
Abstract
Background:
Diabetes self-management education and support (DSMES) is a critical component of diabetes care, but time for it is often limited. Digital tools, such as mobile applications (apps), show promise in extending efforts and supporting self-management education, but have not been fully used. Objectives of this multi-phase study were to (1) evaluate an app designed to support patients with insulin therapy and (2) examine provider perspectives on DSMES apps.
Methods:
Phase 1: Thirty-two adult patients with type 2 diabetes new to or having difficulties with insulin therapy were introduced to the BDTM Diabetes Care App. Three-month app use and satisfaction and changes in hemoglobin A1c (HbA1c) and diabetes distress were assessed. Phase 2: Sixty diabetes providers completed a survey about their experiences with and perspectives on DSMES apps.
Results:
Phase 1: Patients reported satisfaction with the app, and significant improvements in HbA1c and diabetes distress were observed. Phase 2: Most providers viewed apps as adjuncts to diabetes education. Only 33% had previous app experience; however, 100% would consider recommending apps to their patients. Most would spend 5-15 minutes introducing apps to patients. All respondents agreed that the following DSMES app features—evidence-based educational content, data logging and tracking features, customizable user experience, digital coaching via goal setting or reminders, and ability to share data with providers—are key components to consider.
Conclusions:
Findings suggest DSMES apps can play a role in self-management support and provide guidance on factors to consider when introducing digital tools into clinical practice.
Trial Registration:
Clinicaltrials.gov, #NCT03999268
Introduction
Diabetes self-management education and support (DSMES) is a critical component of diabetes care.1 -3 Health care professionals (HCPs) caring for patients with diabetes are expected to perform this service, but time and resources for it are often limited, especially for ongoing support. 4 During patient visits, HCPs are tasked with addressing many patient needs. Patients often feel overwhelmed and may have additional questions; however, it may be difficult to effectively address all patient-related and disease-related concerns within the constraints of a typical visit. Introducing insulin therapy is particularly problematic during a brief routine outpatient encounter or during hospitalization. Teaching people to administer an injection requires time and ongoing support. 5
Compounding these challenges is the shortage of HCPs available to deliver DSMES 6 coupled with chronically low utilization of existing services.7,8 Even when there is a local Diabetes Care and Education Specialist (DCES), access to patients may be problematic. In recognition, DSMES standards emphasize the need to seek ways to improve availability of and participation in DSMES, including technology. Digital tools, such as mobile health applications (apps), show promise in extending efforts and supporting self-management, but have yet to be fully realized.9 -11 There remains a need to identify effective tools and to understand what factors influence a provider’s decision to recommend apps and patients to use them. 11
Recognizing the potential role that mobile apps can play in DSMES, the “Diabetes Care App” 12 was developed to supplement the efforts of HCPs and to assist adults with diabetes with their self-management behaviors. The app was built on current evidence-based content used in formal DSMES 13 and is designed to support DSMES rather than replace it. The app contains general lifestyle information regarding health behaviors and specific information for individuals new to insulin therapy, particularly those with type 2 diabetes. Content is designed to be individualized and provided in a variety of learning modalities, using brief articles, short tutorials, and videos designed to foster skill development and self-efficacy to successfully perform self-management behaviors. 14 Specific to insulin therapy, support is built into the app in the form of articles and tutorials to address fears and concerns related to the initiation and use of insulin therapy while providing information on injection administration and self-management content necessary to assure patient confidence and empowerment with insulin therapy. This educational support app was formatively evaluated in a diabetes outpatient clinic to guide direction on enhancements and improvements to the app’s content and features and to ensure the feasibility of integrating such an app into busy clinical practice. 15
Building on these efforts, the objectives of this study are to (1) evaluate experiences and outcomes of patients with type 2 diabetes in using the app to support insulin therapy and (2) examine HCP perspectives on the role of the app and other mobile apps to deliver DSMES and support self-management behaviors.
Methods
This study was carried out in two phases, which were approved by the University of Pittsburgh’s Institutional Review Board.
Phase 1
This was a pilot study without a control group. Patients who were ≥18 years with type 2 diabetes and requiring insulin therapy education (new to or identified as having issues with insulin therapy) were recruited from participating outpatient clinics and academic hospitals. To be eligible for the study, patients also had to be able to read and follow instructions in English, have a smart phone that was compatible with the app, and be willing to upload it on their devices. Those who agreed to participate in the study provided written informed consent.
Participants who enrolled in the study received insulin therapy education from an HCP who typically delivers diabetes education (eg, DCES, nurse, pharmacist) according to standard practice. 5 During the encounter, the HCP introduced participants to the app and its features and reviewed a handout that described its elements and educational content. The HCP also helped the participant install the app on their smartphone or provided the patient with instructions to install the app on their own. No additional instruction on app use was given to participants. Participants were able to use the app as much or as little as they preferred over the course of a three-month period.
Study outcomes included app use, glycemic control, diabetes distress, and participant satisfaction. Participant usability data (frequency and type) were tracked through the app’s data analytics software platform. Hemogloblin A1c (HbA1c) served as the clinical outcome and measure of glycemic control. HbA1c values were obtained from the electronic medical record system; available values corresponding to baseline and approximately three-month follow-up were extracted. Diabetes distress was assessed at baseline and follow-up using the Diabetes Distress Scale, a 17-item self-report scale. 16 Each item is rated on a six-point scale from “not a problem” to “a very significant problem.” The scale yields an overall distress score based on the average responses for all 17 items plus scores for four subscales—emotional burden (feeling overwhelmed, frightened or fearful about managing the demands of diabetes over time), regimen distress (feeling of failure by not managing diabetes well, for example, meal plan, exercise), interpersonal distress (feeling of not feeling sufficient support for diabetes among family and friends), and physician distress (worries about health care and obtaining sufficient expertise, support, and directions from health care providers). Higher scores indicate higher levels of distress. Participant satisfaction with the app was self-reported using a survey developed for this study. The survey included 10 Likert-scale items assessing overall satisfaction with the app as well as satisfaction with the design, ease of use, visual appeal, content (understandability and usefulness of app, videos, and articles), intention for future use, and likelihood of recommending to others.
Phase 2
Diabetes HCPs representing inpatient, outpatient, and community settings were invited to complete a survey developed for this study to gather information about their experiences with and perspectives on mobile app use for DSMES (see Supplementary Material). In addition, to general questions about mobile apps, respondents answered questions specific to the Diabetes Care App after viewing a brief video that presented information about installation, features, content, and functionality. The survey was administered in both paper format and using the Qualtrics online survey platform. Prior to administering, the survey’s content validity was assessed by four DCESs experienced in DSMES and evaluating mobile apps. They rated item relevance on a four-point Likert scale from “not at all relevant” to “extremely relevant” and also shared comments about word choice, clarity, and importance.17,18 Relevance ratings and comments were reviewed by members of the study team and used to guide survey modifications.
Statistical Analysis
Descriptive statistics were used in both phases to describe participant characteristics and report on app use and experiences. In addition, for phase 1, change in HbA1c and Diabetes Distress Scale scores was assessed using paired t tests. Data were analyzed using SPSS (version 28, IMB Corp, 2021).
Results
Phase 1
Participants (n = 32) were 37.5% women and 71.9% white non-Hispanic, with a mean age of 57.2 ± 10.5 years (range, 30.6-70 years) and baseline mean HbA1c of 10.4% ± 2.3%. The mean duration of diabetes was 11.3 ± 11.4 years (range, 0.8-36 years) for those with an available diagnosis date (n = 26); 28% of all participants were new to insulin therapy. All but one participant used the app; 84% launched it within one day of enrollment. The average app use was 10 times over the course of the study. Most participants accessed curriculum (articles and videos) about insulin pen therapy (74%), followed by living with diabetes (45%).
For those with a follow-up HbA1c (n = 22), glycemia significantly improved during the study period, with an average reduction in HbA1c of 2.5% ± 2.6% (P < .001). Significant reductions in the Diabetes Distress Scale total score and Emotional Burden subscale scores were also observed (Table 1). Of those participants who completed the satisfaction survey (n = 27), most found the app easy to use (81.4%), visually appealing (85.2%), and to contain helpful content (81.5%), especially articles (92.6%). A majority (85.1%) reported that they would recommend the app to another person with diabetes.
Change in Diabetes Distress Scale Scores Among Patients With Type 2 Diabetes on Insulin Therapy.
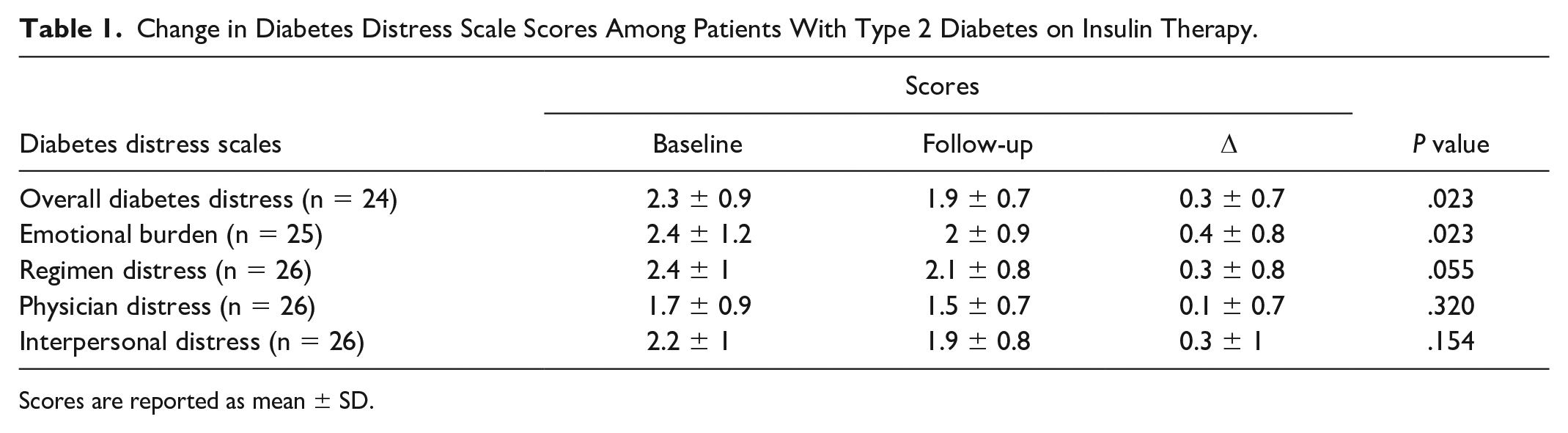
Scores are reported as mean ± SD.
Phase 2
Sixty HCPs including 33% DCESs, 21% endocrine clinicians, 18% nurses, 13% dietitians, 5% primary care providers, and 5% advanced physician providers completed the survey. Of those, 17% (10/59) and 44% (26/59) reported being very familiar and moderately familiar with diabetes mobile apps, respectively. Health care professionals indicated that their colleagues were the most frequent source of information about diabetes mobile apps (68%), followed by professional meetings (47%), professional organization communications (eg, newsletters, journals, 25%), diabetes blogs (20%), and general online mobile app marketing (18%).
HCP experience with mobile apps
Only 33% (20/59) of respondents had previous experience using a mobile app for diabetes education, whereas 25% (15/59) had used an app for support. Among those who had experience with diabetes mobile apps, the average rating for app usefulness was 6.5 on a 10-point scale (10 = very useful). Interestingly, of the HCPs who had never used a DSMES app, 100% indicated that they would consider introducing one to their patients.
Role of mobile apps for DSMES
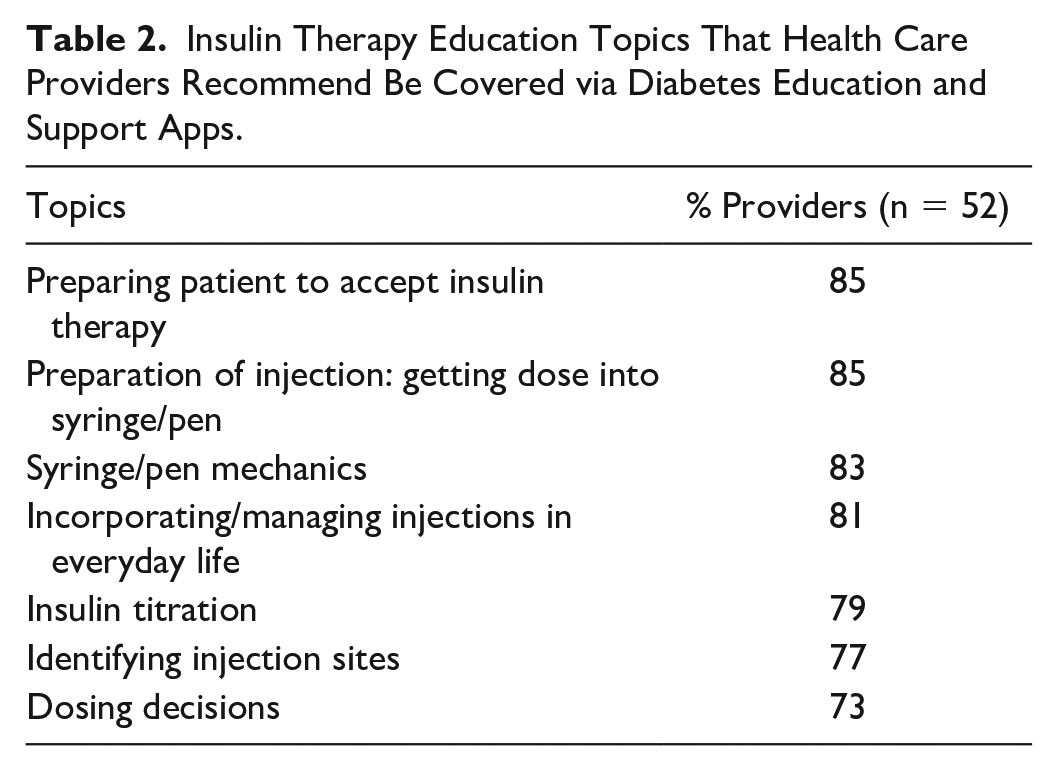
Most respondents (95%) viewed apps as an adjunct to DCES education, particularly for reinforcement of instruction. They also agreed that apps could serve as a helpful resource after hospital discharge (79%) and to support information and reduce time spent answering questions at follow-up visits (71%). In addition, 75% agreed that apps may be particularly useful to patients who use telehealth visits for care and education and/or live far from clinics. Specific to insulin therapy, most respondents agreed that apps could serve as a tool to prepare those new to insulin and aid with injection skills, dosing decisions, and titration in addition to their instruction (Table 2).
Insulin Therapy Education Topics That Health Care Providers Recommend Be Covered via Diabetes Education and Support Apps.
Factors to consider when recommending DSMES mobile apps to patients
Patients’ access to and interest in mobile apps were rated as the most important factors to consider when recommending mobile apps to patients for diabetes education and support (Table 3). Time was also an important consideration. In fact, 43% (17/40) of HCPs reported that they were only willing to spend five minutes to download and teach mobile app use to patients; 32.5% (13/40) would spend 15 minutes, 22.5% (9/40) would spend 30 minutes, and only one HCP indicated that they would spend 45 minutes or more.
Factors That Health Care Providers Agree Should Be Considered When Recommending Diabetes Self-Management Apps to Patients.
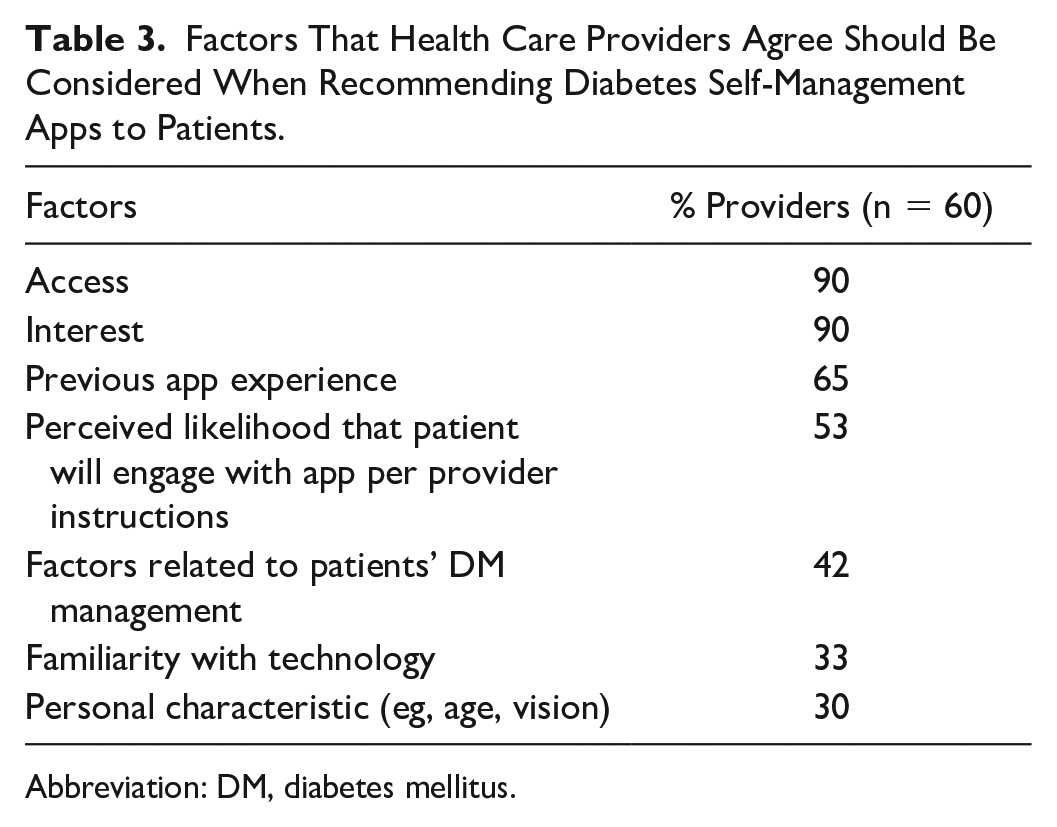
Abbreviation: DM, diabetes mellitus.
Beneficial DSMES mobile app features
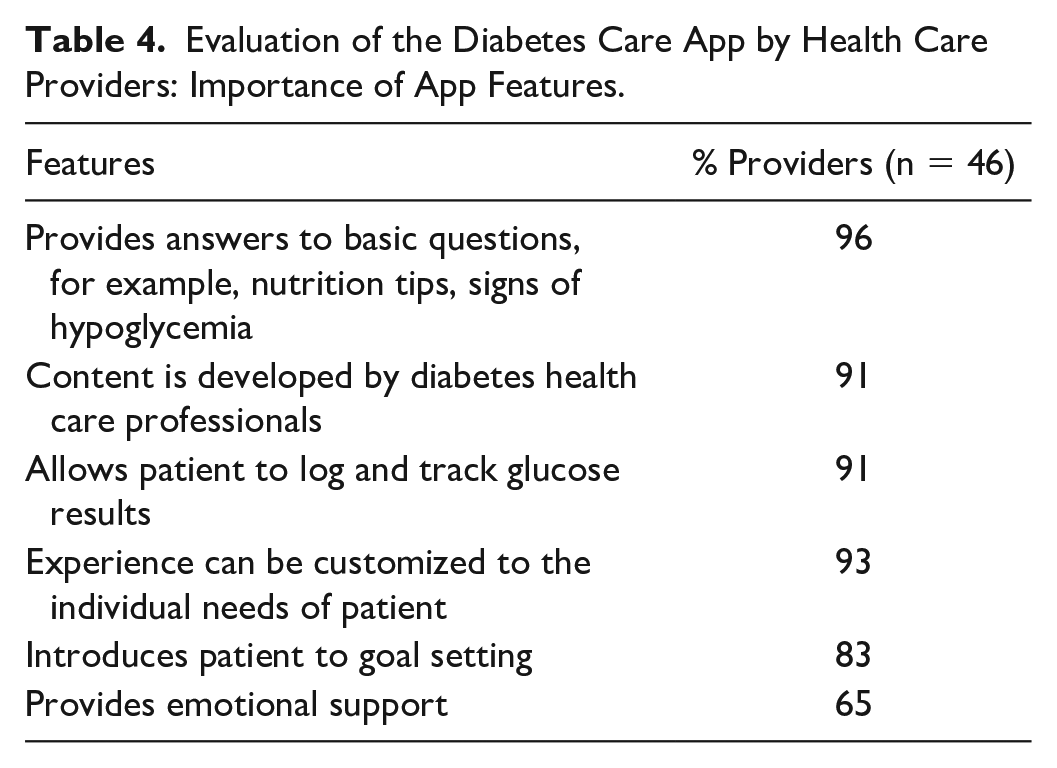
When leveraging mobile apps for DSMES, 100% of respondents rated the following features as potentially useful to patients with diabetes: evidence-based educational content, data logging and tracking features, customizable user experience, digital coaching via goal setting or reminders, and ability to share data with providers. Ninety-six percent of respondents thought including telehealth features (ability to video chat or message providers) as part of apps would be useful to patients with diabetes. These general responses were reflected in the specific evaluation of the study app (Table 4).
Evaluation of the Diabetes Care App by Health Care Providers: Importance of App Features.
Discussion
The National Standards for DSMES 19 and the Medical Care of Diabetes 3 refer to the use of digital technology as a means to provide reach and real-time engagement in self-management. They also note that while data support technology aiding in better outcomes, additional assessment must be considered. Our study, involving both patients who received DSMES via an app and diabetes providers representing a variety of disciplines and practice settings, contributes to the understanding of how mobile apps can support diabetes self-management.
Our evaluation of an educational support app with patients who were new to or having difficulties with insulin demonstrated improvement in diabetes outcomes and satisfaction with the app. Like other studies of DSMES mobile apps, reductions in HbA1c were observed in our study. 9 In the case of our study, glycemic improvements are likely attributed to starting and/or improving adherence to insulin therapy. The degree to which app engagement contributed to glycemic improvement is unknown and needs further study. Interestingly, findings suggest that the app may have addressed psychosocial aspects of diabetes self-management beyond glycemia. In our sample, diabetes distress decreased, specifically in the area of emotional burden. This is notable given that the Diabetes Care App was designed by a DCES in part to support individuals on insulin therapy and includes content to address fears and concerns associated with insulin therapy as well as skill development. Many patients with type 2 diabetes are reluctant to begin insulin therapy, even when recommended by a physician. This phenomenon, often referred to as “psychological insulin resistance,”20,21 is associated with a variety of factors including needle phobia, low self-efficacy relative to properly administering injections, and fear of hypoglycemia. 22 In our previous study of psychological insulin resistance, patient focus groups revealed a strong desire for knowledge on injection logistics and considered education and demonstration of tools to be important features in influencing their willingness and continued adherence to insulin. 23
Most HCPs surveyed in our study concurred that digital tools designed to address the needs of individuals on insulin therapy can serve to supplement education and training provided by an HCP, especially when time is limited. Mobile apps may also play an important role in ongoing support for patients with diabetes. While initial education is necessary and valuable, ongoing support is reported to be critical for sustained outcomes. 19 Ongoing support helps patients to implement and sustain the knowledge, skills, coping, and behavioral strategies needed to self-management. 19 With the national shortage of DCESs, tools that provide this support and access are needed.
Our study findings also provide guidance on factors to consider when introducing digital tools into clinical practice. Health care professionals unanimously agreed that they would consider using a mobile app with patients, yet only a fraction of HCPs in our study had previous experience using them for DSMES. These findings coupled with the fact that many mobile health apps are commercially available 24 and indicate a need to improve the way apps are introduced to HCPs. This is especially relevant as the recommendation of apps by health professionals has been reported to be associated with patient app use and satisfaction.11,25 In a systematic review of the determinants of diabetes self-management apps, it was reported that HCPs were less likely to recommend such apps if they did not perceive their benefits or credibility. The review also found that young and “technology-savvy” HCPs were more likely to recommend self-management apps to patients. 11 Similarly noted during the formative evaluation of our study app, not only do patients need a level of “tech readiness,” but so do HCPs who are supporting the use of digital tools. 15 HCPs must be confident in and knowledgeable about the digital technology and its capabilities. Given that more than 40% of HCPs in our study stated that they would only spend five minutes presenting apps to patients, DSMES apps need to be promoted in a way that this knowledge can quickly be gained and successfully shared with patients, whether in-person or remotely.
This study has limitations. Phase 1 used a pre/post-evaluation design with a small sample size and did not include a randomized controlled group. This phase of the study was mostly conducted during the COVID-19 pandemic, which impacted in-person recruiting, training, and data collection while telehealth was simultaneously being introduced. Further investigation with a more robust study design is warranted to confirm and expand upon the results of this trial. For phase 2 of the study, although HCPs who participated represented diverse areas within a health system, the sample may not have been representative of other health systems and/or geographical areas, thereby potentially limiting the generalizability of the findings.
Conclusions
Digital tools can play an important role in diabetes self-management. Findings from this study indicate that mobile apps offer a promising approach to support patients with type 2 diabetes with insulin therapy. In addition, this study, along with others, provides guidance on ways to successfully introduce DSMES mobile apps into clinical practice and promote their utilization. The recommendations should be carefully considered as health care systems continue to seek ways to support quality care and education for the growing number of patients with diabetes.
Supplemental Material
sj-docx-1-dst-10.1177_19322968231174037 – Supplemental material for Mobile Applications to Support Diabetes Self-Management Education: Patient Experiences and Provider Perspectives
Supplemental material, sj-docx-1-dst-10.1177_19322968231174037 for Mobile Applications to Support Diabetes Self-Management Education: Patient Experiences and Provider Perspectives by Jodi S. Krall, Belinda Childs and Neha Mehrotra in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
The authors wish to thank the patients, providers, and investigators who participated in this study.
Abbreviations
App, application; BD, Becton, Dickinson and Company; DCES, Diabetes Care and Education Specialist; DSMES, Diabetes Self-Management Education and Support; HbA1c, hemoglobin A1c; HCP, health care professional.
Authors’ Note
Prior Presentation: Parts of this study were presented in abstract form at the American Diabetes Association’s Scientific Sessions in 2021 and 2022.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jodi Krall had research support from Becton, Dickinson and Company and Sanofi, Inc. Belinda Childs had a speaking honorarium from Sanofi, Inc., was on an Advisory Board for ProventionBio, and received research support from Abbott Diabetes; payments went to her employer (Great Plains Diabetes Research, Inc.).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Becton, Dickinson and Company
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.