
Abstract
Background:
Ongoing support is critical to diabetes self-management education and support (DSMES) effectiveness, but difficult to realize, particularly in areas with limited resources. The objective of this feasibility study was to assess the impact of a virtual support model on diabetes outcomes and acceptability with high-risk patients with type 2 diabetes in a rural community.
Methods:
In a 12-month nonrandomized trial in federally qualified health centers (FQHCs), patients with hemoglobin A1c (HbA1c) >9% were referred to the Telemedicine for Reach, Education, Access, Treatment, and Ongoing Support (TREAT-ON) program where a Diabetes Care and Education Specialist provided DSMES through videoconferencing. HbA1c change was compared in 30 patients in the intervention group (IG) to a propensity score-matched retrospective control group (CG) of patients who received in-person DSMES delivered by a DCES. Changes in HbA1c, diabetes distress, empowerment, self-care and acceptability were assessed within the intervention group (IG) between those who did and did not meet self-management goals.
Results:
The IG experienced similar significant reductions in HbA1c as the CG. Most (64%) IG participants achieved their self-management goal. Goal attainers had a significant HbA1c decrease of 0.21% every 3 months as well as significant reduction in diabetes distress and improvement in general dietary intake. Regardless of goal attainment, IG participants reported high levels of acceptability with TREAT-ON.
Conclusions:
This feasibility study suggests that TREAT-ON was well-received and as effective as traditional in-person DSMES. While findings augment ample evidence regarding DSMES benefits, the TREAT-ON model offers additional advantages and provides validation for telehealth to inform future practice in reaching and supporting self-management for high-risk patients in underserved areas.
Trial Registration:
Clinicaltrials.gov, # NCT04107935.
Background
Despite increasing availability of effective medical therapies, many patients with diabetes mellitus are unable to meet treatment goals. This unfortunate reality is often due to limited access to specialty services and outdated models of care.1 -4 This is particularly more pronounced in rural communities where it is not uncommon for these areas to be medically underserved. Residents of rural communities suffer from a disproportionate burden of diabetes, while reportedly not receiving the same number and type of chronic services as their urban counterparts. 5 The number of physicians per 10,000 people is approximately 30% lower in rural communities than in urban areas 6 and travel to an urban center is often required for specialist services. 5 While modern diabetes care supports the superiority of a team approach over that delivered by a single provider,4,7,8,9 such care is often unavailable.
To solve the problem of limited access to team-based care consultation and diabetes self-management education (DSME), the
Diabetes is a unique disease in that it requires complex self-management, frequent monitoring, making daily decisions, and multiple medication adjustments to achieve treatment goals. There is ample evidence that demonstrates the value of DSMES delivered by a DCES4,7 -9 however, the benefits are reported to wane over time. 14 For patients to sustain a lifetime of behavior to effectively self-manage, ongoing support, defined as resources which help to sustain the ongoing skills, knowledge and behaviors are needed to manage the condition beyond DSME. 15 Delivering this service can be challenging, particularly in hard to reach rural communities. To address the need for ongoing self-management support, the TREAT-ON (ongoing) intervention was developed based on the tested TREAT video-conferencing approach. TREAT-ON was designed to provide DSMES access to individuals living in underserved rural communities.
The objectives of this feasibility study were to (1) determine if individuals with T2DM who participate in the TREAT-ON experience improved glycemic targets as compared with in-person DSMES, (2) examine the impact of TREAT-ON on individual-level behavioral and psychosocial outcomes that are necessary for optimal self-management, and (3) assess the model’s viability in terms of acceptability to inform future testing of the scalability of TREAT-ON.
Methods
Study Design and Setting
This was a 12-month nonrandomized trial that evaluated TREAT-ON prospectively and compared it to a retrospective in-person DSMES program. Both programs were offered at FQHCs providing care to mostly medically underserved, underinsured and uninsured in rural communities located across three of the most distressed counties in Western Pennsylvania. The University of Pittsburgh Medical Center (UPMC) services extend across the region, and based on UPMC Health Plan data, approximately 1,300 adult patient-members with T2DM received care at the participating FQHCs (58% female, mean age 58 years, >75% Medicare/Medicaid) at the time of the study. The FQHCs were chosen because they offered the UPMC Health Plan’s Diabetes High Risk Initiative, an insurer-based DSMES program, to patient-members with a diagnosis of T2DM and considered to be at “high risk” for diabetes-related problems. 16 The purpose of this study was to compare TREAT-ON, an enhanced telehealth version of the Diabetes High Risk Initiative, to matched controls who had already completed the Diabetes High Risk Initiative in person. This study was approved by the University of Pittsburgh’s Institutional Review Board.
Models for DSMES
The original Diabetes High Risk Program: The DCES-driven Diabetes High Risk Initiative 16 was designed to address key components that have been shown to improve quality outcomes in primary care that include, population health, self-management, and coordinated team care. 1 A DCES proactively identified high-risk patient-members and provided in-person DSMES. Patients were identified through the insurer’s population health reports, which are routinely generated and reviewed to allow for proactive identification of individuals who may benefit from supplemented chronic care management. The DCES created a referral for DSMES to patients considered to be at high risk for diabetes-related problems who met the following criteria: diabetes-related emergency room visit or hospitalization, HbA1c >9%, and reported barriers to care. Barriers to care included lack of access to care because of transportation problems, cost barriers due to difficulty in affording medications and supplies, and challenges with comprehension of a care plan due to deficits in knowledge about diabetes or general health literacy. Treatment ranged from chart review and plan of care with medication recommendations to the primary care provider (PCP) to telephone-based or in-person individualized DSMES sessions with patients, depending on patient needs and preferences. The DSMES sessions were in keeping with the assessment and content presented in the National Standards for DSMES. 17
The TREAT-ON Model: TREAT-ON (Figure 1) is an enhancement of the Diabetes High Risk Initiative with the addition of real-time telemedicine videoconferencing to allow remote access to self-management support within the privacy of a patient’s home (or location of their choosing). Recognizing that rural communities experience challenges with Internet connectivity that could preclude participation, we learned that 96.5% of the population in the area, where the study was conducted, was reported to have broadband connectivity.
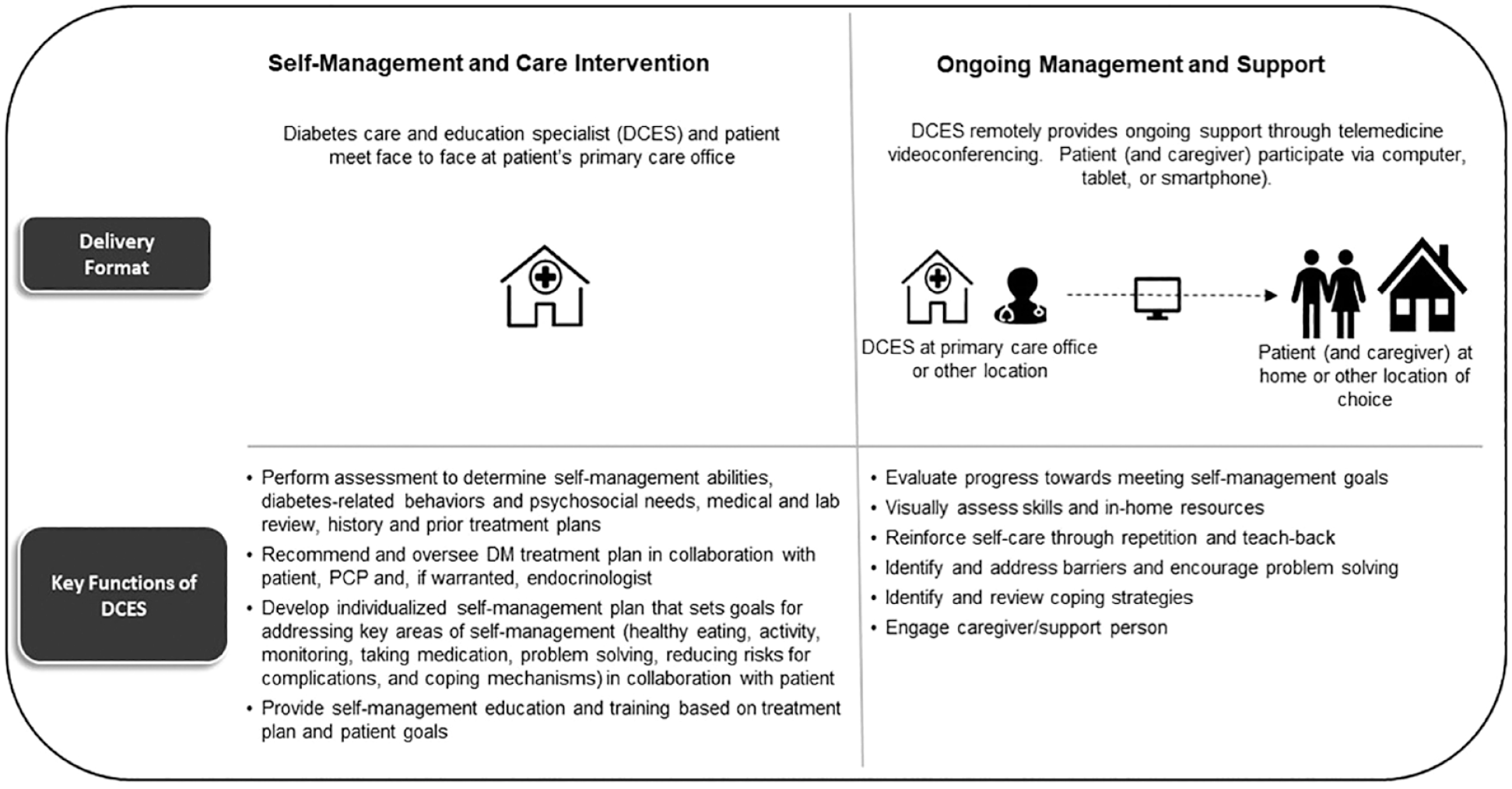
Overview of TREAT-ON model of care.
The DSMES intervention was initiated by the DCES where a comprehensive assessment (review of clinical needs, history, psychosocial needs and barriers, current therapy, nutrition, activity, risk factors, coping strategies, problem-solving skills, with attention to health literacy and cultural influences) was conducted. 18 Based on the assessment, the DCES collaborated with the patient (and PCP) to establish an individualized treatment plan with medication recommendations and self-management goal(s), as well as provide DSMES. Building on this, ongoing management and support was delivered to the patient (and their caregiver if invited) via videoconferencing. As part of ongoing support, the DCES was available upon need and request to the patient over the 12-month period, the DCES had the opportunity to assess an individual’s progress toward meeting their self-management goals, address challenges and barriers that may be impeding progress, and reinforce self-care behaviors, problem-solving-skills and coping strategies. Consistent with the patient empowerment-oriented approach, a patient-centered model tailored to meet the patient’s needs 18 the DCES collaborated with the patient to determine content for discussion, number, length and frequency of follow-up sessions. Content was in keeping with the National Standards for DSMES. 17
Recruitment, Enrollment, and Training
Study patient participants (n = 42) were identified through the UPMC Health Plan population health reports and were invited to participate by a DCES at a participating FQHC if the individual met the “high risk” conditions. 16 Participating patients were consented and introduced to the TREAT-ON model and familiarized with the telemedicine videoconferencing technology by the DCES and health system’s technology staff.
Outcome Measures
Data were collected at baseline and 3, 6, and 12 months for all outcome measures. HbA1c served as the primary outcome and clinical measure of improved DM management. HbA1c values were obtained from the patient’s medical record. Behavioral and psychosocial outcomes were assessed with the following validated self-report instruments:
Self-care behavior
The Summary of Diabetes Self-care Activities Measure (SDSCA) evaluates self-care related to diet, exercise, blood glucose testing, foot care, and smoking. Correlations with other measures of diet and exercise generally support validity of SDSCA subscales. 19
Diabetes distress
The 17-item Diabetes Distress Scale (DDS17) assesses four dimensions of distress—emotional, regimen, interpersonal, and physician, and has shown a consistent pattern of relationships with HbA1c, diabetes self-efficacy, diet and physical activity in multiple samples of patients with T2DM.20,21
Empowerment
The eight-item diabetes Empowerment Scale–Short Form (DES-SF) measures an individual’s perceived ability to manage psychosocial aspects of diabetes, assess dissatisfaction, and readiness to change self-management plan and set and achieve diabetes goals.22,23
Acceptability
The Telehealth Usability Questionnaire (TUQ) is designed to assess telehealth usefulness, ease of use and learnability, interface quality, interaction quality, reliability, and satisfaction. 24
Analyses
A control group was selected from individuals who had previously participated in the Diabetes High Risk Initiative. Propensity score matching was used to form pairs of intervention and control participants. Specifically, a greedy matching procedure with a matching caliper of 0.2 of the standard deviation of the logit of the propensity score was used to create pairs.25,26 For a participant in the intervention group, the closest control participant within the specified caliper distance was selected for matching. Factors selected a priori for inclusion in the propensity score included several covariates known to be possible correlates of HbA1c: race (white and non-white), ethnicity, age, body mass index (BMI), baseline HbA1c, and gender. Standardized mean differences were then calculated to examine the balance between the two exposure groups. Variables with standard mean differences <0.1 were considered to be balanced.
Baseline characteristics of the intervention and control group as well as those who met and did not meet their DSMES goal were presented using measures of central tendency (median, interquartile range) for continuous variables and number and percentage for categorical variables. Comparisons were made using the Wilcoxon rank sum and chi-square tests. To examine the change in HbA1c over time, mixed model regression was employed. 27 Since the baseline characteristics achieved a good balance, those variables were not entered into the propensity score matched model.
A secondary analysis, using only the participants in the intervention group (n = 42), was performed to examine the difference in HbA1c and survey scores for self-care, diabetes distress, empowerment, and the TUQ between those that met their DSMES goal versus those that did not. Similar analyses methods were used except the mixed models were adjusted for age, race, BMI, gender. P < .05 was considered significant. All analyses were carried out using SAS 9.4 (Carey Institute Inc).
Results
HbA1c Changes Compared between Study Groups
Using propensity score matching, 30 intervention participants were paired with 30 individuals who had participated in the original, in-person, diabetes high risk initiative. Baseline characteristics for matched variables are shown in Table 1. Using a conditional mixed regression in this propensity score matched sample, both groups had reductions in HbA1c from baseline (P < .0001), but the reduction was not significantly different between groups (P = .9830). The mean HbA1c decrease was 0.14% every 3 months for both the usual care group (95% confidence interval [CI]: −0.2017, −0.0761) and the intervention group (95% CI: −0.2046, −0.0712).
Baseline Characteristics for Matched Variables between Study Groups.
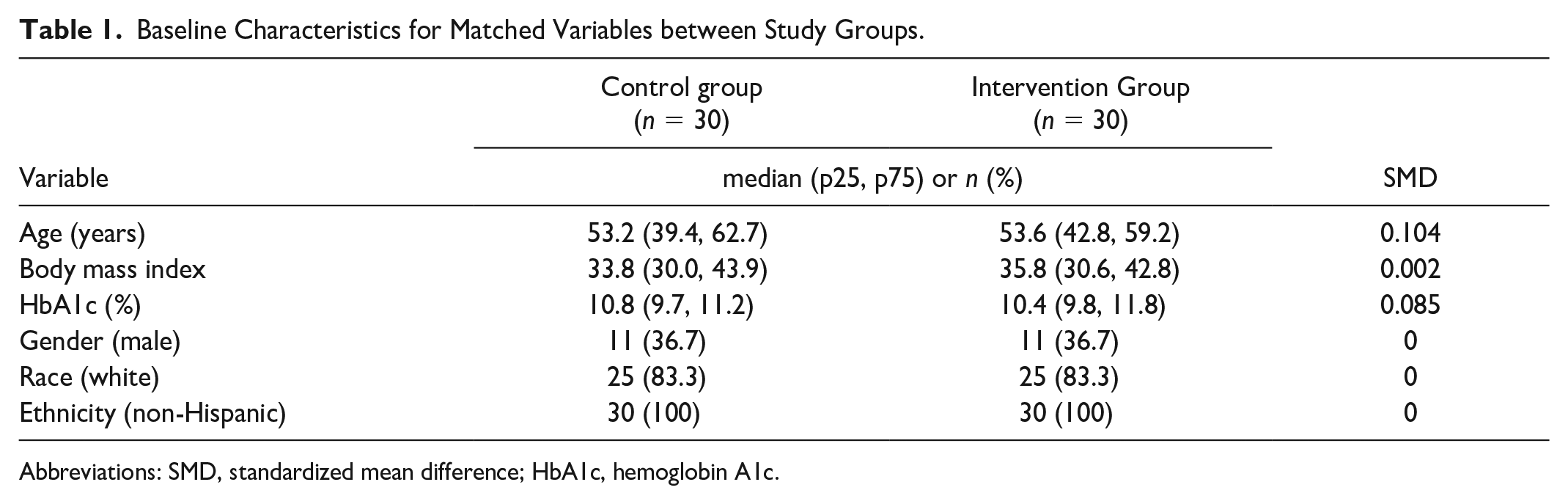
Abbreviations: SMD, standardized mean difference; HbA1c, hemoglobin A1c.
Intervention Within Group Comparisons By Self-Management Goal Attainment
A majority (64%, n = 27/42) of participants in the intervention group achieved their self-management goal. Baseline characteristics of those who did and did not meet their goal are shown in Table 2. Changes in HbA1c, behavioral and psychosocial outcomes were compared between those who did and did not meet their self-management goals. After accounting for age, race, BMI, and time, those that met their self-management goal had a mean HbA1c decrease of 0.21% (95% CI: −0.279, −0.1336)/3 months, as compared with those not meeting their self-management goal who only had a 0.07% reduction in HbA1c/3 months 95% CI: −0.1812, 0.0361). This difference was statistically different between groups (P = .0452), and those who met the goal had a significant decrease in HbA1C from baseline (P < .0001). As shown in Table 3, accounting for the same variables, participants that met their self-management goal had a significant reduction in regimen-related diabetes distress with the associated DDS17 subscale score decreasing 0.07 points/3 months on average (P = .0019; 95% CI: −0.1171, −0.0273). Those that met their self-management goal also had significant improvement in general dietary intake with the associated SDSCA subscale score increasing 0.08 points/3 months on average (P < .05; 95% CI: 0.0006, 0.1563). No other significant within or between goal group differences were found for other behavioral and psychosocial measures.
Baseline Characteristics of Intervention Group Compared by Self-Management Goal Attainment.
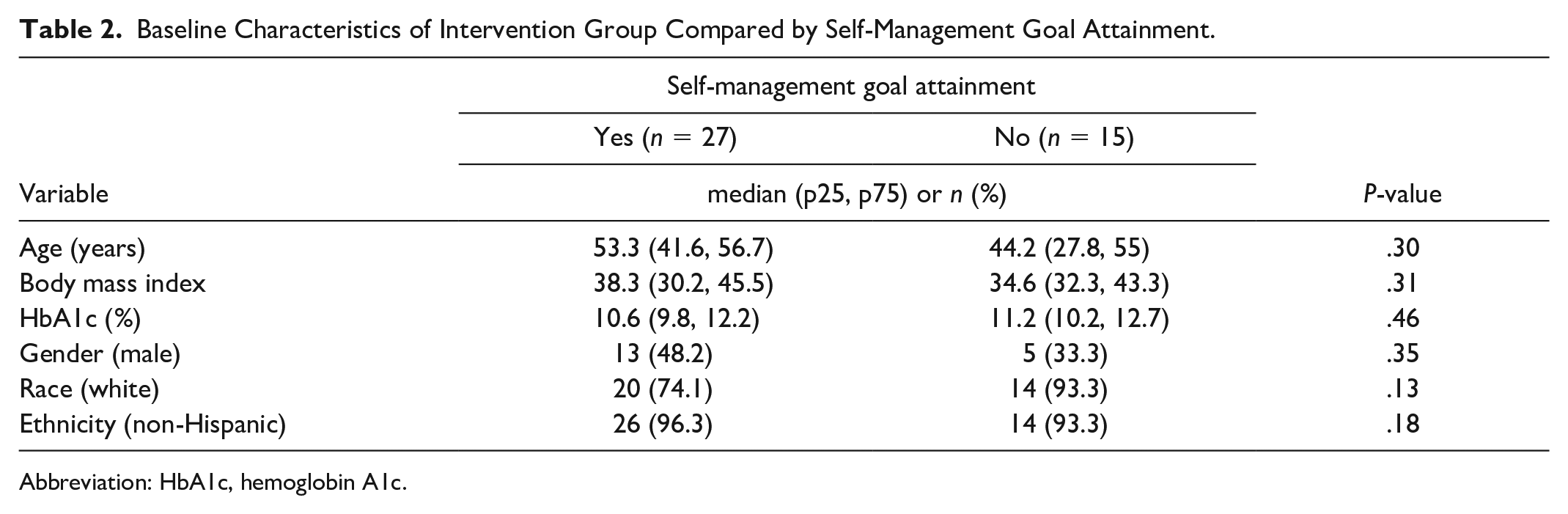
Abbreviation: HbA1c, hemoglobin A1c.
Psychosocial and Behavioral Measures Compared Between Intervention Participants By DSMES Goal Attainment.
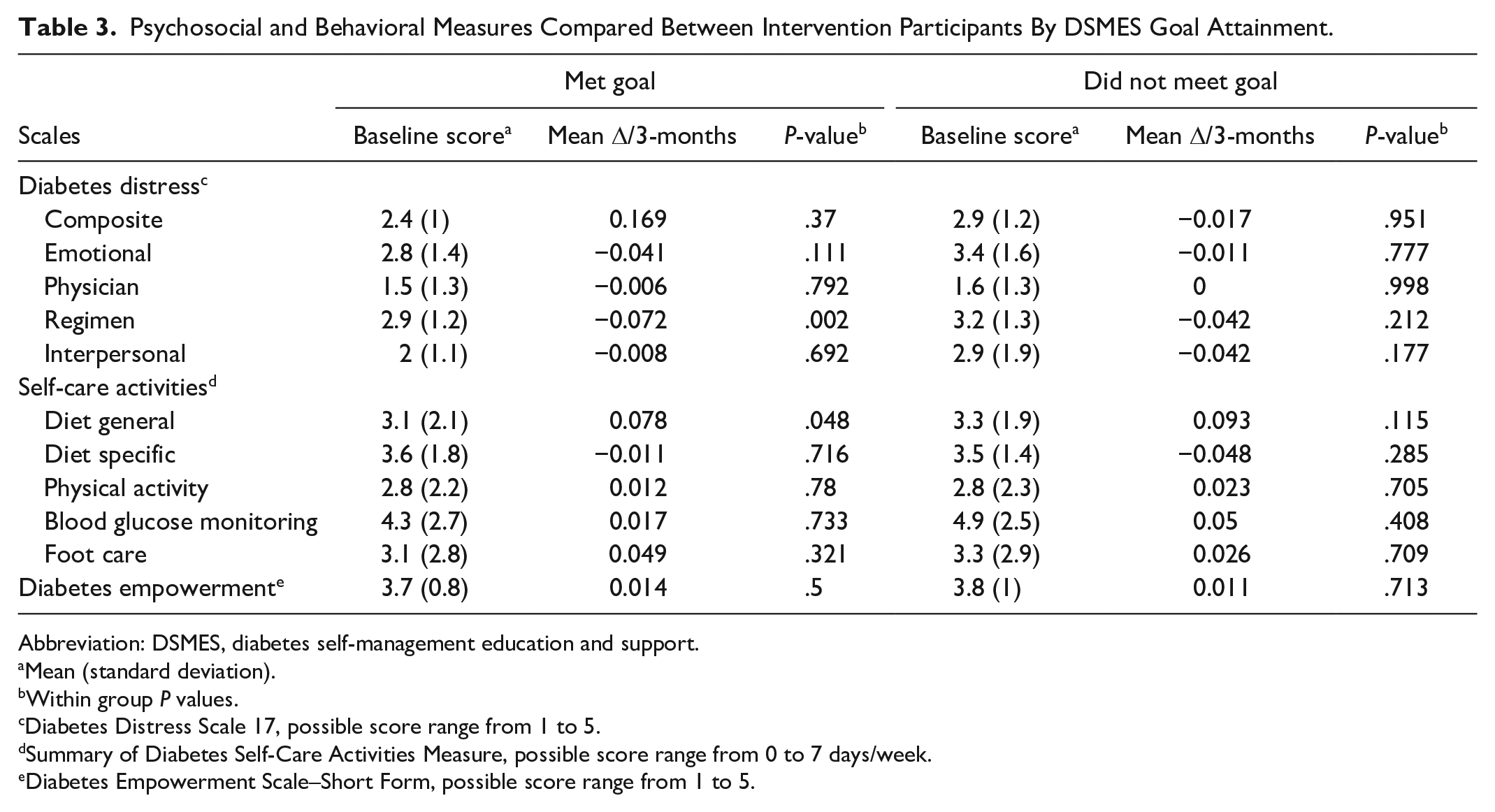
Abbreviation: DSMES, diabetes self-management education and support.
Mean (standard deviation).
Within group P values.
Diabetes Distress Scale 17, possible score range from 1 to 5.
Summary of Diabetes Self-Care Activities Measure, possible score range from 0 to 7 days/week.
Diabetes Empowerment Scale–Short Form, possible score range from 1 to 5.
Intervention Acceptability
Regardless of DSMES goal attainment, participants reported high levels of acceptability with the intervention. Rated by 40/42 intervention participants at 3 months, the average total score on the TUQ was 4.5/5 points with similar high scores for the subscales: usefulness (4.5/5), ease of use (4.5/5), interface quality (4.5/5), interaction quality (4.6/5), reliability (4.2/5), and satisfaction/future use (4.6/5). Intervention acceptability was maintained across the evaluation period with no significant changes in the score values over time or between DSMES goal attainment groups, with the average final 12-month ratings of the TUQ by 38/42 of the sample as 4.3/5 points for total score, (4.4/5), ease of use (4.4/5), interface quality (4.4/5), interaction quality (4.4/5), reliability (4.2/5), and satisfaction/future use (4.6/5).
Discussion
To our knowledge, TREAT-ON is the first study designed to specifically examine the use of a video-conferencing approach to deliver diabetes self-management support. This feasibility study found that the TREAT-ON intervention was well-received and suggests that it may be as effective as traditional in-person DSMES visits with significant improvements in HbA1c in patients with T2DM identified to be at high risk for diabetes-related complications, living in a rural community. In addition, when examining a key component of the DSMES process, those patients in the TREAT-ON group who achieved their personal self-management goal, developed in collaboration with the DCES, were also found to have experienced significant reductions in distress related to regimen adherence and self-care improvements in general diet behavior.
Access to quality health services has been identified as the single most important health priority for the decade in a Healthy People 2020 rural health survey. 28 While DSMES is recognized as a critical component of care, providing DSMES and the necessary ongoing support is particularly problematic in rural communities where there is limited access to specialty care services. The rural landscape also causes challenges for providers in delivering care in areas that often encompass large geographic expanses that require added traveling. These issues add to health care costs and travel time which could be better utilized toward patient care. In a team-based telemedicine consultation to veterans with T2DM in rural communities, clinical outcomes were shown to be comparable to “live” visits. Added “value” was discovered in that the telehealth visits resulted in veteran travel-related savings of $179±123, 431 miles, and 9.4 hours as compared with the costs of veteran’s in-person visits at $66±71; 159±171 miles, and 3.5±4 hours. 29 Similarly, the TREAT-ON model was shown to be just as effective as in person DSMES with the added benefit of offering a time and cost-effective approach. When traditional in person visits were compared with the telehealth model, a lower average cost per patient was noted ($38.85 vs $6.20) along with lower average travel time (99 min vs 16 min). The TREAT-ON model translated to a direct cost savings of $1606 and a reduction of DCES travel time to DSMES sites of 67.6 hours equating to a gain of 8.4 workdays opening care opportunities for an additional 67 new DSMES referrals. 30
The Centers for Medicare Services (CMS) reported that seeking efforts to reduce barriers to promote telehealth to improve access to care for the estimated 60 million Americans living in rural and underserved communities is needed. 31 Considering the critical importance of DSMES in diabetes care and the national shortage of DCES, opportunities to reach patients through telehealth looks to be a viable option. Health systems, insurers and diabetes organizations need to continue to examine methodologies for team-based approaches that include DSMES in telemedicine delivery. This is especially important now as the COVID-19 pandemic has forced health systems to rapidly convert to telecare where use increased 300-fold in 2020 in the United States, 32 with diabetes as the fourth most common diagnosis for telemedicine visits. 33 However, components considered to be essential for high-quality diabetes care have been reported to be inconsistently available in telemedicine visits, including coordinated access to multidisciplinary teams, home blood glucose monitoring results, and vital signs.34 -37 In a recent study of patients who received subspecialty diabetes care, overall, the most cited reasons among both adult patients and caretakers of pediatric patients were a limited familiarity with technology or lack of smartphone access. 38 Other reasons included language barriers, providing lab test results, needing to provide insulin pump data in-person, and forgetting that the appointment was supposed to be a video visit. 38 To maximize benefits of telemedicine for patients with diabetes who are not meeting treatment goals, we first need to address these shortfalls. While the rapid deployment of telemedicine presented some challenges, it also opened the door to examination of an innovative delivery system. For example, data on 6.8 million employer-based health plan beneficiaries in 2020 and 2019, a 20-fold increase in the incidence of telemedicine utilization was observed. 32 The increase in telemedicine was greatest among patients in counties with low poverty levels, supporting the case for telehealth delivery to disadvantaged rural areas. 32
While we found that virtual visits provide DSMES access to people with T2DM in a rural community, limitations of this feasibility study must be taken into consideration when interpreting findings. First and foremost, the study was implemented at the very start of the COVID-19 pandemic when we had intended to recruit 50 patients into the study. When in-person visits were limited by the pandemic, patients had little choice in accepting virtual visits and its associated new challenges. For example, it limited opportunities for in-person contact to introduce and train patients on the intervention. In addition, it caused challenges in obtaining relevant clinical data, like HbA1c, blood pressures and weights, thereby causing some missing values for all the defined time points. In addition, our study design included a historic control group that was chosen for the initial testing of TREAT-ON to make best use of available resources. However, because of the finite number of patients in the high-risk database, the propensity score matching for the control group, while well matched, was only able to pair 30 with the 42 participants in the intervention group. Furthermore, although a retrospective versus parallel control group design was chosen for initial testing of TREAT-ON, it also prevented the ability for collecting behavioral psychosocial and satisfaction data for the control group.
Despite the limitations in this feasibility study, the TREAT-ON model provided an opportunity to reach patients, improve and sustain their diabetes outcomes who live in underserved areas unlikely to receive DSMES services. While requiring further study, we did have the added opportunity to discover the unique advantages for DSMES delivery, including the ability to easily engage with patients’ family and caregivers, obtain insight into patients’ environment and health habits, remotely share home monitoring data, and opportunities to facilitate more frequent follow-up and care coordination for patients who require intensive care to meet diabetes treatment goals.37,39 -41
Conclusions
This study contributes to the evidence of the value of virtual DSMES to improve diabetes behaviors and outcomes. While the diabetes community continues to advocate for increasing the number of people who receive DSMES, efforts to explore and support delivery via technology is vitally important.
Footnotes
Acknowledgements
The authors thank the patients and providers who participated in this study. The authors also thank the research team members, especially Shari Reynolds, for their contribution to this study.
Abbreviations
CI, confidence interval; CMS, Centers for Medicare Services; DCES, diabetes care and education specialist; DDS17, Diabetes Distress Scale 17; DES-SF, Diabetes Empowerment Scale–Short Form; DSMES, diabetes self-management education and support; FQHC, Federally Qualified Health Center; HbA1c, hemoglobin A1c; PCP, primary care provider; PS, propensity score; SDSCA, summary of diabetes self-care activity; TUQ, telehealth usability questionnaire.
Authors’ Note
Prior Presentation: Parts of this study were presented in abstract form at the American Diabetes Association’s Scientific Sessions in 2021 and 2022.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LS, JK, and JN had research support from Becton, Dickinson and Company, and Sanofi, Inc. LS also served on the Bayer Advisory Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work represents research supported by the NIDDK of the NIH under award number R34DK123370.