
Abstract
Background:
Digital app interventions have been shown to enhance medication adherence and self-management of type 2 diabetes mellitus (T2DM), leading to improved glycemic outcomes. Despite the availability and ease of access to these apps, the adoption remains low. Therefore, this study aimed to explore strategies to increase the adoption of mobile apps for medication adherence and T2DM self-management.
Methods:
This study employed a constructivist grounded theory approach. Data were collected through 30 semi-structured in-depth interviews and then analyzed using thematic analysis to identify the strategies.
Results:
The developed model highlighted five key dimensions: technological, economic, social, behavioral, and environmental strategies. Technological strategies discussed user interface and user experience. Economic strategies stressed the importance of financial support. Meanwhile, social strategies focused on social support and partnership. Behavioral strategies emphasized motivation. Environmental strategies included marketing, patient education, health care professionals’ roles, supportive assistance, policy, and evidence-based approach.
Conclusions:
This study offers actionable insights and a blueprint to increase the adoption of mobile apps for T2DM medication adherence and self-management, which requires the collective and collaborative efforts from different stakeholders. Nevertheless, the self-efficacy of patients remains low, justifying the need for further patient education and empowerment.
Introduction
Diabetes is common worldwide, affecting 537 million adults, with 90% having type 2 diabetes mellitus (T2DM). 1 Effective T2DM management requires self-management behaviors coupled with pharmacotherapy. 2 These include medication adherence, self-monitoring of blood glucose (SMBG), physical activity, and healthy eating. 3 Nevertheless, achieving optimal glycemic control remains challenging as the prevalence of poor glycemic control was 66%, primarily due to poor medication adherence and self-care behaviors.4,5 The prevalence of non-adherence varied widely from 6.9% to 90.6%. 6 Consequently, this could lead to complications such as retinopathy, neuropathy, and nephropathy, as well as increased health care expenditures. 6
Digital health interventions show the potential to enhance self-management, improve medication adherence and glycemic outcomes, including both glycated hemoglobin (HbA1c) and fasting plasma glucose. 7 Several features of an ideal T2DM app should be considered, which are medication reminders, pairing with glucometers and blood pressure machines, patient education on healthy eating, easy documentation, and information sharing with health care professionals. 2
Despite the availability of many free, high-quality mobile health (mHealth) apps, with an average user rating of 4.7 out of 5, the adoption remains low. 8 This low utilization prevents T2DM patients from enjoying the benefits of these apps. Similarly, Bults et al 9 reported that the mobile app interventions have not been integrated into routine diabetes care, recommending future research to explore ways to increase the implementation of mHealth apps in current practice.
Previous literature has extensively explored the facilitators and barriers to the adoption of mHealth apps among T2DM patients.9-11 Several factors must be considered, including user-friendly design, functionalities that meet patient needs, security, and health care professional endorsement, as well as addressing obstacles such as low awareness, digital literacy, and cost to ensure successful integration into diabetes management. Nevertheless, the practical translation of these findings into real-world practice and implementation remains unclear.
There is a critical gap in understanding how these factors could be effectively targeted and the mechanisms through which adoption can be enhanced. Previous studies do not adequately address the low adoption issues. Furthermore, there is insufficient knowledge in the existing literature regarding actionable strategies that can be employed to increase app utilization, even after the influencing factors have been well elucidated. By developing a theoretical model grounded in the perspectives and experiences of key stakeholders, this study aimed to explore and identify strategies to increase the adoption of mobile apps designed for enhancing medication adherence and self-management among T2DM patients.
Methods
Study Design
A qualitative interpretation research epistemology, particularly the grounded theory approach for qualitative inquiry was ideal for this study as it aimed to explore new knowledge and insights contributing to a comprehensive theoretical explanation. This study employed Charmaz’s grounded theory approach that was based on the constructivism paradigm. 12 This paradigm aimed to discover multiple realities that were shaped by individual subjectivity, experiences, and perspectives.
One-to-one semi-structured in-depth interviews were conducted with various stakeholders, including patients and health care professionals to gather their views and opinions on strategies to increase the uptake of digital apps to enhance medication adherence and self-management of T2DM.
Interview Guide Development
The interview guide was developed based on a previous study that employed the Technology Readiness and Acceptance Model (TRAM) as its theoretical foundation to identify key factors influencing the adoption of mobile apps among T2DM patients, 13 and was further guided by expert opinions and the objectives of this study. The expert panel comprised three clinical pharmacists. The first author (C.C.J.) drafted the interview guide, which was later refined by the expert panel (M.M.B., E.H., and N.A.M.T.). The interview guide consisted of a series of predetermined open-ended questions as shown in Supplemental Appendix A.
Study Setting and Participant Recruitment
Participants comprised both patients and health care professionals. Participants were recruited through purposive and theoretical sampling. Initial purposive sampling directed data collection based on the listed inclusion and exclusion criteria. The patient inclusion criteria were (1) diagnosed with T2DM and currently on antidiabetic medication; (2) aged 18 years old and above; and (3) able to communicate and understand the interview questions. Participants who were unwilling to provide informed consent were excluded. The patients were recruited at the Endocrine Clinic, Hospital Canselor Tuanku Muhriz. They were identified from the appointment list for diabetic clinics every Wednesday. While waiting to see doctors, C.C.J. approached them to introduce the study and invite them to participate. Meanwhile, the inclusion criterion for health care professionals was their involvement in the management of T2DM patients. Potential health care professionals such as doctors, Diabetes Medication Therapy Adherence Clinic (DMTAC) pharmacists were invited via formal invitation letters. Health care professionals with less than one year of clinical experience in managing T2DM patients were excluded.
Theoretical sampling seeks and gathers additional data guided by concepts emerging from initial data analysis. This process may include recruiting participants with additional diversity within the same group, introducing new participant groups, expanding data collection sites, or incorporating new interview questions. 14 As the study progressed, theoretical sampling guided the inclusion of additional participants to further explore the emerging concepts. Through ongoing data analysis, initial findings highlighted the role of community pharmacists and registered dietitians in supporting T2DM patients, given the widespread accessibility of community pharmacies and the importance of healthy eating in diabetes care. Consequently, theoretical sampling led to the recruitment of these professionals to enrich the data and offer a more comprehensive understanding of the strategies needed to enhance app adoption.
Ethical Approval
This study received ethical approval from the Research Ethics Committee of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2022-650). Written informed consent was obtained from all participants prior to taking part in this study. This included the consent to record the interview sessions. Numerical codes were assigned to each participant to ensure confidentiality and anonymity, with patients labeled as P and health care professionals as HCP.
Data Collection
Data were collected through 30 semi-structured in-depth interviews from April to May 2024 by C.C.J., who was fluent in the main languages used in this country and had prior experience in running qualitative research. The interviews with patients were conducted face-to-face at the Endocrine Clinic, whereas the interviews with health care professionals were conducted online via Zoom. The interview sessions were audio-recorded and field notes were taken throughout the data collection process. The interviewer summarized the gathered information from the interviews and field notes, and subsequently clarified with the participants to ensure accuracy. The sample size was determined by theoretical saturation rather than by the need for demographic representativeness. 15 Data collection continued until theoretical saturation was achieved, defined as the point whereby new categories stopped emerging.
Data Analysis
Data collection and analysis occurred simultaneously. The recorded interviews were transcribed verbatim by C.C.J. and verified by M.M.B. Interviews conducted in other languages such as Malay and Mandarin were first transcribed and then translated into English by C.C.J., verified by M.M.B. The data were then analyzed thematically using ATLAS.Ti 23, following steps recommended by previous literature. 16 This included three main stages of coding (initial, focused, and theoretical) combined with a constant comparison approach. Before coding, C.C.J. initially immersed in the transcripts by reading them multiple times, and referring to field notes to enhance familiarization and theoretical sensitivity, which is the ability to recognize and interpret significant data relevant to theory development. 16
There were three major steps in the coding process. The first step was initial coding, also referred to as open coding, where the quotations from the transcripts were highlighted and assigned with codes line-by-line. The second step was focused coding, which involved clustering the relevant or redundant initial codes into categories, namely subthemes and themes, through selective and conceptual coding. This was followed by theoretical coding, where the themes that were conceptually connected were further categorized into dimensions that formed the model of strategies to increase app adoption in T2DM. 17
A constant comparison approach was used to compare the codes within and across transcripts. This iterative process helped to identify similarities and differences, thereby refining and solidifying the categories. The research team met regularly to review the codes, reconcile coding disagreements, and refine the themes. Throughout the data analysis and theory development process, the research team applied theoretical memoing to record thoughts and interpretations to foster reflexivity. 18 The research team discussed any ambiguities and discrepancies until reaching a consensus. A theoretical model was built from the data collected.
Rigor of Study
The Standards for Reporting Qualitative Research (SRQR) guided the reporting of this study as supplied in Supplemental Appendix B. 19 Credibility refers to the accuracy of the findings in reflecting participants’ views and their interpretation by the researchers. Peer debriefing among the research team enhanced the trustworthiness and credibility. 20 The research team kept on discussing and reviewing the emerged codes, subthemes, and themes until reaching a consensus. Transferability is about the generalizability of the findings beyond the original study context. Dependability relates to the consistency of the findings across time and similar contexts. A detailed description of this study protocol covering data collection and analysis was documented to enhance transferability and dependability. 21
Results
This study included a total of 30 participants, comprising eight patients, three doctors, nine DMTAC pharmacists, nine community pharmacists, and one registered dietitian. All community pharmacists and the registered dietitian had experience in introducing and advocating mobile apps for medication adherence and T2DM management. The mean duration of the interview was 32 ± 5 minutes. Overall, the model of strategies to increase app adoption in T2DM was illustrated in Figure 1, comprising five dimensions. A total of 30 strategies were identified.
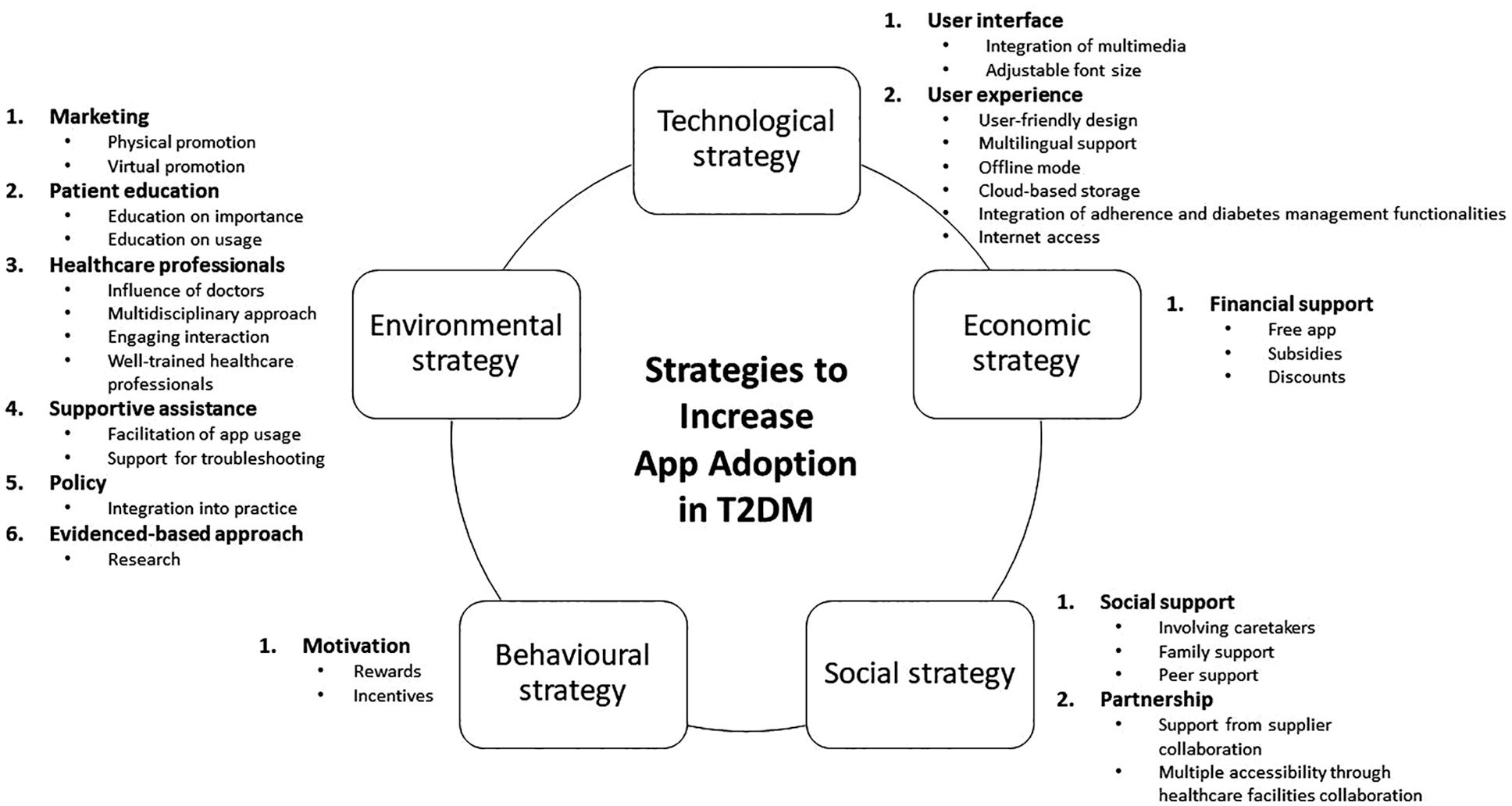
Strategies to increase app adoption in T2DM.
Technological Strategy
Two themes, namely, user interface and user experience, with seven subthemes emerged under technological strategy. For user interface, participants highlighted the need of incorporating multimedia to enhance understanding, especially for older users or those with lower education levels. For example, visual elements such as pictures, numbers, and colors, as well as audio cues instead of text were suggested: If the app has a more user-friendly symbol or icon, using numbers more than words, it would definitely help, especially among the elderly. (Integration of multimedia) (HCP23)
Furthermore, participants suggested that an adjustable font size would be a useful feature, making the app more accessible for older users with vision impairments: The app must be elder-friendly. For example, big fonts with color. (Adjustable font size) (HCP3)
To enhance user experience, several suggestions were proposed. Participants frequently emphasized the importance of user-friendly designs that were intuitive and required minimal effort to learn and use: These apps need to have user-friendly functions and designs, and take very little time to familiarize with, simple and straightforward navigation. (User-friendly design) (HCP8)
Participants also emphasized the importance of multilingual support, noting that many elderly users were more comfortable using apps in their native languages: The apps should include different languages, specifically Malay, English, Chinese, and Tamil. I found that many elderly patients have trouble understanding Malay and English. Many of them are more well-versed in their own mother tongue. (Multilingual support) (HCP7)
The ability to function offline was identified as an important feature, particularly for users in rural areas that faced poor internet connectivity: In certain areas in Pahang, it is quite rural. Perhaps the app could not only function online but also function offline because some patients may have limited or intermittent internet connectivity. (Offline mode) (HCP27)
To overcome the barrier of limited phone storage, participants suggested using cloud-based data storage: Cloud-based data storage instead of phone storage. (Cloud-based storage) (HCP5)
Participants also suggested integrating adherence and T2DM management functionalities into existing widely used apps. This integration would enhance convenience by reducing the burden of downloading new apps and the need to use multiple apps simultaneously: Instead of using multiple apps, why not just use the established app, MySejahtera (Malaysia’s COVID-19 app) and just upgrade or include one more function for diabetes because patients already have the app in their phones. (Integration of adherence and diabetes management functionalities) (HCP30)
Additionally, participants recommended offering internet access in health care facilities to support the process of downloading and installing the apps. This initiative would facilitate easier access to digital health management tools and improve the overall user experience: Provide support for internet connectivity, especially in healthcare facilities so that patients can download and install the apps. (Internet access) (HCP6)
Economic Strategy
One theme, namely financial support, with three subthemes emerged under economic strategy. The availability of free apps would enhance patients’ willingness to try the apps, thus encouraging adoption: If there is no need to pay, I think many people will definitely take it. (Fee app) (P12)
Participants indicated that government subsidies were crucial in alleviating the financial burden, thus facilitating broader adoption among patients from diverse social and economic backgrounds: Government should provide subsidies to the patients who are willing to adopt digital health interventions so that they can get access to digital devices and the internet needed for these interventions. (Subsidies) (HCP1)
Offering discounts on glucometers that are compatible with the apps, along with discounted test strips would further incentivize their usage: Offer a discounted price for a Bluetooth glucometer, which has the function of storing SMBG records directly in the mobile app. (Discounts) (HCP4)
Social Strategy
Two themes, namely social support and partnership, with five subthemes emerged under social strategy. Social support including caretakers, family, and peers is crucial especially among older patients with limited digital literacy. Recognizing that not all patients are proficient in technology, involving their caretakers is deemed essential to promote app usage. Caregivers could remotely monitor patients’ health conditions through the app: Involve caregivers and allow caregivers to download and sync patient’s information. For example, if I’m in KL (Kuala Lumpur) but my mother is in Kuching, I still know my parent’s health conditions. We can give the caregivers an online e-manual, so when patients go back, their children can help them. (Involving caretakers) (HCP29)
Family members could also play a key role in facilitating and assisting patients to overcome technical barriers, especially in-home settings: It is a new thing to me. I need my children to teach me and guide me at home if I forget how to use it because before this, it was my children to help me download and teach me. (Family support) (P14)
In addition, peer influence such as shared experiences could motivate and attract patients to adopt the apps: We can do some peer support because sometimes, they believe more in their peers who have the same condition. For example, the words coming from other patients like the testimonials actually motivate the patient to try using the apps. (Peer support) (P27)
Participants described the advantages of fostering partnerships with other parties such as suppliers and health care facilities. Collaborating with glucometer suppliers could boost app visibility and make SMBG more affordable: We run subscription models by supplying the strips at a lower price with the support of the supplier. The app itself so far none of the suppliers are charging the patients. Perhaps can we work with a glucometer supplier who is open to collaboration opportunities. The supplier actually sponsors the glucometer. (Support from supplier collaboration) (HCP25)
Furthermore, broadening access to apps could be achieved through collaboration with various health care facilities such as community pharmacies, thus increasing adoption across different points of care: Maybe the collaboration part. Hospitals can connect with community pharmacies, like continuity of care after their DMTAC appointment to increase patients’ engagement to use the app. (Multiple accessibility through healthcare facilities collaboration) (HCP24)
Behavioral Strategy
One theme, namely motivation, with two subthemes emerged under behavioral strategy. Participants consistently pointed out the positive impacts of rewards on motivating patients to adopt the apps. These included offering rewards for improved medication adherence, better blood glucose control, and regular app engagement. Examples of the rewards encompassed redeemable points or vouchers for purchasing glucometer test strips and insulin pen needles. Moreover, ongoing encouragement and recognition were identified as crucial factors in sustaining user engagement and ensuring continued usage: Rewards like giving the vouchers to buy test strips, needles, alcohol swabs as it helps to save their cost. (Rewards) (HCP26)
Depending on a country’s health care policy, at the initial stage of implementation, incentives could act as a potential motivator to encourage health care providers to actively promote the apps and recruit patients to download and use them: Maybe some incentives from the company selling the CGM (continuous glucose monitoring) or glucometers to the pharmacies. (Incentives) (HCP24)
Environmental Strategy
Six themes, namely, marketing, patient education, health care professionals, supportive assistance, policy, and evidence-based approach, with 12 subthemes emerged under environmental strategy. For marketing purposes, promotion could be conducted either physically or virtually to boost awareness of the apps. Physical promotion efforts include campaigns and printed materials. These initiatives need regular implementation to ensure continuous exposure, thereby addressing the barrier of low awareness: Give talks to patients regarding the latest technology in T2DM management and how technology can help in managing T2DM. For example, able to trace the SMBG records with trend analysis, notifications from the apps to serve as reminders for patients regarding their medication administration and blood sugar control. (Physical promotion) (HCP4) The hospital needs to issue pamphlets or flyers for people to know that the app exists. (Physical promotion) (P10)
The use of virtual promotion, particularly through social media platforms is an effective strategy for reaching a broader audience besides promoting the apps to targeted potential users: Promotion of the apps to the public through social media in different languages. For example, demonstrate how to use the apps and the potential benefits, show some examples of real-life success cases in terms of reduction of the HbA1c and FBS. (Virtual promotion) (HCP5)
Furthermore, patient education on the importance of using the apps could be disseminated to the public as many patients fail to recognize the benefits in adherence and T2DM management. This could be achieved through educational campaigns conducted at health institutions, where health care professionals directly explain the practical benefits of the apps to patients. This would help foster awareness and set expectations about how the apps can aid in improving medication adherence and self-management: You need to explain to patients the importance of these apps. If you don’t explain, who will use them? So, people will feel it’s not important. (Education on importance) (P21)
Participants also emphasized the importance of providing clear instructions on how to use the apps. Education on app usage could be facilitated through physical demonstration and visual aids, which complement each other to reinforce the learning process: Physical demonstration to patients during follow-up and give step-by-step instructions to patients in written format. (Education on usage) (HCP4)
Health care professionals played a crucial role in introducing and promoting the apps. Participants elaborated on the influence of doctors, noting that patients were more inclined to accept the advice from their doctors regarding app adoption: I think it has to come from the doctor’s advice, telling the patient to use the app, maybe the patient will listen and follow. (Influence of doctors) (P10)
Apart from doctors, a multidisciplinary approach involving various health care professionals such as pharmacists, nurses, diabetic educators, and registered dietitians is important in raising the awareness and promoting the apps: I don’t think doctors have the time. Or pharmacists can also advise you to use the app. Maybe when we take medicines, the pharmacists can show the patients that this app is good for your diabetes. (Multidisciplinary approach) (P16)
The interaction between health care professionals and patients through the apps for consultations and feedback fosters active engagement. As a result, patients are more inclined to adopt the apps for professional guidance and advice: The acceptance can be greatly increased if healthcare professionals such as dietitians and pharmacists provide consultations for free. So, the patients will feel that the app is more useful if they are given feedback and consultations for their blood glucose readings and diet changes. (Engaging interaction) (HCP1)
Before launching the app interventions, health care professionals should undergo comprehensive training to ensure they are knowledgeable about the app functionalities. This would enable them to effectively guide and support patients in using the apps: Need to provide training to healthcare professionals first before launching the intervention because they need to provide the hands-on support and guidance to the patients, so they need to familiarize themselves with the app first before teaching the patients. (Well-trained healthcare professionals) (HCP27)
Moreover, supportive assistance that covers usage and troubleshooting should be provided. After introducing the app to patients, it is crucial to assist them to download, install, register, and set up the app to minimize their learning burden. Hospitals and community pharmacies were suggested as accessible settings to seek for assistance and guidance when users encountered technical challenges with app usage and navigation: Once you set up for me, it will be very easy because you have helped me to key in the medication information and everything is there. I just follow the instructions, click yes when the alarm rings after I take my medication. (Facilitation of app usage) (P11)
Support for troubleshooting common issues or errors is needed to streamline the user experience: In Taiwan, they are prepared for errors and they documented the common errors. So, when the common error is detected, then we can inform our customers, if you have this, then this is what you can do. (Support for troubleshooting) (HCP23)
At the policy level, participants suggested integrating app interventions into health care practices, particularly within government health settings. For example, making app interventions compulsory could rapidly increase app uptake: The acceptance of mobile health can be greatly increased if it is made compulsory for those patients under follow up in government health settings. (Integration into practice) (HCP1)
Lastly, participants recommended conducting research studies to demonstrate the evidence on the effectiveness and feasibility of app interventions before scaling up to a broader population. The data collected could serve as compelling evidence to convince patients to adopt the apps: I think you need to demonstrate. Conduct a randomized control trial and then you observe the outcomes of the disease. If the people who use it show obvious improvement, then you can show it, this is my evidence. If not, people will question why they bother to use apps. (Research) (P18)
Discussion
This study has highlighted a multifaceted model of strategies aiming at enhancing the adoption of mobile apps for medication adherence and T2DM management. These strategies were derived from the perspectives of multiple stakeholders including patients and health care professionals such as doctors, pharmacists, and a registered dietitian, who led the digital diabetes care team in a community pharmacy company. This study has also enriched the literature on digital health by introducing a model grounded in five dimensions, namely technological, economic, social, behavioral, and environmental strategies. The integration of these strategies would establish a holistic and comprehensive approach to address the barriers and promote app adoption, thus increasing the uptake among users.
To aid comprehension among T2DM patients with low health literacy, this study suggests incorporating multimedia elements such as images and colors alongside text. This approach is supported by previous studies, leveraging multiple sensory cues to aid information processing, particularly beneficial for elderly users. 22 For medication reminders and notifications, incorporating loud audio with vibrations could assist patients with hearing difficulties. Moreover, to accommodate patients with low digital literacy, app developers should prioritize designing simple and intuitive navigation interface to minimize learning efforts, thereby facilitating app usage. 23 Hence, evaluating app usability using the mobile application rating scale (MARS) during development is recommended for ensuring user-friendly design. 24 Furthermore, language barriers, particularly limited English proficiency, contribute to health care and digital disparities. 25 This issue is particularly relevant in Malaysia owing to its linguistic diversity, where many elderly patients prefer their native languages such as Malay, Mandarin, or Tamil. Hence, this highlights the necessity of multi-linguistic support in apps, allowing users to switch from English to their native languages to bridge the language gaps.
Lower income has been reported as the barrier to app adoption among patients. 26 This adoption may further decline due to the low willingness to pay for digital health technologies even among patients in urban areas. 27 This reluctance stems from the perception that the government should provide free apps besides lacking awareness regarding the existence and benefits of the apps. 28 Hence, experts advocate for free apps as a strategy to prompt adoption. 29 Furthermore, the additional costs associated with purchasing new technologies such as Bluetooth-enabled glucometers, which are more expensive could deter app adoption. 30 For successful implementation of digital health interventions, these new technologies must be affordable and accessible. 31 This highlights the need for financial incentives targeted at patients such as government-provided reimbursements and subsidies to support the adoption and continued use of the app. 32
Social support from family members, friends, and peers motivates patients to try the apps. 33 This is in line with previous research that technical support provided by the family facilitates the patients in app usage. 34 Family members could assist the patients if they encounter any technical difficulties at home and reinforce patients’ memory on how to use the apps. Therefore, family or caretakers should be involved during the counseling sessions to introduce the apps to them. Peer influence through word-of-mouth spread would also improve public understanding of mHealth services, thus increasing their willingness to adopt the apps. 35
This study suggests using rewards as a strategy to motivate patients to initially adopt and consistently use the apps. The proposed rewards for patients include gamification elements to make the app experience engaging. Patients earn points for consistently using the app and demonstrating improvement in adherence and glycemic outcomes. They would receive financial rewards such as vouchers for purchasing test strips, needles, and alcohol swabs. Moreover, health care professionals play a crucial role by offering motivational praise for patients’ efforts and improvements, further reinforcing positive behavior and adherence. This approach is supported by previous research indicating that gamification and financial incentives effectively improve medication adherence. 36 This could be explained that rewards stimulate patient engagement, fostering a stronger intention to use the apps regularly. 37 They also provide a sense of accomplishment, which encourages continued usage. 38 Similarly, Brower et al 39 found out that even small app incentives such as reward points as little as $0.05 improved app retention rates.
Lack of awareness about the availability of mHealth has been identified as a barrier to app adoption. 40 Education and awareness served as a starting point for integrating app interventions into practice. 41 As proposed, raising awareness could be achieved through marketing efforts. Previous research reported that employing a combination of marketing tools such as social media, printed materials like posters and flyers, and face-to-face communication was effective in promoting apps. The marketing materials should include instructions to guide users through the installation process and navigation of the app from start to finish. 42
Additionally, adoption could be further amplified through the collective effort from health care professionals. This was supported by previous research that suggested health care professionals could introduce and prescribe apps during clinical visits, making patients more aware of the available digital health solutions.29,43 Health care professionals should discuss the benefits with their patients. Digital apps effectively support diabetes self-management and improve glycemic control. 44 As compared with self-recorded blood glucose reading into a booklet by patients themselves, which they often miss or forget to bring to appointments, digital apps offer the advantages of auto-syncing and easy recording. Patients are able to visualize their blood glucose trends and identify potential causes of hypo- or hyperglycemic events. 45 These trends also support health care professionals in making more appropriate and informed clinical and pharmacotherapy decisions. 46
It was worth to notice that although patients were included as study participants, none of the strategies came from the patients’ self-initiative. Patients pointed out the roles of other stakeholders in helping them to enhance their medication adherence and self-management of T2DM through app interventions. However, they were unable to reflect on their own responsibilities and efforts to improve their own health outcomes. This underscores that patient empowerment should be prioritized to foster self-efficacy so that patients proactively participate and engage in their self-management. Medication adherence and confidence grow along with self-efficacy. 47 This could be achieved through extensive and continuous patient education and counseling, focusing on the patient-centered care.
The proposed model provides valuable insights for app developers on the gold standard for a diabetes adherence app. First, it emphasizes the importance of a personalized and user-friendly interface and experience that include multimedia elements such as pictures and colors, adjustable font size, native language options, and easy updates for health records. Additionally, the app should be free and possess high interoperability, seamlessly connecting with devices such as glucometers, blood pressure monitors, and smartwatches. Furthermore, caregivers should be able to receive notifications in cases of non-adherence, hyperglycemic, or hypoglycemic events. The app should also facilitate effective real-time communication between patients and health care professionals, fostering collaborative treatment planning. Incorporating gamification elements is crucial to motivate sustained use and engagement. By integrating these characteristics, the app could provide tailored care and enhance medication adherence for T2DM patients. The authors acknowledge that such an app may not be one-size-fits-all, but it represents a significant step toward the digitalization of adherence and diabetes management.
While integrating all five dimensions of strategies is ideal, the authors recommend a phased approach, targeting the most critical dimension first, which is the environmental dimension. This allows for the gradual incorporation of additional strategies over time to address emerging obstacles, thereby increasing the digital app interventions’ visibility and acceptance among the public. Previous research revealed that perceived usefulness significantly influenced the adoption of digital apps, outweighing perceived ease of use. 13 This indicates that patients are unlikely to use the apps that they do not find beneficial, regardless of how user-friendly they are. Therefore, prioritizing the environmental dimension is essential to address pressing challenges, such as low awareness of the existence and benefits of these apps. Patient education and the efforts of health care professionals should be at the forefront of this initiative. Therefore, enhancing patient awareness about using apps to manage adherence and diabetes through health care professional teams is crucial.
One of the strengths of this study was it involved multiple stakeholders and thus the inputs given were based on their experiences. This study offered a comprehensive set of strategies to raise app adoption for medication adherence and T2DM management, addressing technological, economic, social, behavioral, and environmental dimensions. These proposed strategies need to be implemented to transform knowledge into action. Hence, all stakeholders should work together, aiming toward a sustainable and larger scale of digital app interventions, which ultimately improve health outcomes. The applicability of this model might extend beyond T2DM, meaning that these strategies could be used to enhance digital health solutions among patients with multiple comorbidities, such as cardiovascular diseases and chronic kidney disease, which similarly require complex and long-term medication management.
Nevertheless, there are potential limitations to consider. Although several strategies were proposed, their effectiveness remains uncertain. This warrants future research to determine the effectiveness of the identified strategies through a Delphi approach to seek for expert consensus to inform future decisions on prioritizing and investing in the most agreed-upon strategies for the implementation and scaling of digital app interventions to support T2DM medication adherence and self-management. Another limitation was that although our participants consisted of T2DM patients, no strategies were originating from the patients’ self-effort. Hence, future research should explore the roles of patients themselves to increase app adoption. Given that successful app interventions require government support and thus future research should also include the government’s opinion as they are the policymakers. National-level mHealth policy guidelines should be developed to formally integrate digital app usage into chronic disease management, thereby ensuring consistent and widespread implementation. For example, endorsement from the Ministry of Health could involve integration into routine clinical practice in public primary care clinics and hospitals, along with the provision of educational materials for patients and training programs for health care providers. In addition, future research should explore the best practices in real-world settings by considering the feasibility and implementation in public health care facilities, collaboration between hospitals and clinics with community pharmacies, as well as data ownership and security.
Conclusions
This study provided insights into the strategies to increase the adoption of digital apps for medication adherence and T2DM management, constituting technological, economic, social, behavioral, and environmental dimensions. The proposed model acted as a framework for guiding and structuring national mHealth projects. Successful implementation of these strategies demanded continuous and collaborative efforts from all stakeholders, including app developers, health care professionals, policymakers, and most importantly patients in supporting and establishing future adoption of digital health interventions.
Supplemental Material
sj-docx-1-dst-10.1177_19322968251349851 – Supplemental material for Enhancing Mobile App Adoption for Type 2 Diabetes Mellitus Medication Adherence and Self-Management: A Grounded Theory Study
Supplemental material, sj-docx-1-dst-10.1177_19322968251349851 for Enhancing Mobile App Adoption for Type 2 Diabetes Mellitus Medication Adherence and Self-Management: A Grounded Theory Study by Cheng Jun Chong, Mohd Makmor-Bakry, Ernieda Hatah, Nor Asyikin Mohd Tahir, Norlaila Mustafa, Francis R. Capule and Andi Hermansyah in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
The authors wish to extend their gratitude to the study participants for their valuable contributions.
Abbreviations
DMTAC, Diabetes Medication Therapy Adherence Clinic; HbA1c, glycated hemoglobin; mHealth, mobile health; SMBG, self-monitoring of blood glucose; SRQR, standards for reporting qualitative research; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank Universiti Kebangsaan Malaysia for the support of this project through the University Research Grant GUP-2021-008.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.