
Abstract
Aim
This study aimed to examine the factors influencing leisure walking intention among older adults in urban residential areas, analyze their interrelationships, and propose strategies for promoting walking activities.
Background
Understanding the factors influencing walking intentions among older adults is essential for developing interventions that enhance physical activity levels in an ageing society. A comprehensive approach that integrates psychological and environmental factors provides deeper insight into these influences.
Methods
Data were primarily obtained from older adults aged 60 years and older residing in five residential areas in Guilin, China, selected based on construction time, population density, available facilities, and aesthetic design. Participants were recruited through assistance from residential management. After excluding questionnaires with ineligible ages, excessively short completion times, or uniform responses, 527 valid questionnaires were retained. Data analysis was constructed using structural equation modeling, integrating the Theory of Planned Behavior and the Health Belief Model. Reliability and validity of the questionnaire were evaluated through Cronbach’s alpha, composite reliability, factor loadings and average variance extracted.
Results
The findings of this study revealed that among the factors influencing walking behavior intention, attitudes towards walking had the strongest positive effects. Perceived environmental barriers have a stronger negative impact on walking intention than perceived personal barriers.
Conclusions
Improving residential walking facilities to reduce environmental barriers and enhancing community health education to reinforce health beliefs are effective strategies for promoting physical activity among older adults. These findings provide practical guidance for urban planning and public health initiatives.
Keywords
Introduction
The global population aged 60 years old and above has exceeded one billion and is projected to reach two billion by 2050 (Navarro et al., 2024). Strain et al. (2024) reported that physical inactivity has risen among older adults, regardless of region or gender. Urban ageing presents additional challenges due to high population density and limited public space that can further restrict physical activity. Addressing the health and well-being of older adults is an urgent priority for ageing societies, and walking is widely recognized as one of the most accessible and effective forms of physical activity for this population (Nicklas et al., 2020). Among various walking types, leisure walking refers to walking undertaken for enjoyment, relaxation, or health promotion, rather than for transportation or shopping purposes, which characterize utilitarian walking. It also fosters social interactions and enhances overall wellbeing, underscoring its vital role in promoting healthy ageing (Ungvari et al., 2023).
Despite these benefits, cultivating regular walking habits among older adults remains challenging. Most older adults prefer to age in place, choosing to remain in their own homes and communities as they grow older (Lewis & Buffel, 2020). Therefore, urban residential environments play a crucial role in shaping their walking behavior, as factors like infrastructure quality and traffic safety influence both their motivation and ability to walk. Research has shown that walking intentions are influenced by a combination of psychological, social, and environmental factors (Moghetti et al., 2020; Tong & Maliki, 2024). However, previous studies often examine these factors in isolation. Some emphasize the benefits of walkability, green spaces, and pedestrian infrastructure (Kim et al., 2024; Nwana et al., 2024), while others have highlighted barriers such as poor lighting, uneven pathways, and insufficient resting areas (O’Meara et al., 2024). Similarly, research has suggested that perceived health risks and benefits influence walking participation (Kaushal et al., 2021). Nevertheless, few studies have explored the combined effects of health beliefs and environmental barriers on walking behavior.
This study integrates two widely used theories: The Health Belief Model and the Theory of Planned Behavior. These two theories are extensively applied in health behavior research and hold significant value in predicting walking intentions. The Health Belief Model emphasizes how individual health beliefs shape behavioral intentions (Karl et al., 2022). Meanwhile, the Theory of Planned Behavior explains behavior through cognitive assessments of the social environment and behavioral capabilities (Ajzen, 1991; Stehr et al., 2021). Although both contribute to understanding walking intentions, they differ in their explanatory focus. The Health Belief Model accounts for the role of health beliefs in shaping behavior; however, it overlooks the cognitive dimensions influenced by social norms and environmental factors (Alyafei & Easton-Carr, 2024). Conversely, the Theory of Planned Behavior excels in predicting behavioral intentions but does not sufficiently incorporate health beliefs as motivators. Thus, integrating these two models allows them to complement each other. Furthermore, both theories overlook the impact of the physical environment on walking behavior (Pedersen et al., 2022; Rehn et al., 2022). To address these gaps, this study integrates the Health Belief Model and Theory of Planned Behavior while incorporating perceived environmental barriers as an external environmental factor. The measured environmental barriers include surface evenness, availability of resting facilities, trail connectivity, richness of natural landscapes, and environmental maintenance.
This integrated framework positions the functions of the Health Belief Model as potential antecedents to the Theory of Planned Behavior, emphasizing that the cognitive components from the Theory of Planned Behavior (attitude, subjective norms, and perceived behavioral control) are influenced by personal barriers, health motivation from the Health Belief Model, and external physical environmental factors. This integration strengthens the role of health beliefs and environmental influences in shaping behavioral intentions, thereby addressing the limitations of the Theory of Planned Behavior in capturing intrinsic health motivation. This establishes a more comprehensive and structured framework. The findings may guide urban planners and public health professionals to promote physical activity among older adults by improving built environments, strengthening social support, and enhancing community health awareness. To examine the relationships among the factors influencing the walking intentions of older adults, this study proposes the following research questions: (1) How do cognitive components from the Theory of Planned Behavior influence older adults’ leisure walking intentions? (2) How does health motivation affect cognitive components in older adults? and (3) How do perceived personal and residential environmental barriers separately influence cognitive components and leisure walking intention among older adults?
Literature Review
This section examines past studies, research models, and hypotheses regarding the recreational walking intentions of older adults in residential areas.
Leisure Walking Activities Among Older Adults
Engaging in moderate-intensity walking for 50–60 min, three times a week has been shown to significantly enhance the health of older adults (Hu & Wu, 2016; Yu et al., 2022). As shown in Table 1, walking can be classified into utilitarian and leisure walking. Leisure walking is distinct from utilitarian walking as it focuses on enjoyment, relaxation, or exercise in pleasant environments, rather than goal-directed activities such as commuting or shopping. Compared to utilitarian walking, leisure walking typically involves longer durations, lower frequencies, slower speeds, and is influenced more by aesthetic and recreational factors (Kang et al., 2017; Zurawik, 2020). This distinction is particularly important for older adults, as leisure walking offers opportunities for low-intensity, self-paced physical activity in supportive environments, which is essential for those experiencing mobility limitations or lacking access to structured exercise programs. Moreover, environmental factors significantly influence older adults’ ability and motivation to engage in leisure walking.
Classification of Walking.

Adopted from Kang et al. (2017); Zurawik (2020).
Role of Residential Environment in Leisure Walking
Several studies conducted in the United States, the Netherlands, Japan, and China have indicated that most older adults prefer to “age in place,” choosing to spend their later years in familiar residential settings to maintain their independence and sense of familiarity (Annink & Van Hees, 2023; Nakagawa et al., 2022; Ratnayake et al., 2022). In this context, the residential environment serves as the physical foundation for sustained leisure walking among older adults. However, environmental barriers can significantly constrain walking behaviors. In Tel Aviv, deteriorated sidewalks intensified older adults’ fear of falling, consequently limiting their outdoor mobility (Plaut et al., 2021). In Singapore, poor lighting and inadequate shelter diminished perceived safety and comfort, discouraging participation in walking activities (Močnik et al., 2022). Similarly, the absence of shaded walkways and resting areas in Finland contributed to greater physical fatigue, reducing both the frequency and duration of leisure walking (Tuomola et al., 2024).
Existing Research and Theoretical Gaps
This study conducted a literature search using Web of Science and Scopus, focusing on studies published between 2016 and 2024. Filters were applied to include only peer-reviewed journal articles. The search terms used were “Theory of Planned Behavior,” “Health Belief Model,” “behavioral intention,” “physical environment,” and “older adults.” To better understand the relationships among these variables, we prioritized empirical studies that examined multiple relevant factors. Table 2 provides a summary of studies from different countries investigating behavioral intentions in older adults, including sample characteristics, validated and rejected hypotheses, explanatory power, and theoretical frameworks applied.
Studies on Behavioral Intentions in Older Adults.

AT: attitudes; BI: behavioral intention; HBM: health belief model; IBC: integrated behavior change model; PT: perceived threats; PB: perceived benefits; PPB: perceived personal barriers; PEB: perceived environmental barriers; PN: perceived norms; PC: perceived control; SDM: self-determination theory; TPB: theory of planned behavior.
It shows only the hypotheses established with the variables included in the current study.
The Theory of Planned Behavior lacks consideration of health perception, while the Health Belief Model, despite its extensive application in disease prevention, places limited emphasis on social and environmental factors. Furthermore, existing studies have primarily examined the formation of short-term behavioral intentions, with limited focus on the maintenance of long-term health behavior intentions. The residential environment serves as a crucial physical foundation for long-term activities, and its interaction with psychological health factors may influence the persistence of long-term behaviors (Cheung, 2024; Su & Zhou, 2022). Therefore, this study integrates these two theories with environmental barriers to better understand the reciprocal relationship between health beliefs and environmental factors in shaping long-term behavioral intentions.
Development of Theoretical Framework
This study integrates the Health Belief Model and the Theory of Planned Behavior to establish a structural theoretical framework, drawing on their shared features (Hossain et al., 2021).
The Theory of Planned Behavior
The Theory of Planned Behavior, proposed by Ajzen (1985), explains behavioral intention through three determinants: attitude, subjective norms, and perceived behavioral control. These factors collectively shape intentions, which in turn serve as predictors of actual behavior. The Theory of Planned Behavior has been widely recognized for its effectiveness in explaining behaviors, including walking. Among older adults, walking behavior is strongly influenced by attitude and perceived control (Stehr et al., 2021).
The Health Belief Model
Rosenstock (1966) proposed the Health Belief Model in the 1950s to explain why individuals choose not to engage in public health services. Subsequent studies have demonstrated its effectiveness in predicting health behaviors (Karl et al., 2022; Liao et al., 2024). Over time, the Health Belief Model expanded to include six key constructs: Perceived susceptibility (the perceived likelihood of experiencing negative outcomes without health behavior), perceived severity (the perceived seriousness of the consequences of failing to adopt health behaviors), perceived benefits (the potential advantages of engaging in health behaviors), perceived barriers (the obstacles or challenges that may hinder participation in health behaviors), action cues (factors that prompt individuals to engage in healthy behaviors), and self-efficacy (an individual's confidence in their ability to perform and maintain specific health behaviors).
Perceived Environmental Barriers Factor
Perceived environmental barriers are incorporated into this study as physical environmental factors to enhance the explanatory power of the model. Unlike internal psychological factors such as perceived personal barriers or perceived behavioral control, perceived environmental barriers refer to objective external conditions. These include factors like unsafe sidewalks and poor connectivity, which are typically beyond individual control (Lima et al., 2024; Soto et al., 2022). Empirical studies have shown that such unfavorable environments not only constrain perceived behavioral control but also negatively affect walking attitudes and behavioral intentions (Pedersen et al., 2022; Wee et al., 2019). Therefore, conceptualizing environmental barriers as an independent external factor allows for a more comprehensive understanding of the multifaceted influence of the physical environment on walking intentions among older adults.
Extended Theory of Planned Behavior and Health Belief Model
This study extends the Theory of Planned Behavior by integrating elements from the Health Belief Model. The integrated theoretical framework retains the three major factors from the original Theory of Planned Behavior. Perceived susceptibility and severity from the Health Belief Model were combined into perceived threats (Kaushal et al., 2020). Both perceived threats and benefits are classified as health motivations, while perceived personal barriers are retained as independent factors (Akram, 2024).
Building on this integration, the remaining constructs from the Health Belief Model are embedded within key components of the Theory of Planned Behavior. Action cues are internal or external triggers for health behavior, such as physician recommendations, media messages, or reminders from family members. Subjective norms from the Theory of Planned Behavior refer to perceived expectations from significant others. Therefore, action cues are often concrete expressions of these subjective norms. For example, a doctor’ s recommendation may function not only as a behavioral prompt but also as an implicit expectation rooted in medical authority (Prusiński, 2022). Similarly, repeated advice from family members may reflect perceived behavioral norms within the household (Thomas & Hovick, 2021). Therefore, in this study, action cues are incorporated into the structure of subjective norms. Likewise, self-efficacy refers to confidence in one’ s ability to perform a specific behavior (Kaushal et al., 2020). It shares conceptual relevance with perceived behavioral control and is integrated into the structure of that construct.
As illustrated in Figure 1, the theoretical framework illustrates the structural characteristics of the extended model. The Health Belief Model explains behavior through two key components: Personal barriers and perceived health motivation, both of which influence attitudes and perceived behavioral control in the Theory of Planned Behavior (Qiao et al., 2021). Additionally, the physical environment is incorporated as an external factor that influences attitudes, subjective norms, and perceived behavioral control within the Theory of Planned Behavior, ultimately shaping behavioral intentions (Jiang et al., 2022; Ritchie et al., 2020). Furthermore, both perceived personal barriers and environmental factors directly influence behavioral intentions, highlighting the interaction between internal psychological determinants and external environmental influences (Gabriel et al., 2019).

Theoretical Framework.
Methods
This study employed an empirical approach, using quantitative and survey methods to collect data through a structured questionnaire, which was analyzed using structural equation modeling (SEM). The questionnaire utilizes a 5-point Likert scale (Likert, 1932), and included items based on eight core variables, as well as demographic information. The scales are listed in Supplemental Materials, Table A1. In this research model, the outcome variable (dependent variable) was behavioral intention. The independent variables included perceived health threats, perceived benefits of walking, perceived personal barriers, and perceived environmental barriers, which acted as predictors of the other variables. The mediating variables included attitudes toward walking, perceived walking norms, and perceived walking control. These mediators established a connection between the independent and outcome variables.
Hypotheses Formulation
First, we proposed several hypotheses to examine the role of cognitive components (attitude, perceived norms, and perceived behavioral control) on leisure walking intention among older adults. Studies indicate that positive attitudes, such as the belief that walking enhances well-being, significantly improve behavioral intention (Harada et al., 2023; Shaffer, 2021). Perceived norms, particularly in urban settings where walking is encouraged through urban planning and community policies, exert a substantial influence on behavioral intentions (Moreira, Andrade et al., 2020; Tong & Maliki, 2024). Additionally, perceived behavioral control, which reflects an individual's sense of autonomy and capability in regulating their walking behavior, has been positively linked to behavioral intentions (Ng et al., 2022). Therefore, this study hypothesizes that attitudes toward walking (H1), perceived norms (H2), and perceived walking control (H3) all have a positive effect on behavioral intention.
Second, we formulated several hypotheses to examine the influence of health motivation on cognitive components in older adults. Perceived health threats, such as awareness of the risks of chronic diseases and sleep disturbances caused by insufficient physical activity play a crucial role in shaping individuals’ attitudes (Blackwood et al., 2021). Similarly, the perceived benefits of walking, such as its potential to improve physical health, enhance mental well-being, and foster social interaction, can strengthen attitudes toward walking and behavioral intentions (Leung et al., 2021). Hence, perceived health threats (H4) and perceived benefits of walking (H5) had a positive effect on attitudes toward walking.
Third, we proposed hypotheses to investigate the impact of perceived personal and residential environmental barriers on cognitive components and leisure walking intentions among older adults. Perceived personal barriers, such as fear of injury, lack of motivation, and joint pain, can negatively impact attitudes toward walking, behavioral intention, and perceived control (Leung et al., 2021; Richards & Woodcox, 2021). Therefore, this study suggests that perceived personal barriers are negatively related to attitudes towards walking (H6a), behavioral intentions (H6b), and perceived walking control (H6c). Perceived environmental barriers, such as uneven roads, poor lighting, and a lack of walking infrastructure, can weaken attitudes toward walking, reduce the perception of supportive norms, and diminish perceived control, lowering walking intentions (Castillo-Paredes et al., 2021; Omura et al., 2020; Soto et al., 2023). Therefore, this study proposes that perceived environmental barriers are negatively related to attitudes toward walking (H7a), perceived norms of walking (H7b), perceived walking control (H7c), and behavioral intention (H7d). The conceptual framework in Figure 2 illustrates the relationships among these variables.

Conceptual model.
Data Collection and Sampling Selection
This study employed convenience sampling, primarily targeting individuals aged 60 years and older. However, individuals aged 50 and above were also included, considering that chronic disease prevalence and physical activity patterns begin to change at this stage (Ghanem et al., 2023; Gil-Salcedo et al., 2020). The sample population was drawn from five representative residential areas in Guilin, China (as shown in Figures 3 and 4). The selection of these areas was based on construction time, population size, residential facilities, and aesthetic design (as detailed in Table 3). The construction time reflects the characteristics of different stages of urban development (Hu et al., 2024), ranging from areas with incomplete infrastructure to fully developed residential environments. Considering the sample size, each residential area selected consisted of more than 500 households. Residential facilities range from limited amenities to modern developments featuring leisure trails, green spaces, and recreational zones (Hao & Ma 2022; Jiang et al. 2023). Aesthetic design emphasizes visual appeal and its impact on the walking experiences of older adults (Najafi & Mohammadi, 2024). These characteristics ensure the diversity and relevance of the selected areas, with the final selection also considering the support of property staff and homeowners’ committees.

Location map of the five residential areas in Guilin City. Source. Sketched by the author, original photo taken from Baidu Maps.

The plans of the five residential areas. Source. Sketched by the author, original photo taken from Google Maps.
Characteristics of the Five Residential Areas.

Electronic surveys were distributed using SoJump’ s QR code technology to quickly achieve a sufficient sample size. According to the number of households in each residential area proportionally, 600 samples were collected. With the assistance of property management staff, we randomly selected target residents, primarily those aged 60 years and older, and distributed electronic survey links to them. Participants had the option to complete the survey online independently. Older adults who required assistance could either seek help from their family members or visit the property management office for volunteer support. To enhance the efficiency of survey collection, we enlisted the support of homeowners’ committees, who distributed QR code survey links in residential WeChat groups. Given the large number of participants in these groups, this strategy significantly improved survey distribution efficiency. Through this multi-layered recruitment approach, we successfully collected all responses. All survey participants received incentives for their participation. Residents who completed the survey could enter a lucky draw held at the property management office, with prizes such as tissue packs, pens, towels, and foldable shopping bags provided by the research team. Property management staff and assisting individuals received a thank-you package consisting of a supermarket gift card and practical items, including a reusable shopping bag and a portable water bottle. Following data collection, we applied exclusion criteria to ensure data quality, including incomplete surveys, uniform responses across items, submission times under 180 s, and ineligible age. After filtering for valid responses, a final dataset of 527 valid responses was retained for analysis.
Data Analysis
SEM was conducted in two stages to test the proposed hypotheses and validate the conceptual model. First, the scales were evaluated to ensure reliability and validity of the constructs. The psychometric reliability of the scales was evaluated based on Cronbach’ s alpha (CA) and composite reliability (CR), with values above 0.70 considered acceptable (Thompson et al., 1995). This step ensured that key constructs, including health motivation (perceived threats and benefits), perceived personal barriers, perceived environmental barriers, attitudes, perceived norms, and perceived behavioral control demonstrated strong internal consistency. To establish convergent validity of the scales, factor loadings (≥0.5) and average variance extracted (AVE, ≥0.5) were examined to ensure that latent variables were accurately represented by their indicators. Discriminant validity was determined using the Fornell–Larcker criterion, ensuring that the maximum shared variance (MSV) of each construct was lower than its AVE. This verification ensured a clear distinction among health beliefs, cognitive components, and environmental barriers within the scale structure, further strengthening the validity of the theoretical model.
Harman's single-factor test was conducted to control for common method bias, ensuring that measurement artifacts did not artificially inflate relationships. Given the study's integration of two theories, this validation process ensured a rigorous measurement of how health motivation, personal and environmental barriers, and cognitive components interacted to shape behavioral intentions in residential settings.
Furthermore, to ensure the statistical validity of the hypothesized pathways, model fit was evaluated using these key indices. Fit indices, including the comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and goodness of fit index (GFI), determined whether the model aligned with the observed data (Hair et al., 2010).
In the second stage, the structural model was analyzed. Path analysis was first conducted to test the hypothesized relationships among constructs. Specifically, a hypothesized relationship was considered supported if the standardized path coefficient was statistically significant (p < 0.05), the critical ratio (C.R.) exceeded ±1.96, and the effect was in the hypothesized direction. The magnitude of the path coefficient reflected the strength of the relationship between constructs. The model's explanatory power was determined by the determination coefficient (R²), which ranges from 0 to 1, indicated acceptable predictive accuracy when R² exceeded 0.10 (Hair et al. 2010). To test the mediating effects of cognitive factors, the bootstrap method with 5000 resamples was employed by applying a maximum likelihood estimation for model fitting (Preacher et al., 2007). This approach, combined with Bias-corrected and Percentile methods at a 95% confidence interval was employed to determine whether cognitive factors from the Theory of Planned Behavior mediated the relationships between health beliefs, environmental barriers, and behavioral intention. Mediation effects were considered significant if the confidence interval excluded zero and the p-values fell below 0.05 (Zhonglin et al., 2004). This analysis ensured a rigorous examination of indirect pathways, clarifying how cognitive components translated external influences into behavioral intentions. This systematic approach provided robust and comprehensive insights into the relationships within the research model.
Results
The sociodemographic characteristics of the participants are presented in Table 4. Most respondents (71.73%) were aged between 60 and 70 years, and 68.50% reported having chronic diseases. According to the World Health Organization, older adults should engage in 150–300 min of moderate-intensity aerobic physical activity per week to promote healthy ageing (Bull et al., 2020). In this sample, 81.59% of respondents reported walking twice or less per week, and 84.82% walked for 45 min or less per session. Thus, more than 80% of older adults do not meet the recommended walking levels for health benefits. Additionally, 76.47% reported walking at a slow pace, and 37.76% had a relatively low monthly income. These findings highlight the limited health awareness, low walking intensity, and a high prevalence of chronic diseases among older adults. Understanding these trends provides valuable insights into the relationship between health status, physical activity patterns, and demographics factors in this population.
Demographic Characteristics of the Participants.

More than 80% of older adults do not meet the recommended walking levels for health benefits.
Measurement Model
Given that all items in each questionnaire were completed by individual respondents, Harman's single-factor test was conducted beforehand to check for common method bias. Exploratory factor analysis using SPSS 26.0, extracted four factors with eigenvalues greater than 1 from all scale items. The first factor explained 25.278% of the variance, which was below the critical threshold of 40%, indicating no serious common method bias. Therefore, the questionnaire data were reliable and appropriate for further analysis.
To develop the measurement model, internal consistency, convergent validity, and discriminant validity of the scales were assessed. First, as shown in Table 5, internal consistency was confirmed as all CA and CR values exceeded 0.7, indicating strong reliability and stability across the scales (Thompson et al., 1995). This confirms that the measurement model effectively represents health beliefs (perceived health threats, perceived benefits of walking, and personal environmental barriers), cognitive components (attitudes towards walking, perceived norms of walking, and perceived walking control), and perceived environmental barriers as distinct but interrelated constructs. Second, convergent validity was achieved as factor loadings ranged from 0.672 to 0.825 and AVE values ranged from 0.506 to 0.656, both exceeding 0.5 (Hair et al., 2010). Table 5 confirms that the scales and the item design of the model were scientifically sound and accurately reflected the core characteristics of each latent variable. Third, discriminant validity was also established as the MSV for all latent variables remained lower than their respective AVE values, with no cross-loadings among the factors (as detailed in Table 6) (Hair et al., 2010). This confirms that each construct of the scales is empirically distinct and conceptually sound, ensuring the integrity of the model and preventing redundancy among the variables within the theoretical framework.
Convergent Validity and Reliability.
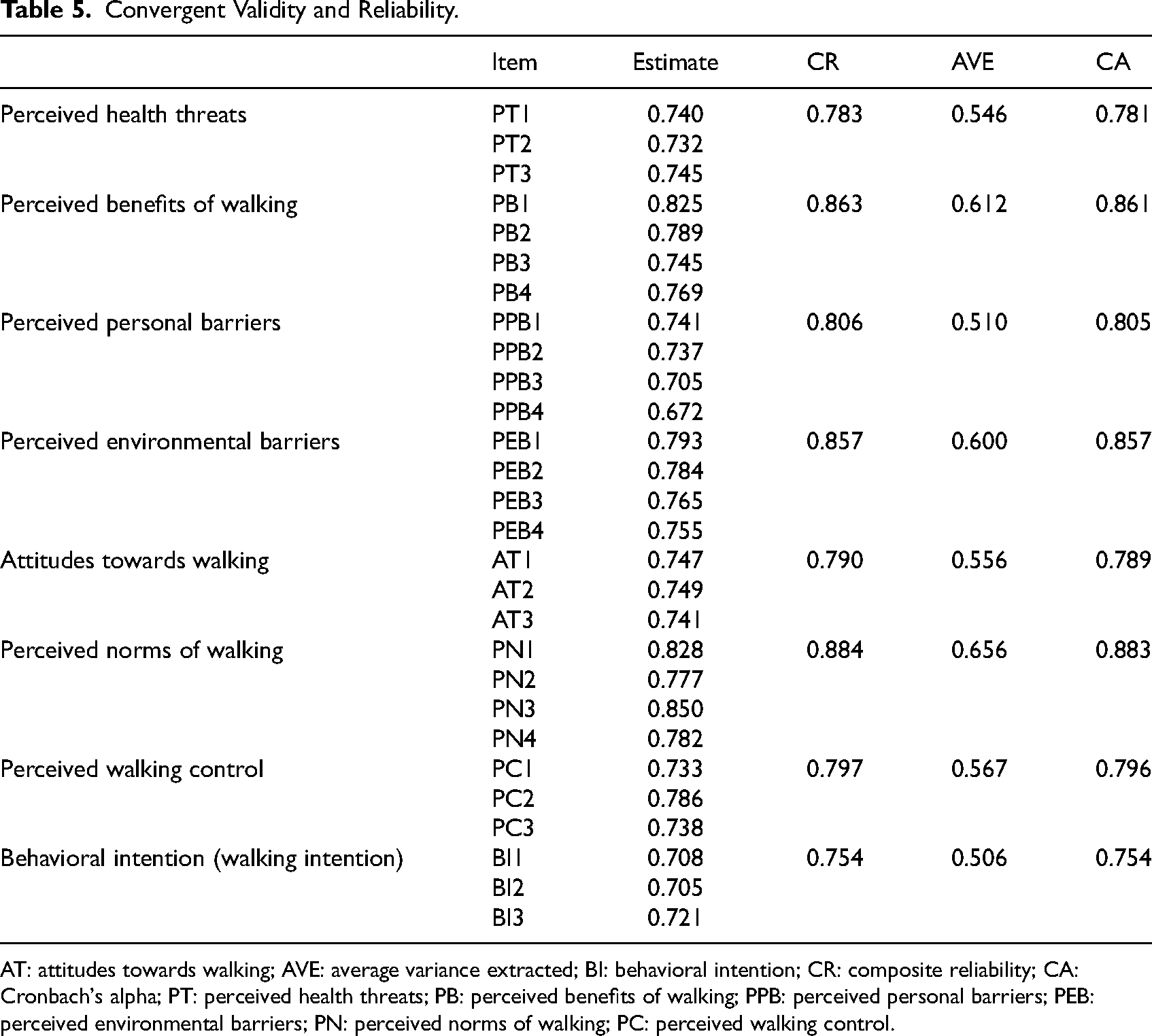
AT: attitudes towards walking; AVE: average variance extracted; BI: behavioral intention; CR: composite reliability; CA: Cronbach's alpha; PT: perceived health threats; PB: perceived benefits of walking; PPB: perceived personal barriers; PEB: perceived environmental barriers; PN: perceived norms of walking; PC: perceived walking control.
Discriminant Validity.

AT: attitudes towards walking; AVE: average variance extracted; BI: behavioral intention; PT: perceived health threats; PB: perceived benefits of walking; PPB: perceived personal barriers; PEB: perceived environmental barriers; PN: perceived norms of walking; PC: perceived walking control.
*Indicates significance level: *0.01 ≤ p < 0.05, **0.001 ≤ p < 0.01, ***p < 0.001; values on the diagonal indicate the square roots of the AVE.
The model fit was evaluated using various indices based on good convergent and discriminant validity results. Table 7 shows that the model exhibited a good fit, with CFI (0.978), TLI (0.975), RMSEA (0.027), and GFI (0.941) exceeding the recommended thresholds (Hair et al., 2010). This supports the robustness of the integrated framework, ensuring that cognitive components, health belief, and environmental barriers collectively and accurately explain walking intentions among older adults. These results reinforce the theoretical and empirical validity of the study.
Model Fit.

CFI: comparative fit index; GFI: goodness of fit index; IFI: incremental fit index; NFI: normed fit index; RMSEA: root mean square error of approximation; TLI: Tucker–Lewis index; χ2/df: Chi-square divided by degrees of freedom.
Structural Model
A structural model was evaluated to determine causal relationships between the proposed structures. The results of the hypothesis testing are shown in Figure 5 and Table 8. Hypothesis H6a was rejected, while the others (H1, H2, H3, H4, H5, H6b, H6c, H7a, H7b, H7c, and H7d) were supported. The R² value for behavioral intention was 0.41, indicating that the model captures a substantial portion of the factors influencing older adults’ leisure walking decisions, aligning well with the study's research objective.

Structural model results.
Structural Path Coefficients.

AT: attitudes towards walking; BI: behavioral intention; C.R. : critical ratio; DV: dependent variable; PT: perceived health threats; PB: perceived benefits of walking; PPB: perceived personal barriers; PEB: perceived environmental barriers; PN: perceived norms of walking; PC: perceived walking control; P: P-value; R²: coefficient of determination, reported once per dependent variable to avoid redundancy; S.E. : standard error.
*Indicates significance level: *0.01 ≤ p < 0.05, **0.001 ≤ p < 0.01, ***p < 0.001.
Table 8 also presents the significance of relationships, standardized path coefficients, standard errors, and C.R.s. Among the exogenous latent variables, perceived environmental barriers were the most crucial determinants of behavioral intention, with a standardized effect of 0.199, followed by perceived personal barriers, with a standardized effect of 0.183. Additionally, perceived environmental barriers played a crucial role in shaping the cognitive structure based on the Theory of Planned Behavior, with the most decisive impact on perceived norms of walking, reflected by a path coefficient of 0.339. This reinforces the importance of the physical environment in shaping walking behavior and directly answers the third research question by exploring how physical environmental factors influence cognitive components and walking intention. Among the exogenous latent variables, perceived environmental barriers were the most crucial determinant of walking behavioral intention.
Hypothesis H6a was rejected, indicating that perceived personal barriers do not influence attitudes toward walking but significantly affect perceived walking control. This distinction clarifies the role of personal barriers in the cognitive structure. This contrast strengthens the theoretical structure of this study, indicating that personal barriers primarily affect perceived walking control, while perceived environmental factors simultaneously influence attitudes towards walking, perceived norms of walking, and perceived walking control within the cognitive structure. This finding further answers the third research question regarding how perceived personal and environmental barriers influence cognitive components based on the Theory of Planned Behavior.
The results also showed that within the cognitive components of the Theory of Planned Behavior, attitudes toward walking were the strongest determinant of behavioral intention, with a standardized effect of 0.239. Together with previous findings, these results further confirm that attitudes are the most significant predictor of walking intention. These findings address the first research question and confirm the importance of cognitive components based on the Theory of Planned Behavior in predicting walking intention among older adults.
According to the data in Table 8, the strongest factors influencing attitudes toward walking were the perceived health threats and benefits of walking, with path coefficients of 0.229 and 0.192, respectively. The perceived health threats and benefits of walking fall under health motivation, which addresses the second research question regarding how health motivation influences cognitive components from the Theory of Planned Behavior.
The results of the mediation effect tests are presented in Table 9. Most of the mediation effects were significant, except for the mediation effect of perceived personal barriers on behavioral intention through attitudes towards walking, which was not supported due to a p-value above 0.05 and a confidence interval that included zero (Zhonglin et al., 2004). These findings further explain the second research question. The results indicate that health motivation has a positive impact on attitudes toward walking, functioning as a mediating variable and significantly predicting walking intention. According to the results in Table 9, perceived personal barriers do not influence walking intention through perceived walking attitudes, further supporting the notion that walking attitudes are primarily shaped by health motivation rather than perceived personal barriers.
Mediation Effects.

AT: attitudes towards walking; BI: behavioral intention; CI: confidence interval; PT: perceived health threats; PB: perceived benefits of walking; PPB: perceived personal barriers; PEB: perceived environmental barriers; PN: perceived norms of walking; PC: perceived walking control; P: P-value.
*Indicates significance level: *0.01 ≤ p < 0.05, **0.001 ≤ p < 0.01, *** p < 0.001.
Discussion and Conclusions
Over 80% of the participants reported insufficient walking activity, highlighting the widespread lack of physical activity among older adults, which is consistent with previous studies (Moreira, Filho et al., 2020). This represents a significant public health concern, as a large proportion of older adults fail to meet the recommended physical activity levels, increasing the risk of chronic conditions such as cardiovascular disease, diabetes, and mental health decline (Makino et al., 2022; Van Zutphen et al., 2021). These results underscore the need for targeted interventions to increase walking activity in this population. The findings of this study indicate that attitudes toward walking are the strongest predictor and determinant of behavioral intentions.
The structural model results and hypothesis testing confirmed that the cognitive components based on the Theory of Planned Behavior directly influences walking intention. The findings of this study indicate that attitudes toward walking are the strongest predictor and determinant of behavioral intentions (R² = 0.21; path coefficient = 0.239). These results highlight the crucial role of attitudes within the cognitive structure of the Theory of Planned Behavior in promoting walking intention among older adults, aligning with the findings of previous studies (La Barbera & Ajzen, 2024; Stehr et al., 2021). The practical implication of this finding is that interventions aimed at promoting walking among older adults should focus on fostering positive attitudes toward walking. This includes exploring methods to create engaging and enjoyable walking experiences that evoke positive emotional responses. The practical implication of this finding is that interventions aimed at promoting walking among older adults should focus on fostering positive attitudes toward walking. This includes exploring methods to create engaging and enjoyable walking experiences that evoke positive emotional responses.
Unlike previous studies that treat the Theory of Planned Behavior structure as exogenous variables (Liu et al., 2022; Mandal et al., 2023), this study positions it as a cognitive structure to mediate health beliefs and perceived environmental barriers, thereby enhancing the applicability. The structural model and hypothesis testing results not only confirm that attitudes are the most important cognitive mediators influencing walking intention, but also indicate that health motivation (including perceived health threats with a path coefficient of 0.229 and perceived benefits of walking with a path coefficient of 0.192) is the most significant determinant of attitudes. This finding is consistent with previous studies, in which it is believed that the benefits of walking outweigh personal barriers (Kadir et al., 2019; Liliana et al., 2020). To effectively change walking attitudes among older adults, interventions should focus on increasing awareness of the health risks associated with physical inactivity. Community health seminars and interactive workshops can educate older adults about the negative effects of inactivity, while highlighting the health benefits of regular physical activity. Health risk assessments can help individuals better understand their health status, further increasing their awareness of potential threats. Additionally, health management applications that provide personalized health insights can keep older adults informed and motivated, improve their attitudes, and increase their walking intentions.
The results showed that among the exogenous latent variables, perceived environmental barriers were a more significant determinant of behavioral intention than perceived personal barriers, with a path coefficient of 0.199. This emphasizes the critical role of physical environmental factors in health behavior decisions, especially when integrated with the Health Belief Model. Previous studies primarily focused on internal physical or psychological limitations, overlooking the impact of external environmental factors (Khodaveisi et al., 2021; Kim et al., 2023). Specifically, the direct influence of perceived environmental barriers on walking intention underlines the importance of environmental factors in promoting health behaviors. These findings suggest that interventions should focus on improving the physical environment, such as sidewalk design, traffic safety, and public facilities, to remove barriers and encourage active walking among older adults. Future studies should investigate the relative importance of various environmental factors in different populations.
Furthermore, this study also confirms how perceived personal and environmental barriers jointly shape cognitive processes based on the Theory of Planned Behavior. Perceived environmental barriers had the greatest influence on perceived walking norms (path coefficient = 0.339), while perceived personal barriers primarily determined perceived behavioral control. This study suggests that when individuals perceive their walking environment as unsafe or unfriendly, they may feel that walking lacks social support. Additionally, their judgment of whether they can overcome personal barriers influences their belief in their ability to walk. Unlike previous studies that focused solely on personal barriers (Aliyas, 2019; Bentley & Kelechi, 2018), this study highlights the complementary role of the environment in shaping the perceptions of social norms. In practice, policymakers can improve walking environments by increasing social support for walking, such as by adding signage and encouraging initiatives. Interventions should also help individuals recognize their walking abilities and overcome personal barriers. Future studies should explore how different types of environmental barriers affect walking intentions.
The rejected hypothesis (H6a) posited that perceived personal barriers do not negatively affect attitudes towards walking. This contradicts previous findings (Batten et al., 2020; Jones et al., 2023). This finding suggests that older adults’ attitudes towards walking are shaped more by health motivations and environmental quality than by personal barriers. Despite physical challenges, many older adults remain positive, motivated by a desire to improve their health, engage in social interactions, and enjoy the outdoors. This underscores the importance of interventions that extends beyond addressing physical and psychological barriers and focus on health awareness and environmental improvements. Policymakers and health professionals should encourage walking by creating safe, accessible outdoor spaces and providing convenient facilities. Future studies should explore how external facilities interact with personal barriers to encourage physical activity among older adults.
Overall, our study highlights the long-term interplay between health beliefs and environmental factors. Additionally, our model explained 41% of the variance in leisure walking intentions, demonstrating strong explanatory and predictive power. Future research should explore strategies to enhance health education, strengthen awareness, and improve residential environments to reduce these barriers.
Limitations and Future Research
This study has certain limitations. First, the sample size of participants aged 70 years and older was relatively small, likely due to their limited availability and willingness to participate, potentially leading to insufficient representation of this age group. Second, the reliance on electronic surveys in this study may have introduced selection bias, as older adults with limited digital literacy could have been underrepresented. Third, as this was a single-city study, the findings may have been influenced by the city's unique urban design, walking infrastructure, population structure, and cultural context. These factors may differ from those in other urban areas, thereby limiting the generalisability of the findings.
In summary, this model can be applied to explore other health-related behavioral intentions among older adults. Future research should recruit a more balanced age group, employ mixed survey methods to overcome technological barriers, and expand the sample size to include participants from multiple cities to enhance its applicability.
Implications for Practice
Promoting positive attitudes: As attitudes were identified as the strongest predictor of leisure walking intention among older adults, interventions should prioritize strategies that enhance positive perceptions of walking, such as fostering enjoyable and meaningful walking experiences.
Strengthening health motivation: Given that perceived health threats and benefits significantly shape attitudes toward walking, tailored health education programs should highlight the risks of inactivity and the broad benefits of regular walking to increase motivation and intention.
Improving the residential environment: With environmental barriers emerging as the most influential external factor, urban planners and community leaders should focus on optimizing sidewalk quality, lighting, resting facilities, and connectivity to create supportive environments for walking.
Building supportive social norms: Since environmental barriers also impact perceived social norms, communities should implement age-friendly initiatives and social support networks, such as group walking programs, to foster positive social expectations around walking, especially when environmental conditions are limited.
Addressing personal barriers and confidence: As personal barriers primarily affect perceived behavioral control, interventions should provide resources like fall prevention workshops, physical training, and counseling to empower older adults and reduce self-perceived obstacles.
Supplemental Material
sj-pdf-1-her-10.1177_19375867251365886 - Supplemental material for Predicting Leisure Walking Intentions Among Older Adults in Urban Residential Areas: Extended Theory of Planned Behavior and Health Belief Model
Supplemental material, sj-pdf-1-her-10.1177_19375867251365886 for Predicting Leisure Walking Intentions Among Older Adults in Urban Residential Areas: Extended Theory of Planned Behavior and Health Belief Model by Jinhui Zhuge, Wan S. Wan Mohamed and Shureen F. Abdul Shukor in HERD: Health Environments Research & Design Journal
Supplemental Material
sj-pdf-2-her-10.1177_19375867251365886 - Supplemental material for Predicting Leisure Walking Intentions Among Older Adults in Urban Residential Areas: Extended Theory of Planned Behavior and Health Belief Model
Supplemental material, sj-pdf-2-her-10.1177_19375867251365886 for Predicting Leisure Walking Intentions Among Older Adults in Urban Residential Areas: Extended Theory of Planned Behavior and Health Belief Model by Jinhui Zhuge, Wan S. Wan Mohamed and Shureen F. Abdul Shukor in HERD: Health Environments Research & Design Journal
Footnotes
Data Availability Statement
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Ethics Committee of Universiti Putra Malaysia (JKEUPM Ref No: JKEUPM-2024-168) on March 06, 2024. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Informed Consent
All participants provided written informed consent prior to enrollment in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.