental movement skills. 6 Fundamental movement skills are commonly developed in childhood and subsequently refined into context- and sport-specific skills. Fundamental movement skills include locomotor (e.g. running and hopping), manipulative or object control (e.g. catching and throwing), and stability (e.g. balancing and twisting) skills. 6
Active play promotes long-term fitness and well-being. Participation in active play also supports psychological development through the development of mastery, self-efficacy, self-confidence, peer interaction, and social skills. 7 In contrast, children who experience active play barriers, lag in the development of fundamental movement skills, do not feel good about their play experiences, and are at risk for secondary behavioral health problems such as anxiety, depression, and social isolation or secondary health problems associated with inactivity such as obesity. 5
Children with physical disability are at risk for the consequences of low physical activity levels in the areas of physical health, mental health, and social interaction. 8 However, little is known about the active play experiences of children who use lower extremity prostheses (LEP) and subsequent health effects. Approximately 25,000 children in the United States use LEP. 9 About 750 babies are born each year in the United States with lower extremity reductions. 10 In addition, infections, 11 cancer, 12 and traumatic events 13 can result in a medical need for amputation. The life expectancy of children who use LEP is similar to peers. Therefore, these children will need prostheses for a lifetime and the challenges and consequences of prosthetic use will be long term.
The literature indicates that participation in play is a essential life activity that is influenced by a variety of child, family, and environment facilitators and barriers. 8 Adults who use LEP report that participating in active play as a child were among the earliest challenges they experienced. 14 Active play experiences, including corresponding facilitators and barriers, of children who use LEP are not well documented. Yet, this population of children may be at risk for experiencing challenges that impede their participation in active play.
Anecdotal information from adults who use LEP indicates that they experienced play barriers as children. For example, when asked about childhood playground experiences, a university student with bilateral congenital lower extremity amputations said: “Frankly, all of them had difficult parts, but climbing ropes, rope ladders, things with holes that my foot can slip through … I felt the most guilt knowing that I was the slowest physically to get to the destination.” 14
Adults with amputations report challenges of working on the ground; moving in cramped spaces; moving sideways and backward; traversing uneven ground, slopes, slippery, or soft surfaces; climbing on and off step stools and ladders; as well as standing and sitting tolerance.14–16 Childhood play activities may require similar movement demands and occur in different environments within the home, neighborhood, school, and community contexts.
Although literature specific to participation in active play for children who use LEP is limited, research using clinical and laboratory tests have revealed movement differences. One case–control study showed that children who used LEP compared to controls had significantly poorer scores on the Functional Mobility Assessment, the Timed Up and Go, the Timed Up and Down Steps, and the 9-Minute Walk Distance. 17 Two other case–control studies found gait asymmetries and poorer balance for children using prostheses compared with age- and sex-matched controls.18,19 Although simple walking tests do not reflect movement patterns that would be required in more complex environments that children must navigate during active play, it may be assumed that these differences would be exacerbated by more complex movement and environmental demands.
In studies of children with physical disability, a wide range of child, family, and environmental factors, such as the child’s motivation and health status, family resources, and features of the physical and social environment, have been identified as facilitators or barriers that influence children’s participation in leisure, recreation, and play.8,20,21 Similarly, for children who use LEP, it is important to understand the child, family, and/or environment factors that influence participation in active play and the barriers to play, as in other areas of daily life function. While there may be similarities to children in other diagnostic groups or with other orthopedic, past and current medical conditions, children who use LEP have important unique differences, including the use of prostheses. We wanted to know whether, how, and where children who use LEP participate in active play and the potential barriers to active play they may experience.
The purpose of this study was to explore participation in active play of elementary school-aged children who use LEP, with an emphasis on fundamental movement skills, characteristics of play environments, and other potential barriers to active play. A secondary aim was to examine trends by age and function level as selected child factors that may influence participation in active play.
Methods
Study design and inclusion criteria
This was a cross-sectional exploratory descriptive study. Parents of children 6–12 years old, who used LEP, were invited to respond to an online questionnaire. The parents needed to read English and have Internet access. Parents of children with only upper extremity limb loss were excluded. This study was approved by the University of Washington, Human Subjects Institutional Review Board.
Procedures
Flyers that included the link to the questionnaire were posted and distributed nationally by rehabilitation professionals and community organizations that supported children who use LEP. Word of mouth, personal contacts, social media, and listservs were also used to recruit participants. In addition, the study was advertised on the Amputee Coalition website (http://www.amputee-coalition.org/). Participants who offered their contact information were asked to help distribute information regarding the questionnaire. This process of snowball sampling has been used previously in studies for recruitment of rare populations. 22
Analysis/questionnaire development
A well-developed questionnaire, specifically targeting participation in active play of children who use LEP, does not exist. Therefore, an experienced, interprofessional, clinical, and research team of two physical therapists, an occupational therapist, and a certified prosthetist/orthotist developed a 21-question, 10-min anonymous online questionnaire (Appendix). The team collaboratively developed and reviewed the questionnaire items to cover child demographics, a representative sample of children’s sedentary and active play activities, fundamental movement skills that included common body positions for play, and characteristics of play environments.
Parents were asked to indicate their child’s preferred activities (e.g. What types of activities does your child enjoy? What physical skills does your child have difficulty with?) and rank the child’s level of difficulty with positions or environmental conditions (e.g. Rank the ground surfaces from least (1) to most (5) challenging for your child to play on). Open-ended questions were included so that parents could comment on specific types of challenges with play in home, school, or community environment contexts. For example, parents were asked to briefly describe any specific challenges (if any) their child experienced with activities in the community.
The questions were informed by the literature on mobility challenges for children with other disabilities and published research on analogous activity limitations and participation restrictions for adults who use LEP. For example, adults who use LEP report challenges working on the floor, moving from the floor to other postures, comfort with foot position on ladders or motorcycle pedals, and mobility on uneven ground and other surfaces.14,16
Questions also reflected play activities and expectations of fundamental movement skills that would be developed by children in this age range. When children enter elementary school around 6 years of age, fundamental movement skills (e.g. hopping, skipping, and jumping) required to participate in active play are present and practiced. 23 Context-specific skills such as running speed, ball skills such as throwing, catching or kicking, and coordination of higher level movement patterns are refined and advanced based on opportunities within the culture, expectations, and environments of the child and family. We expected that 6- to 12-year-old children, the target population in this study, would have a basic set of fundamental movement skills and be able to move freely in different play environments with skills that facilitate participation at a level comparable to same-aged peers with typical development.
Data analysis
Means for rank-order questions and summary counts and percentages for categorical multiple-choice questions are presented. Using conventional content analysis, 24 responses to the three open-ended questions regarding community, school, and playground participation were reviewed by the research team and grouped based on the following themes that emerged: prosthetic, activity, participation, and environmental factors.
Results
In all, 29 parents of children who use LEP completed the questionnaire. Three questionnaires were excluded from data analysis. Two parents completed the survey, but did not meet the study inclusion criteria due to child’s age and only upper extremity amputation. One parent questionnaire had inadequate data.
Demographic characteristics of children who use LEP
The parents’ children consisted of 12 males and 14 females across the following age groups 6–7 years (n = 7), 8–10 years (n = 14), and 11–12 years (n = 5) and a median age of 9 years. Children had wide-ranging amputation levels (Table 1). A small number of children in the sample had other medical conditions that included scoliosis (n = 1), vision impairment (n = 1), infection (n = 1), and additional lower extremity orthopedic problems (n = 3).
Participant demographics.
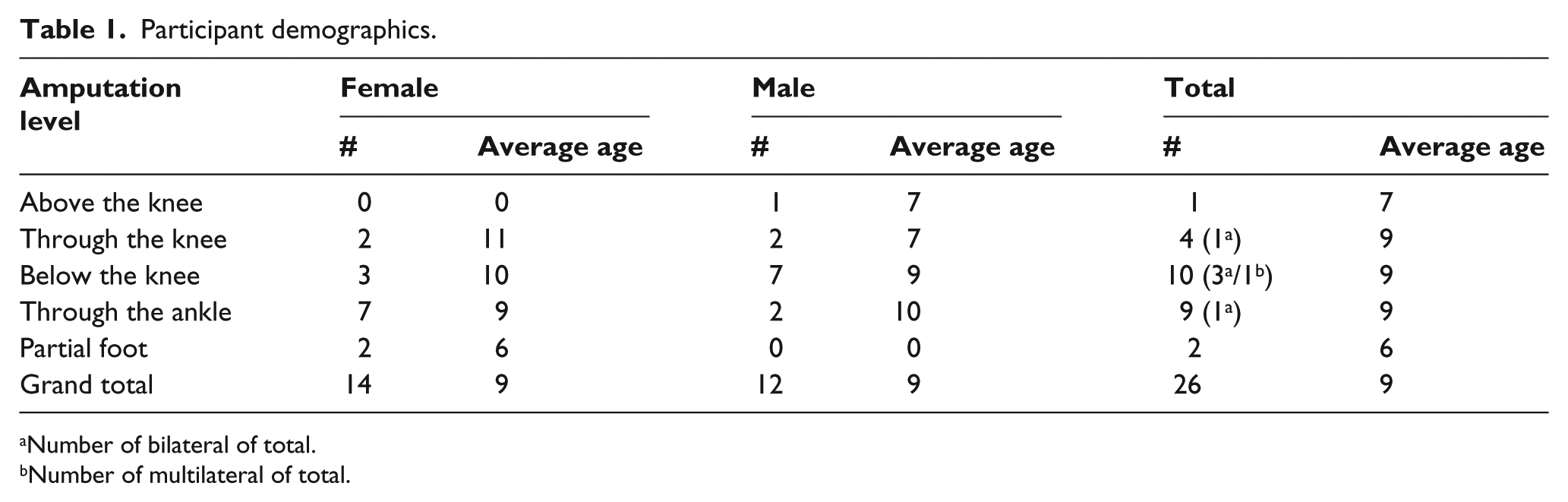
Number of bilateral of total.
Number of multilateral of total.
Participation in active play
Parents reported that their children enjoyed a variety of sedentary and active play activities (Table 2). Almost all of the children were reported to enjoy participation in play activities involving playgrounds, swimming, outdoors, and nature and parks. A lower percentage of children were reported to enjoy activities such as dancing, team sports, martial arts, and gymnastics. In all, 58% of parents reported that their children participated in playground games with their peers, but about the same amount of parents (57%) also noted that their children were not adequately keeping up with peers.
Preferred play activities (26 respondents, n, % of respondents).
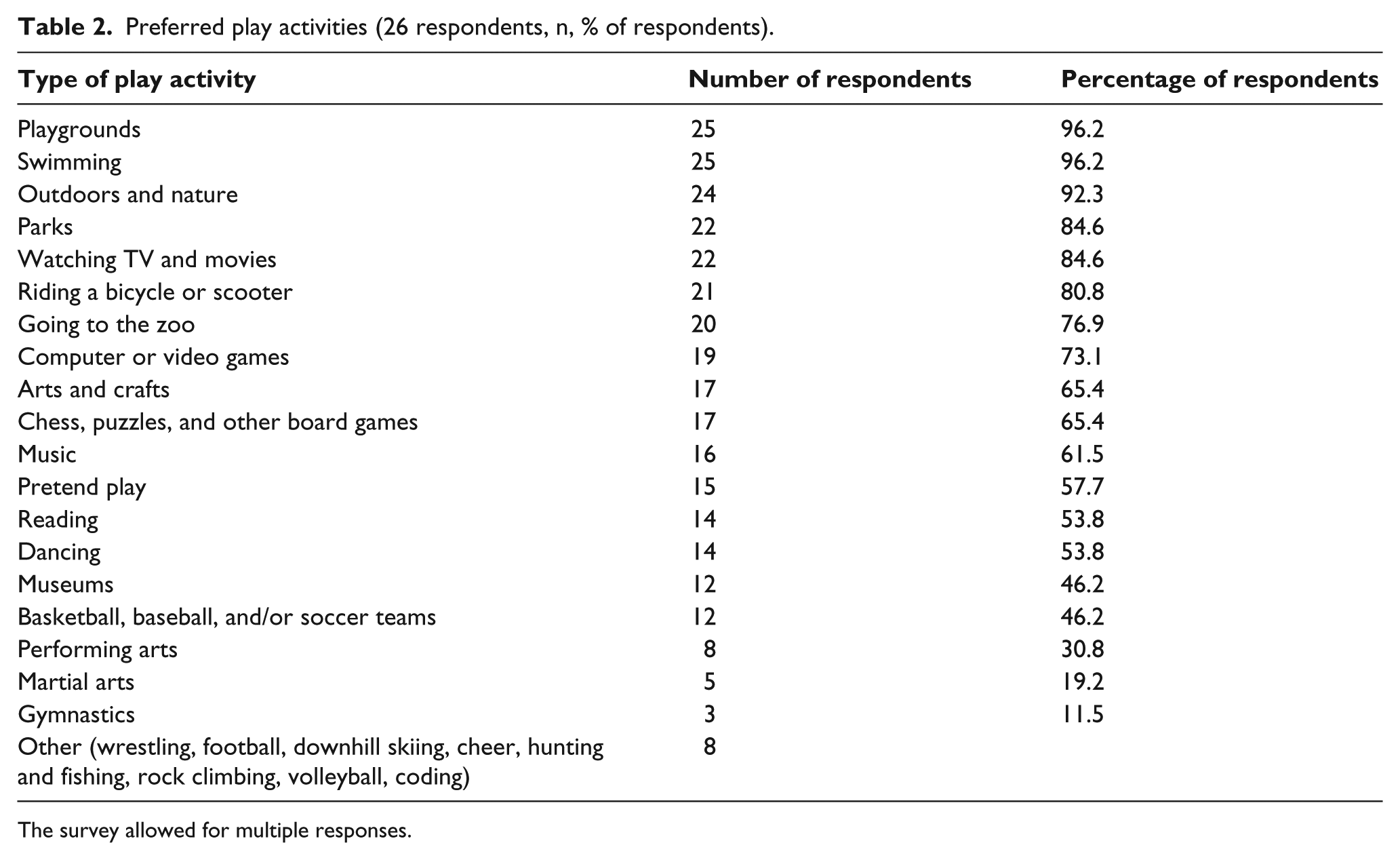
The survey allowed for multiple responses.
Movement skills
Parents reported that their children who use LEP had challenges with sitting, transitional postures, and mobility. For 56% of the parents, postures identified as the most difficult positions when playing on the floor for their children included sitting with legs crossed and sitting on heels. Other parents noted the most difficult position as sitting on heels (n = 5), kneeling (n = 4), side-sitting (n = 3), and crawling (n = 2). A total of 69% of parents reported that their child had some difficulty in moving between positions on the floor. According to 54% of the parents, sitting and moving around in cramped narrow spaces posed difficulties for their children and 58% of the parents reported their children to fall two or more times a week.
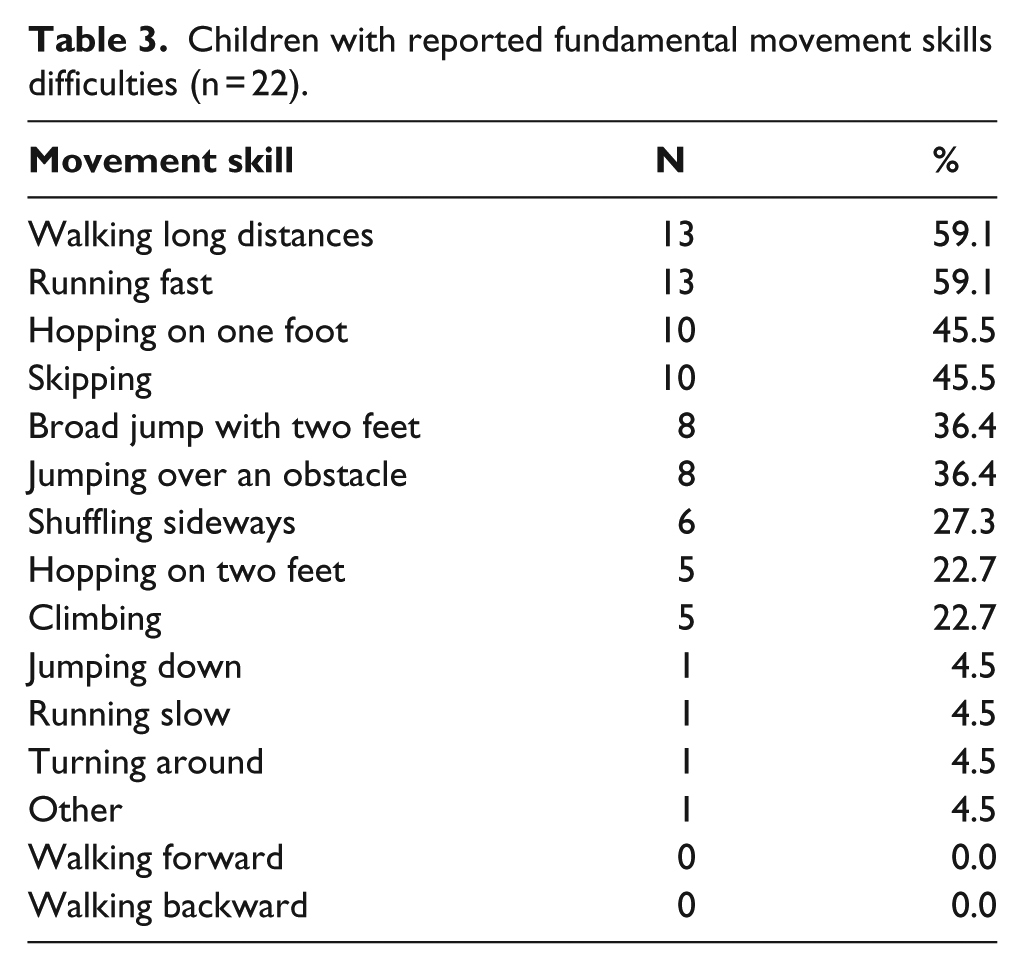
Fundamental movement skills (Table 3) that required endurance (walking long distances, 59%), speed (running fast, 59%), strength (hopping on one foot, 46%), and coordination (skipping, 46%) were rated by more parents as difficult, whereas simple movements, such as walking forward or backward were not difficult (0%). Play activities that involved equipment and required more strength or coordination, such as roller skating or climbing on play structures, were also rated as problematic by more parents.
Children with reported fundamental movement skills difficulties (n = 22).
Environmental features
Figure 1 represents the number of children who use LEP who reported level of the relative ease or difficulty of mobility on different environmental surfaces and conditions they might face during active play. In response to ranking different surfaces from least (1) to most (5) challenging, less complex surfaces (e.g. flat, grass) were reported as easier compared with uneven, sloped, and softer surfaces. Gravel and sand were rated as the most difficult surfaces. More specifically, 100% of the children rated flat surfaces as the least challenging, whereas 63% rated sand as the most challenging.
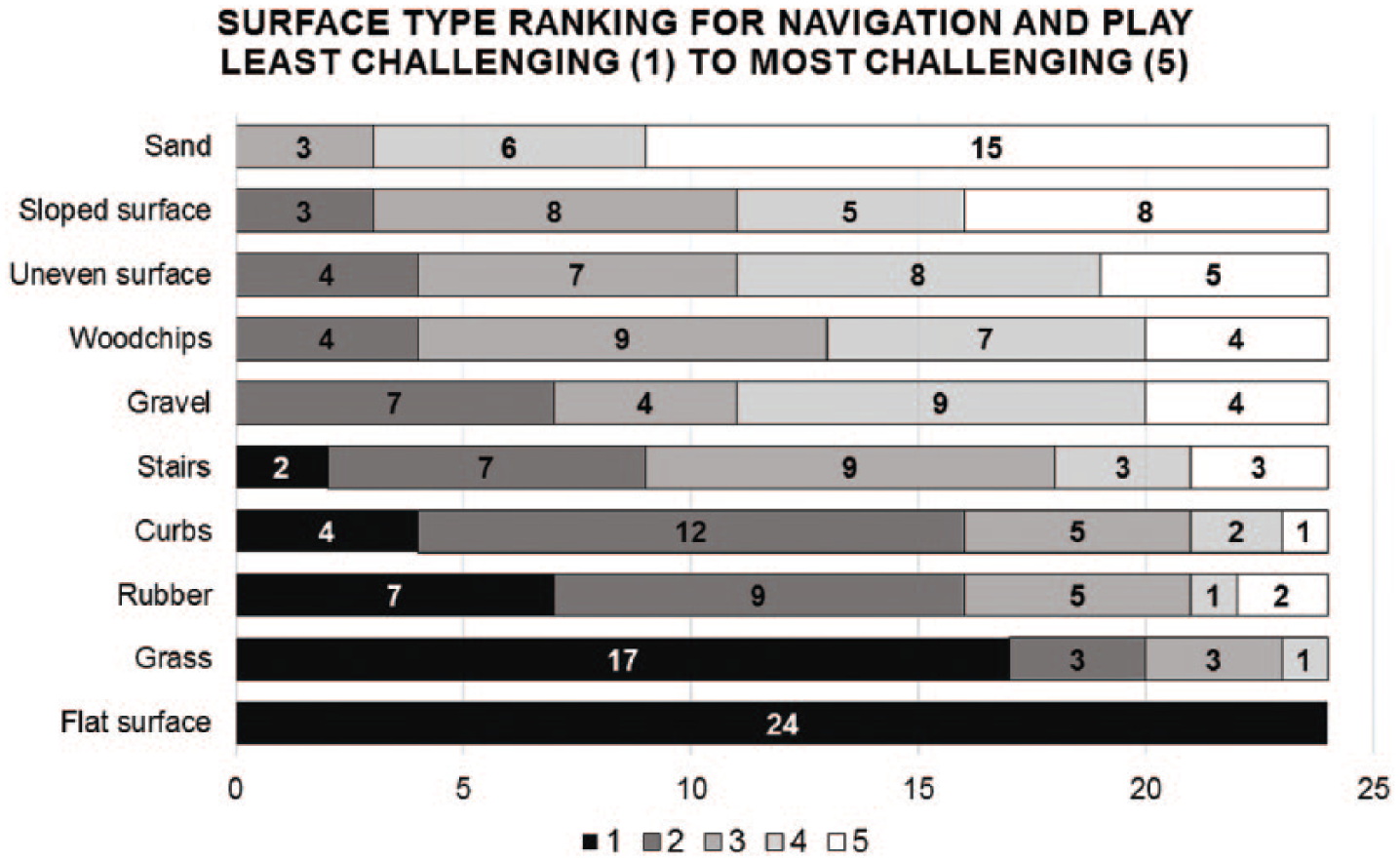
Surface type ranking (n = 24).
Comparison of children by level of function and age
Considering that children in the sample had different levels of amputations, numbers of limbs affected and spanned 6–12 years of age, trends by function level and age group were explored. We clustered our participants into three subgroups based on the expected level of function as derived from amputation level and type. These included (1) partial foot, through the ankle and below the knee (BK; n = 16), (2) through the knee and above the knee (AK; n = 4), and (3) bilateral/multilateral amputations (BA; n = 6). Data were categorical, so similarities and differences between frequencies of responses were evaluated. 25
In general, responses to questions about movement challenges were similar across levels of amputations. Some differences were noted with sitting cross legged or sitting on heels, which were the most difficult positions for 7 (44%) of the BK group, 4 (100%) of the AK group, and 4 (67%) of the BA group. In terms of fundamental movement skills, walking long distances were reported to be very challenging for 1 (6%), 4 (100%), and 6 (100%) children, respectively. When asked to rate environment-related playground surfaces, similar responses were noted (rated from 1, least challenging, to 5, most challenging) for wood chips averaged 3.4 for the BK group, 3.3 for the AK group, and 3.8 for the BA group. Uneven surfaces were rated on average 3.5, 3.5, and 3.8, respectively.
Like level of amputation, when comparing the youngest (age 6–7 years) to the oldest groups of children (age 11–12 years), similar positions, surfaces, activities, and fundamental movement skills were challenging. For example, parents reported that both younger and older had challenges with hopping, jumping, and skipping. There were no responses to questions that demonstrated a notable trend based on age.
Open-ended questions
Through the open-ended questions, parents reported several prosthetic-specific factors that influenced participation in active play. Parents stated (n = 3) that the child’s prosthetic leg would fall off when running, swinging, or playing kickball. Pain and bruising of the residual limb as well as prosthetic fit were also challenges (n = 3). In contrast, one parent wrote “When her leg is fitting properly, she does wonderfully and engages in almost any activity.” Tripping on the prosthesis was a problem mentioned by two parents. One parent stated that the prosthesis made the amputated side stick out further when sitting compared to the opposite side. Balance problems were described by one parent, especially in crowded areas, suggesting that more complex environments may impact mobility.
Less frequently, parents reported on activity, participation, and environmental factors. For example, two parents stated that participating in group activities was problematic because the prosthesis interfered with sitting on the floor. Three parents described concerns, avoidance, or worries about their child’s running speed compared with other children. Another parent commented about safety and risk-taking “… he will sometimes do activities that are too dangerous for him, or he cannot do, because everyone else is doing it.”
Discussion
This exploratory study is the first to describe participation in active play and play characteristics of children who use LEP. Our descriptive findings revealed that school-aged children who use LEP participated in a variety of play activities including active play, but they experienced barriers and challenges, including factors related to their prostheses that impacted their participation. Results offer preliminary insights into the specific types of play activities, fundamental movement skills, movement demands, and play environments that may pose difficulties and contribute to participation in active play challenges for children who use LEP.
Children who use LEP were reported to enjoy diverse types of age-appropriate play activities, including active outdoor play as well as sedentary activities. However, when asked about how their children moved in specific situations, parents noted difficulty with some play positions, transitions between positions and fundamental movement skills. They reported that certain types of play equipment, playground structures, and surfaces were harder to navigate. So, despite participation, over half of the parents of these school-aged children felt their child had difficulty keeping up with or performing at a comparable level with peers close in age.
Our findings that children with LEP engaged in and enjoyed diverse active play in indoor and outdoor environments, are consistent with a previous questionnaire study that reported children with LEP were very active participants in swimming, running, and bicycling activities. 25 In this study, specific activities parents reported as less frequently enjoyed by their children were those that require more skilled or complex movements (e.g. martial arts and dance). However, it is unclear from this questionnaire what specific factors contributed to less enjoyment or participation, or specific factors that supported participation (e.g. adaptive equipment).
Participation challenges could be impacted by many factors such as age of the child and developmental expectations, past and current medical conditions, limitations of the LEP, child interests, family resources, and environmental affordances, as all are possible influences on play outcomes. This study did not account for all of the factors that could collectively influence participation in active play, 20 and our small sample limited our capacity to systematically explore these relationships statistically. The multifaceted influences on participation in active play for children who use LEP warrant attention in future studies, specifically factors that enable participation (e.g. adaptive sport groups and other adaptations or resources) would be useful to understand.
The children in this sample shared common challenges, regardless of amputation level and age, and LEP use appears to impact participation in active play. Prosthetic factors were indeed highlighted by the respondents. When fit was optimal, there were fewer reported play barriers. However, prosthesis performance under different environmental conditions and with certain activity demands posed challenges. For example, parents reported it was harder for their children to play on uneven or sloped playground surfaces; sand was the most difficult surface to navigate. Also, children who used LEP did not seem to do as well with higher performance demands, such as speed, endurance, and coordination, required for more advanced movement activities. Play activities involving secure placement of the prosthetic foot, such as characteristic of skates, bikes, and ladders, were also challenging.
Parents reported that factors such as pain, tripping, and socket contact posed problems specific to children using LEP. In a previous adult study, pain, component failure, and tissue breakdown were reported as additional barriers to prosthetic use and mobility. 16 Findings collectively suggest that better prosthetic fit and design could reduce these barriers.
For children who use LEP, prosthetic engineering offers hope of regaining function that may improve their participation in active play. However, a recent prosthetic professional editorial discussed impediments to commercialization of children’s LEP. 26 Clearly, the limited market size presents a challenge to the cost of development and production. As a consequence, many children’s foot designs are small-sized adult feet that may not meet all the needs of children. For children with above knee amputations, choices in prosthetic components lag behind those available for adults. On the other hand, despite developmental differences, the concerns voiced by adults who use LEP in previous studies14,16 and the children’s challenges reported here mirror one another in many ways and indicate needed attention to LEP development in children.
The development of prostheses that have improved performance on a variety of surfaces, across and between postures, over longer time periods, in cramped spaces, on a variety of apparatus and equipment, under different gait types, and with limited cognitive effort will benefit people of all ages. Problem situations like keeping a prosthetic foot on a bicycle pedal have similarities to adult complaints of challenges riding motorcycles. Climbing ladders is problematic for some adults and children. However, hopping, skipping, jumping, and other distinctly childhood fundamental movement skills deserve their own attention and child-specific solutions. Versatility of prosthetic function across a child’s fundamental movement skills and play contexts was recommended in a recent professional magazine article. 26
While the development of versatile pediatric prostheses is important in the long run, reducing environmental barriers to participation in active play may help children who use LEP as well as other children with physical disabilities. Universal design solutions (e.g. playground surfaces) that maximize inclusive play opportunities for children with diverse needs and physical abilities are being implemented 27 to reduce barriers in the built play environment. 28 The barriers that emerged in this study suggest there may be specific design solutions that could meet the needs of children who use LEP. Another way to bypass environmental barriers and increase participation in active play is to access adapted sports, which are becoming more common and accepted for children who use LEP.
Mobility and postural challenges, faced by children who use LEP, inform the need to use more relevant outcome measures to account for the daily activity demands of children, compared to simple, straight-line, walking, and gait to measure the effectiveness of prosthetic design changes or other interventions. Parents of children who use LEP did not indicate that their children had challenges with playing on simple surfaces or moving forward or backward, suggesting that more complex, advanced movement skills might be the best skills to target and measure through performance indicators. Suggested outcomes could include standardized measures such as the Fundamental Movement Skills test (FMS) 29 and Pediatric Outcomes Data Collection Instrument (PODCI). 30 However, most standardized tests need to be validated for children who use LEP.
Fundamental motor skill development during the elementary school years provides an essential foundation for more complex actions that underpin lifetime participation in active play and these skills are correlated with cardiorespiratory fitness and inversely correlated with body weight status. 29 Thus, building fundamental movement skills can also reduce or prevent secondary problems that may stem from lack of or exclusion from active play. For example, children who do not have proficient movement skills due to motor impairments may stand out from peers and ultimately be excluded or choose to disengage from active play activities with peers. Perceived peer rejection and lower self-confidence in physical competence even for children without disabilities has been shown to contribute to a general decrease in physical activities. 31 As with other children with physical disabilities, over time this may result in children who use LEP engaging less in active play with increasing preferences for sedentary activities, increasing risks for secondary physical health consequences.
Teaching and building fundamental movement skills, particularly more complex and higher level skills, for children who use LEP is an important priority that could be facilitated in clinical, school, and/or community settings by a number of providers such as physical therapists, physical education teachers, or coaches. It would be important to consider factors such as child interests, available programs, and family resources when deciding on goals and methods of support. Opportunities to modify and practice these skills could help children who wear LEP feel more comfortable and willing to participate in physical activities with their peers.
While we explored questionnaire responses based on the level or presentation of the amputation, the conclusions that can be drawn about differences among these groups from these data are limited. The sample was heterogeneous and children had mixed presentations (e.g. unilateral, bilateral), thus it is possible that the questions were only able to identify the presence of a challenge, such as uneven ground, but were not able to differentiate the severity of the challenge. Thus, responses among children with different levels of amputation might be similar, even though the quality of performance would not.
It is also possible that some problems are present for most children with LEP, such as comfort at the prosthesis with residual limb interface, but we did not systematically inquire about fit or evaluate specific prosthetic technology, which would differ depending on the level of amputation. Children from different age groups, similar to levels of amputation, did not show marked differences in responses, possibly for the reasons noted above. This study suggests that future research should consider research methods and sampling that accounts for the heterogeneity of this group, so that the impact of factors such as age and level of amputation as well as other factors on active play participation can be examined systematically.
Study limitations include the small sample size, the use of a new questionnaire, and parent-report bias. The population of children with congenital, traumatic, or disease-associated amputation is small and heterogeneous, and therefore recruitment of parents to complete the questionnaire was challenging. This was a sample of convenience and the study sample size was small, hence the results have limited generalizability to other groups of children who use LEP. Respondents may also have different characteristics compared to nonrespondents in that children who were experiencing difficulties had parents who responded.
This preliminary study questionnaire was developed for exploratory purposes with the primary aim of understanding if participation in active play was a problem or not for this group. Also, to reduce participant burden the questionnaire is not inclusive of all aspects of childhood participation in active play. For example, information about the use of mobility aids during active play was not obtained. Refining the questionnaire as a valid and reliable child- and/or parent-reported measure of participation in active play for children with LEP would be an important goal for future research. Furthermore, parents were the respondents in this study; however, measuring the children’s own perceptions of their active play skills and experiences is essential to understand participation in active play.
Our exploratory results highlight the need for future research to understand more specifically what factors contribute to participation in active play challenges for children using LEP, and strategies to overcome these. In particular, more needs to be known about specific prosthetic components that facilitate or impede fundamental movement skills for active play, or interface with children’s play environments. Outcome measures need to more effectively capture the movement and participation demands of active play.
Conclusion
In conclusion, the majority of parents of children who use LEP reported that their children experienced play barriers that may stem from mobility limitations, the type of play activity, and characteristics of the built environment (i.e. surfaces, apparatus, and equipment), as well as concurrent challenges keeping up with their peers in schools and the community. Understanding challenges and barriers to participation in active play may result in prosthetic design improvements, rehabilitation, and other interventions that improve the quality of life for children who use LEP.
Supplemental Material
Supplementary Material
Supplemental material, OnlineAppendix_POI for Participation in active play of children who use lower extremity prostheses: An exploratory questionnaire by Cheryl Kerfeld, Tracy Jirikowic, Katheryn J Allyn and Murray E Maitland in Prosthetics and Orthotics International
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available Online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.