
Abstract
Background:
Previous research has identified that people with type 2 diabetes (T2D) within the Hispanic community would benefit from an online peer support community (OPSC) and continuous glucose monitoring (CGM) data to facilitate diabetes self-management.
Methods:
A mixed-methods feasibility study enrolled Hispanic, Spanish-speaking adults with T2D, not on insulin. Participants were provided with CGM and access to an OPSC for 12 weeks. Feasibility was assessed by number of eligible participants who enrolled, attrition, quantity of CGM data, validated clinical measures of self-efficacy, quality of life and adverse events. Engagement in the OPSC was measured using objective metrics on the online platform. Qualitative interviews were conducted upon conclusion of the intervention to assess feasibility, acceptability, participant satisfaction, and key recommendations for improvement.
Results:
Of 46 participants screened, 39 were eligible and 26 completed the study. Participants significantly improved self-efficacy scores. Posts in the OPSC related to goal setting had the highest engagement followed by mid-week and end of week check-in posts respectively. Participant interviews described challenges accessing the OPSC platform as a barrier to engagement. Despite this, all participants were satisfied with the intervention. Key recommendations for improvement included providing greater variety of and individualized education and the use of a peer support platform that is easily accessible.
Conclusions:
The CGM + OPSC intervention tailored to the Hispanic community with T2D was feasible, acceptable and satisfactory and improved participant self-efficacy for diabetes management which may lead to improved clinical outcomes.
Introduction
Type 2 diabetes (T2D) is more prevalent in the Hispanic community (12.5%) compared to non-Hispanic white counterparts (7.5%), 1 and A1C levels are significantly worse. 2 Individuals from racially and ethnically diverse communities often have less access to resources for engaging in diabetes self-management education and support (DSMES) and for using diabetes technology.
Continuous glucose monitoring (CGM) has been shown to lower A1C compared to blood glucose monitoring (BGM) in people with T2D who use insulin.3,4 Evidence of benefits of CGM for those who do not use insulin is emerging 5 and use has been addressed in the American Diabetes Association Standards of Care. 6 Among those not using insulin, CGM can reduce A1C for up to 9 months 7 and can foster health behavior changes that can delay the need for insulin in T2D.8,9 However, CGM insurance coverage is limited for those not using insulin.
Most CGM research in T2D does not represent populations who are racially and ethnically diverse, have lower socioeconomic and education status, or lack health insurance. Well-documented CGM disparities in children and young adults with type 1 diabetes 10 are heightened in diverse populations with lower socioeconomic status. 11 Data from the T1D Exchange show that regardless of age, socioeconomic status, race/ethnicity or income, CGM users have lower A1C levels. 12 CGM use in diverse populations with T2D may improve outcomes; optimizing CGM implementation and use would require robust diabetes education, training, and support, 6 and decreasing disparities in diabetes technology use. One innovative opportunity for CGM education and support is engagement in online peer support communities.
Diabetes online peer support communities (OPSC) have shown improved clinical, behavioral, and psychosocial outcomes. 13 Racially and ethnically diverse populations benefit from diabetes-related in-person and telephone-mediated peer support, 14 but are typically under-represented in OPSC. In a review of 47 studies, people who engage in OPSC reported increased confidence in managing diabetes, increased resilience in facing diabetes challenges, and overall feelings of not being alone. 13 Research in the use of OPSC in the Hispanic population has been limited.
Our previous PCORI-funded work with community stakeholders highlighted the insufficiency of diabetes self-management education alone, 15 and identified the need for Hispanic individuals with T2D to have access to ongoing diabetes-specific peer support and CGM technology in Spanish. 16 Through community-based participatory research practices and a community advisory board, stakeholders agreed it was critical to design an intervention that provided access to CGM in Spanish so participants can learn about glycemic patterns, and to provide ongoing support through easy access to OPSC with Spanish-speaking peers also living with diabetes. This study assesses the feasibility, acceptability, and satisfaction of a CGM + OPSC intervention and reports key recommendations to improve the intervention.
Methods
Design
We used mixed methods to conduct a feasibility study of a CGM + OPSC intervention in Hispanic, Spanish-speaking adults with T2D who do not use insulin.
Setting
Data collection took place in the community. Participants were recruited by bilingual community health workers in a mountain-state urban area via Spanish radio ads and flyers at events frequented by Hispanic individuals, then contacted and consented by a bilingual research assistant, from December 2019 to March 2020. Two significant unforeseen events occurred during the study: the COVID-19 pandemic shutdown on March 13, 2020; less than a week later, a 5.7 magnitude earthquake with extended aftershocks, impacting where most participants resided.
Intervention Description
Participants used a CGM (Freestyle Libre 14-day system, Abbott Diabetes) equipped with a Spanish language reader to scan glucose levels at least every 8 hours. Beyond Type 2 en Español (previously EsTuDiabetes)—a well-established Spanish-language OPSC—served as the OPSC platform. Participants wore a professional (blinded) CGM for 1 week to establish baseline, then concurrently used personal CGM and the OPSC for 12 weeks, with no additional DSMES. Lost sensors were replaced. All CGM data were downloaded at the end of the study.
The OPSC was moderated by 5 bilingual, trained peer facilitators with diabetes and expertise in CGM and OPSC use. Peer facilitators encouraged discussions around the ADCES7™ Self-Care Behaviors for diabetes management in response to CGM data. The OPSC included 3 intervention-related posts each week focused on: goal-setting through personal experiments; check-in and troubleshooting goals; and final check-in on goal achievement. Participants were encouraged to engage in the OPSC at least 3 times per week. All communication between participants and peer facilitators were conducted asynchronously via threads within the OPSC. As part of a safety protocol, a Spanish/English bilingual dietitian who was certified as a diabetes care and education specialist reviewed the content within the OPSC every 2 to 3 weeks for accuracy and coached the Peer Facilitators as needed. While the likelihood of hypoglycemia was low, given no participants were using insulin, when participants reported out of range glucose levels, peer facilitators encouraged participants to visit their healthcare providers. Peer facilitators were also instructed to report any concerning posts, such as suicidal behavior, depression, concerning blood glucose levels, and so on.
Participants completed a semi-structured post-intervention interview to document their experiences and provide feedback. We used rolling recruitment; participants started at different timepoints.
Sample
Participants were aged ≥21 years, self-reported as Hispanic, had T2D and were not using insulin, spoke and read Spanish, were willing to wear CGM, had Internet access and were willing to engage in an OPSC, and were willing to avoid daily vitamin C >500 mg and aspirin >325 mg (due to effects on CGM accuracy). Exclusion criteria were: type 1 diabetes; insulin use; use of CGM in the previous 6 months; illness that prevented participation (cognitive impairment, 2 or more hospitalizations in the past year, life expectancy <6 months, alcohol abuse or dependence); pregnancy or plans to become pregnant; concurrent enrollment in another diabetes study.
Data Collection and Analysis
Quantitative Feasibility Outcomes
We examined eligibility, recruitment, retention, reasons for dropout, data capture (eg, number of days CGM worn, completed surveys), and adverse events. For categorical variables, the number and percentage are presented. For continuous variables, the median and quartile are presented.
Qualitative Feasibility Outcomes
Semi-structured post-intervention phone interviews in Spanish used an interview guide (Appendix A) to ensure consistency across interviews. Participants were encouraged to talk about their experiences with CGM+OPSC. Interviews were audio-recorded, translated, transcribed, and checked verbatim for accuracy. The researchers read the transcripts, using a qualitative thematic analysis to a priori code data specific to feasibility, acceptability, satisfaction, and key recommendations to improve the intervention. We defined feasibility as whether implementation of CGM and OPSC use was easily and conveniently achieved, accounting for advantages and disadvantages to integrating both into their day-to-day routine. Acceptability was defined as whether or not participants found CGM and its components likable, and liked the OPSC interface and navigation features. Satisfaction was defined as whether participants liked the study, would like to continue using CGM or the OPSC after the study ended, or would recommend the intervention to others. Key recommendations were categorized as general, CGM-, and OPSC-specific.
Clinical and Patient-Reported Outcomes
Demographics and health history were collected at baseline. Time-in-Range (TIR) (primary clinical outcome) was collected at baseline and at 12 weeks. Secondary outcomes included A1C and patient-reported outcomes: self-efficacy 17 and quality of life (WHO-5 18 ), collected at baseline and 12 weeks. Inferential statistics for nominal variables utilized Fisher’s exact test; most ordinal and continuous measures were evaluated using non-parametric Mann Whitney U for between-group and Wilcoxon Sign Rank tests for within-group comparisons.
Online Peer Support Community Engagement
OPSC engagement was measured through objective online forum metrics (number of days an individual visited, number of threads visited, number of comments made, time spent reading, and how many likes and comments received). Participation engagement was defined as 3 or more posts per active participant per day. Participants received a daily email summary of new OPSC posts. We could only collect metrics within the forum, so could not track reading of the email digest.
Results
Feasibility, Demographic, and Clinical Characteristics
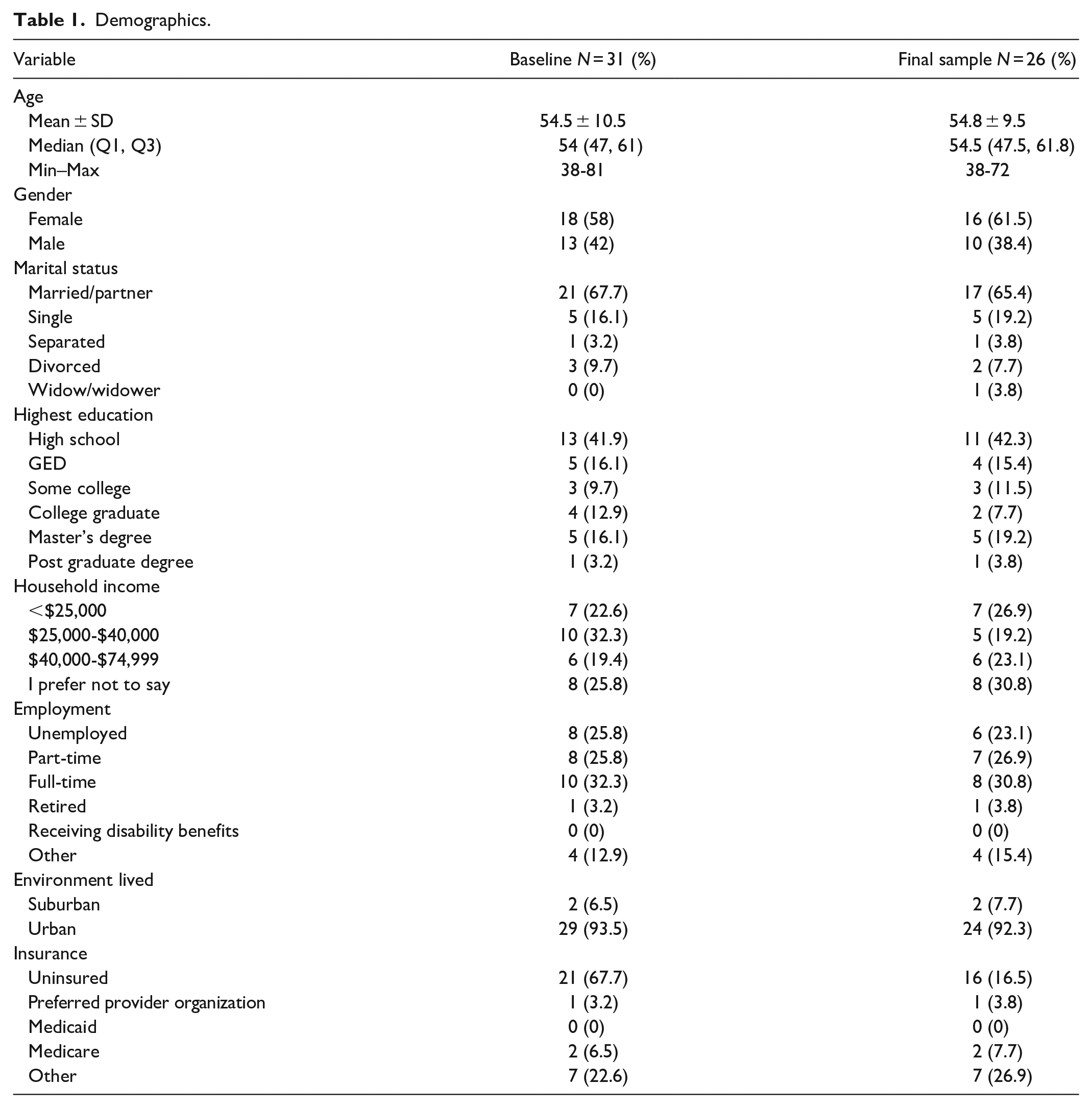
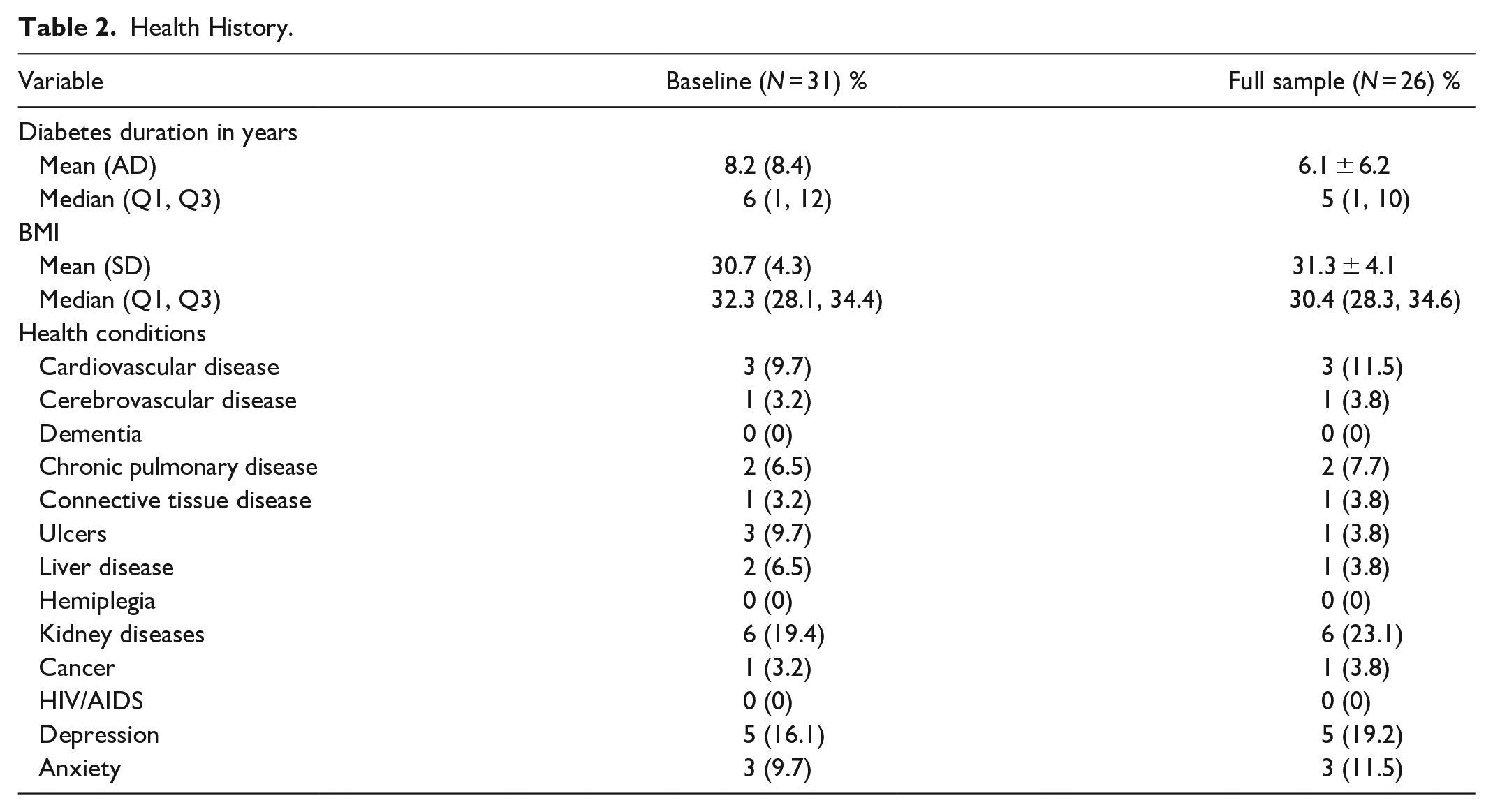
We identified 39 eligible participants of 46 recruits screened. Of the 34 who consented, 31 completed all baseline components and 26 completed the study, for a retention rate of 76.5%. Eight participants (4 males, 4 females) discontinued the study. See Figure 1 for details. All participants were Spanish-speaking and self-identified as Hispanic or Latino. Table 1 describes demographics and medical history for all participants, stratified by gender. The majority had a high school education or GED (56.4%), were uninsured (67.6%), and reported a household income of <$35,000 (56%). Table 2 lists comorbid conditions and complications.
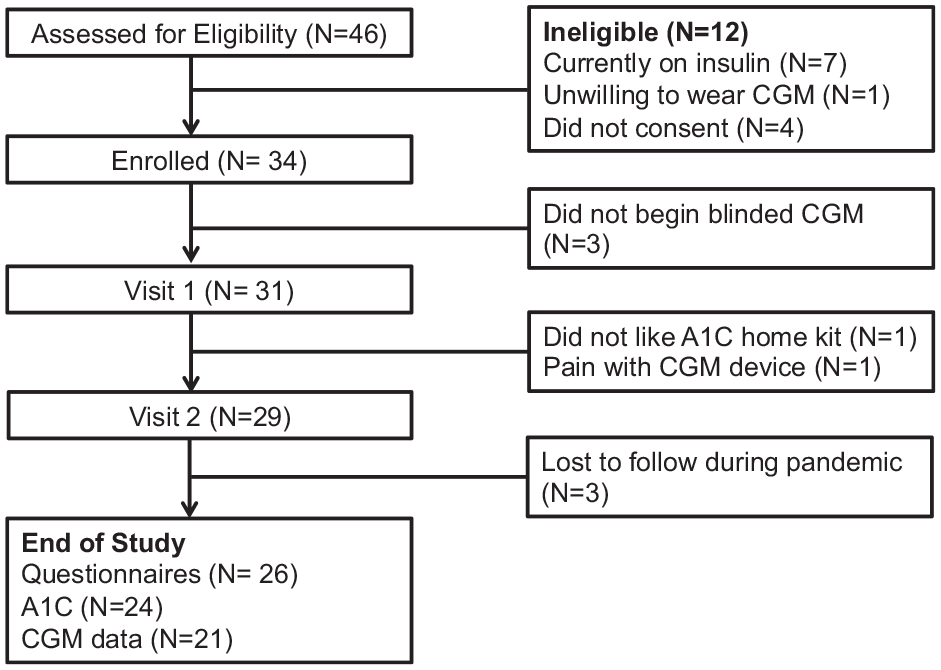
CONSORT diagram.
Demographics.
Health History.
Continuous Glucose Monitoring
Baseline CGM was completed by 31 participants. Twenty-one participants (67.7%) returned the device for download at 12 weeks. Females were slightly more likely to continue wearing CGM through 12 weeks (72.2%, 13/18) compared to males (61.5%, 8/13). Including baseline data, participants had median 91 recorded days (Q1 = 15, Q3 = 98). Median scans at 12 weeks were 3 per day (Q1 = 4, Q3 = 6), consistently throughout the study. TIR was a median of 89% (44, 97) at baseline and 82% (63, 87) at 12 weeks. There were no statistically significant differences in median TIR or median glucose levels between baseline and 12 weeks. A statistically significant increase in glycemic variability coefficient of variation was observed; Wilcoxon sign rank test, Z = −2.172, p = 0.03 (see Table 3).
A1C and Continuous Glucose Monitoring Outcomes.
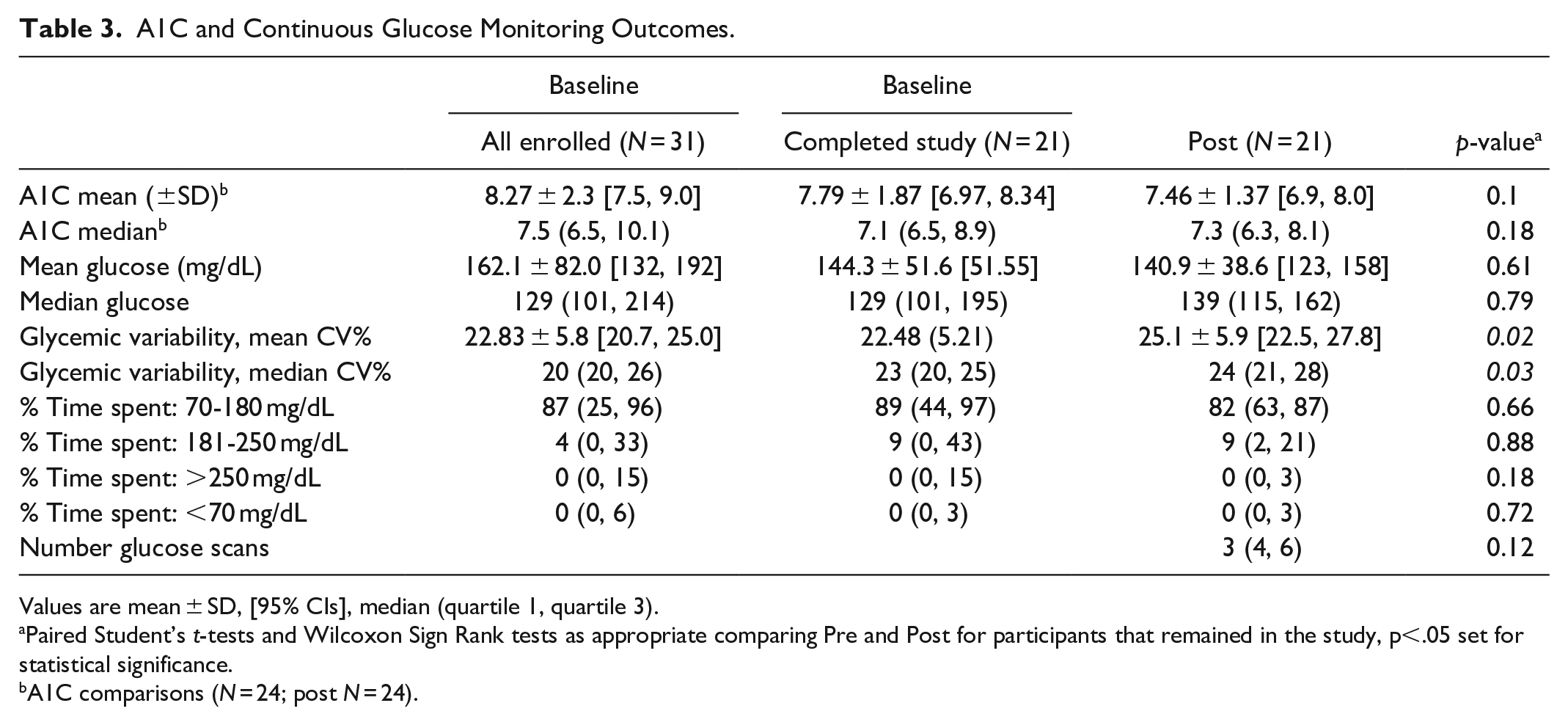
Values are mean ± SD, [95% CIs], median (quartile 1, quartile 3).
Paired Student’s t-tests and Wilcoxon Sign Rank tests as appropriate comparing Pre and Post for participants that remained in the study, p<.05 set for statistical significance.
A1C comparisons (N = 24; post N = 24).
A1C
A1C was completed at 12 weeks by 24 of 31 participants (77.4%). Individuals who discontinued participation had a higher baseline A1C (N = 5, Median = 11.7%; Q1 = 7.6, Q3 = 13.6) versus those who completed the study (N = 26, Median 7.1%; Q1 = 6.5, Q3 = 8.9). As predicted, given our small sample size, for those completing the study there was no statistically significant change between baseline (N = 24, M = 7.8% ± 1.9) and 12 weeks (N = 24, M = 7.5 ± 1.4; p = 0.10). Nine participants had a clinically meaningful 12-week decrease in A1C (≥−0.5%), 5 had a clinically meaningful increase (≥+0.5%), and 10 had no clinically meaningful change (±0.4%).
Patient-Reported Outcomes
Self-Efficacy
Cronbach’s alpha was 0.82. Mean self-efficacy increased significantly from baseline (N = 26, M = 68.6 ± 18.3) to 12 weeks (N = 26, M = 82.7 ± 14.5; p < 0.01). Interestingly, baseline self-efficacy was greater for males (N = 10, M = 78.4 ± 9.4) compared to females (N = 16, M = 62.4 ± 20.1; p = .012). The 5 participants who discontinued tended lower on self-efficacy (Median = 57.0; Q1 = 43.4, Q3 = 79.9) than those who completed the study (Median = 72.2; Q1 = 57.1, Q3 = 82.9).
Quality of Life
Cronbach’s alpha was 0.85. There was no significant difference in QOL score at baseline (N = 26, M = 15.1 ± 5.6) compared to 12 weeks (N = 26, M = 16.7 ± 5.1; p = 0.18). For those completing the study, there was no difference in baseline QOL by gender (male N = 10, M = 17.3 ± 5.9), female (N = 16, M = 13.7 ± 5.1; p = 0.112).
Online Peer Support Community Engagement
Within the OPSC, 25 intervention-specific posts related to goal setting: posts focused on setting up a personal experiment generally attracted the most engagement (390 comments), followed by mid-week check-in posts (350 comments), and end-of-the-week check-in posts (230 comments). Twenty-eight original posts (non-study topics) attracting 250 comments were made on a variety of topics, including tips on using CGM, how personal experiments with food and activity impacted CGM readings, sharing healthy recipes, and stress, along with experiences with COVID-19 and the local earthquake. Peer support engagement for participants and facilitators is described in Table 4. The highest rate of OPSC engagement was 61.5%, with 13 participants active within the forum (week of 24th February, on the cusp of the COVID-19 pandemic).
Online Peer Support Community Engagement.
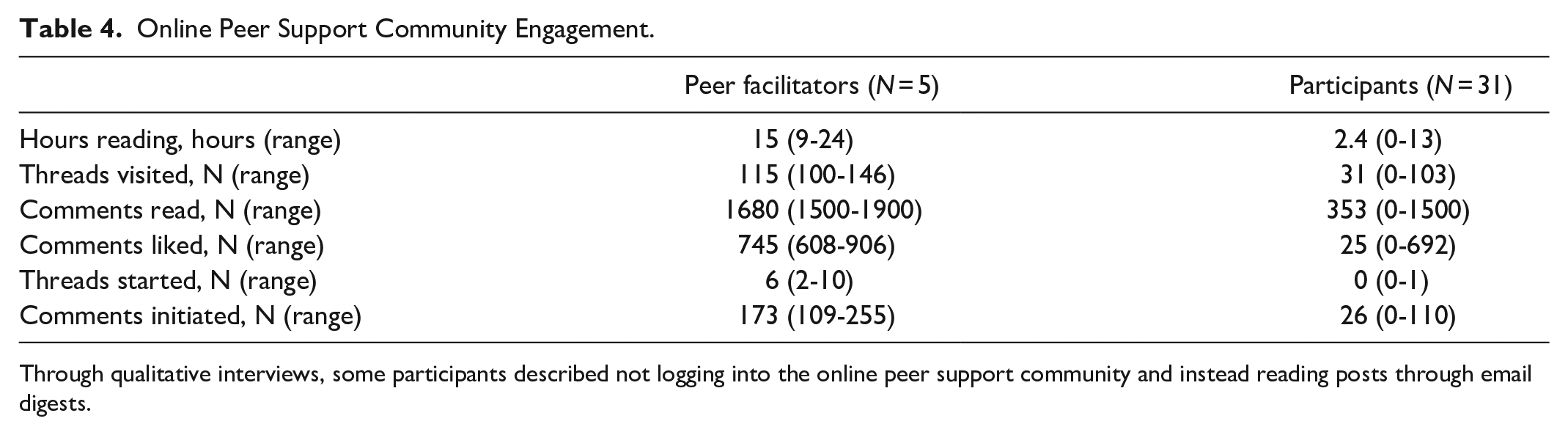
Through qualitative interviews, some participants described not logging into the online peer support community and instead reading posts through email digests.
Interview Results
Twenty-six post-intervention interviews examined feasibility, acceptability, and satisfaction, and gathered key recommendations to improve CGM + OPSC.
Feasibility
Participants found that CGM was easy to wear and use, and could be easily integrated into their regular routines. Wearing CGM did not interfere with day-to-day activities. However, 9 participants reported 14 instances of sensors falling off (1 person reported 5 instances). Sensors fell off during clothing changes, placing/removing a bra, and while wearing/removing a backpack.
Participants liked the personal experiments posted within the OPSC, describing how the challenges sparked them to do new activities they would not have previously thought of (eg, try a new snack to see how it impacts glucose). Participants appreciated the support of the peer facilitators and fellow participants, describing how the OPSC allowed them to vent, obtain new ideas about managing diabetes, and receive social support. Interestingly, the OPSC became a trusted source of information during the COVID-19 pandemic and following the earthquake. A few participants reported social support needs (food, utilities payments, etc.) to the research assistant; in response, we posted a list of resources, in Spanish, for all participants, which was appreciated.
Acceptability
Participants unanimously found CGM preferable to BGM, citing its fingerprick pain and comparative annoyance. Patients favored the ease of scanning the sensor to obtain and visualize their glucose levels and trends. Additionally, they liked being able to scan several times a day, receiving immediate feedback for gauging how different day-to-day behaviors affected glucose levels.
Participants sometimes could not remember where to log into the OPSC, forgot their login handle or password, or had other challenges accessing the OPSC, including backend platform changes. Further, participants noted challenges due to the OPSC website not already being a part of their daily routine. Some participants opted to check the OPSC email digest to review posts because email was already part of their routine and they could obtain the same information, though not post or reply to comments. Participants did not describe a lack of internet access (eg, WIFI) as a challenge.
Satisfaction
All participants (100%) stated they were satisfied with the study and would recommend it to others. Several participants reported going to their local grocery store (Walmart, Sam’s Club) to see if they could purchase CGM so they could continue using it after the study ended. Participants reported the main barrier to using CGM after the study is cost.
The majority of participants were satisfied with the OPSC. There were 2 males who stated they did not need the OPSC for anything other than gathering the personal experiment information. However, while these 2 participants personally did not feel the OPSC was beneficial for them, they could see how other participants benefited. Most stated that they would like to continue using the OPSC after the study ended.
Key Recommendations for Improving the CGM + OPSC Intervention
Generally, some participants were interested in basic diabetes education (e.g., physiology, complications). Some with higher A1C levels desired one-on-one education with a healthcare provider who could provide tailored medical advice.
Specific to CGM, participants recommended more education on how to prevent sensors from falling out. One participant recommended we train on advanced CGM features, such as how to enter the number of carbohydrates consumed or how to navigate trend data over different time periods (e.g., 3-hour, 12-hour, 24-hour).
There were 3 OPSC recommendations. First, use an OPSC platform that is simpler to use in someone’s day-to-day routine (e.g., Facebook, text message, WhatsApp). Second, provide synchronous sessions, including at the start of the study to allow for introductions (video or in person) to differentiate peer facilitators from other participants, and throughout the study to improve overall group dynamics. Third, one participant recommended we explain the personal experiments in simpler terms.
Discussion
To our knowledge, this is the first study to examine CGM + OPSC in Hispanic, Spanish-speaking adults with T2D. Our data indicate that participants found the CGM + OPSC intervention feasible, acceptable, and highly satisfactory. The CGM + OPSC intervention simplified how participants could obtain glucose data, while providing immediate feedback on how health behaviors impacted glucose levels. The OPSC provided personal experiments coupled with an engaged community that provided emotional support on how to carry out personal experiments. The peer facilitators were “cheerleaders” for the participants, encouraging them while also listening to their concerns. As a result, participants achieved higher levels of self-efficacy at 12 weeks. Participants also provided key recommendations that would need to be addressed to optimize the intervention.
Using a bilingual research assistant and community health worker from the community of interest, we were able to successfully recruit participants. We believe our greatest obstacles were retention and obtaining CGM and A1C data remotely in response to the COVID-19 pandemic. As seen across the nation, Hispanic participants were disproportionally impacted by the pandemic. 19 Despite these challenges, we were able to retrieve 21 receivers. We believe that cloud-based CGM data collection will resolve the need to retrieve receivers in the future. Importantly, though the OPSC was designed for diabetes, we were able to provide critical information about COVID-19, the earthquake, and local social support services that address health disparities, increasing participant trust in us as researchers.
Our findings shed light on the interconnectedness of feasibility, acceptance, and satisfaction of a CGM + OPSC intervention. Our goal was to see if such an intervention among participants not on insulin could support health behavior changes. Most participants had minimal DSMES prior to the study; the OPSC provided an opportunity to learn how to self-manage diabetes (recognizing that additional basic diabetes education may be needed). Consistent with self-efficacy theory, 20 the significant improvement in diabetes self-efficacy may indicate that CGM + OPSC provided a strong foundation to engage in personal experiments to support future behavior change. Future research should address our participants’ recommendations to optimize CGM + OPSC.
Technology studies conducted in ethnically and racially diverse adults with T2D are uncommon. Our preliminary findings suggest CGM and OPSC as a combined intervention is feasible and acceptable in a Hispanic and Spanish-speaking population, and can influence positive behavior changes while addressing technology use disparities. Our study indicates Hispanic populations will use CGM, though it must be affordable and accessible: despite our participants’ interest in CGM, they identified cost as a concern for continued use. Two studies7,21 suggest cost-benefits and A1C reduction when providing personal 7 and professional 21 CGM to adults with T2D, cost-effectiveness of CGM use in Hispanic populations are needed. Juxtaposing these findings suggests: efforts should be taken to include ethnically and racially diverse populations in future diabetes technology studies; cost and coverage of CGM for adults with T2D must improve for both clinical and economic reasons, and to avoid widening the existing diabetes technology gap.
This study has several limitations and strengths. The intervention was combined, and therefore the effects of CGM or OPSC alone cannot be determined. We were unable to track lifestyle or medication taking changes that may have affected the measured outcomes. Self-reported data is subject to social desirability bias, so some participants may have exaggerated positive reactions to the intervention. We take many participants seeking out how to continue the intervention beyond the study period as strongly suggesting we have captured an accurate representation of satisfaction. Further, the mixed-method approach to analyzing feasibility data strengthened the credibility of our findings. Transferability of results may be limited to other Hispanic, Spanish-speaking adults and not to other ethnically/racially diverse populations. It is nonetheless a strength that our study recruited participants not typically enrolled in diabetes technology clinical trials. Participants were Hispanic, Spanish-speaking, with low SES, the majority without insurance. Systemic policy changes are needed to improve access to diabetes technologies for racially and ethnically diverse populations. While our sample size was intentionally small in order to establish feasibility, we did identify improvements in self-efficacy, illustrating the value of our CGM + OPSC intervention. Future research should explore effects of CGM + OPSC beyond a 3-month follow-up period, examine CGM trends intermittently throughout the study, and coordinate glucose reporting to the participant’s primary care provider.
Conclusion
CGM and OPSC as a combined intervention hold great promise for overcoming health disparities among Hispanic populations with T2D by bridging a gap in access to glucose data and social support to enhance healthy behaviors. Results of this evaluation may be used to guide future research on the use of CGM+OPSC in diverse populations.
Supplemental Material
sj-pdf-1-dst-10.1177_19322968211032278 – Supplemental material for Combining CGM and an Online Peer Support Community for Hispanic Adults with T2D: A Feasibility Study
Supplemental material, sj-pdf-1-dst-10.1177_19322968211032278 for Combining CGM and an Online Peer Support Community for Hispanic Adults with T2D: A Feasibility Study by Michelle L. Litchman, Ashley Ng, Ana Sanchez-Birkhead, Nancy A. Allen, Bruno Rodriguez-Gonzales, Eli Iacob and Deborah A. Greenwood in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
A special thanks to the Association of Diabetes Care & Education Specialists for donating paraprofessional trainings and to diabetes nonprofit, Beyond Type 1, for hosting the online peer support community platform. We would also like to acknowledge the intervention team, Eugenia Araiza, Lorena Drago, Rebeca Peon, Julissa Rulon, Ruis Santos, and Diana Velo.
Abbreviations
CGM, continuous glucose monitor; OPSC, online peer support community; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Throughout the study period DAG had no conflict of interest, however now is an employee of Dexcom.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is an investigator-initiated study funded by Abbott Diabetes Care.
Protocol
The study was prospectively registered on ClinicalTrials.gov (Identifier No: ADC-SRR-IIS-18-23).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.