
Abstract
Introduction:
The growing prevalence of diabetes has increased the need for scalable technologies to improve outcomes. My Diabetes My Way (MDMW) is an electronic personal health record (ePHR) available to all people with diabetes in Scotland since 2010, associated with improved clinical outcomes among users. MDMW pulls data from a national clinician-facing informatics platform and provides self-management and educational information. This study aims to describe MDMW user demographics through time with respect to the national diabetes population, with a view to addressing potential health inequalities.
Methods:
Aggregate data were obtained retrospectively from the MDMW database and annual Scottish Diabetes Survey (SDS) from 2010 to 2020. Variables included diabetes type, sex, age, socioeconomic status, ethnicity, and glycemic control. Prevalence of MDMW uptake was calculated using corresponding SDS data as denominators. Comparisons between years and demographic sub-groups were made using Chi- Squared tests.
Results:
Overall uptake of MDMW has steadily increased since implementation. By 2020, of all people with T1D or T2D in Scotland, 13% were fully enrolled to MDMW (39,881/312,326). There was proportionately greater numbers of users in younger, more affluent demographic groups (with a clear social gradient) with better glycemic control. As uptake has increased through time, so too has the observed gaps between different demographic sub-groups.
Conclusions:
The large number of MDMW users is encouraging, but remains a minority of people with diabetes in Scotland. There is a risk that innovations like MDMW can widen health inequalities and it is incumbent upon healthcare providers to identify strategies to prevent this.
Keywords
Introduction
Approximately 10% of the world’s population has diabetes, accounting for 10% of global health spending. 1 Eighty percent of costs are due to complications, the majority of which are preventable through better clinical management and patient self-management. 2 Despite clear evidence for pre-emptive approaches through complications screening, risk factor reduction and appropriate self-management, care remains suboptimal, and outcomes poor. 3
Diabetes care in Scotland relies on a series of managed clinical networks supported by a national informatics platform, SCI-Diabetes. 4 SCI-Diabetes serves as an electronic health record containing data extracted from primary care, laboratory systems, and other services (eg, retinal screening) and is accessed by all healthcare professionals involved in the care of people with diabetes. All people with diabetes in Scotland (n ~300,000) are registered within SCI-Diabetes, which was implemented nationally in 2006. The Scottish Diabetes Survey (SDS) provides an annual overview of key performance indicators. 5 SCI-Diabetes is associated with significant improvements in care quality and outcomes;6,7 however socioeconomic status is a consistent predictor of glycemic control. 8
Diabetes data-driven Information Technology Systems have been associated with improvement in diabetes care. Technologies that incorporate tailored support and education for people with diabetes are associated with improved self-management and clinical outcomes. 9 The My Diabetes My Way (MDMW) electronic Personal Health Record (ePHR) links with SCI-Diabetes to provide users with personal health data and provides tailored education through multimedia online resources and courses that are accessed via an interactive website or app. 10
MDMW takes a subset of data from primary and secondary care, including key diabetes indicators (HbA1c, blood pressure (BP), body mass index (BMI)), as well as eye and foot screening results, medication and clinical correspondence. The platform provides users access to these records, as well as advice and resources (information, structured education, and videos) tailored to each user through data characteristics and the implementation of rules and algorithms. 11 Additionally, users can manually enter home-recorded data (eg, weight, blood pressure, blood glucose), and set their own health and lifestyle goals. Data and resources are presented via a series of user-friendly menus, data visualizations and explanations. History graphs allow users to interrogate their data over time, and “target charts” display key diabetes indicators to encourage users to reach a target (green) region (Figure 1). A checklist of care measures on MDMW (based on the Diabetes UK “15 Healthcare Essentials” 12 ) displays care targets achieved for each user (Figure 2), while encouraging users to follow-up overdue assessments with their healthcare team.
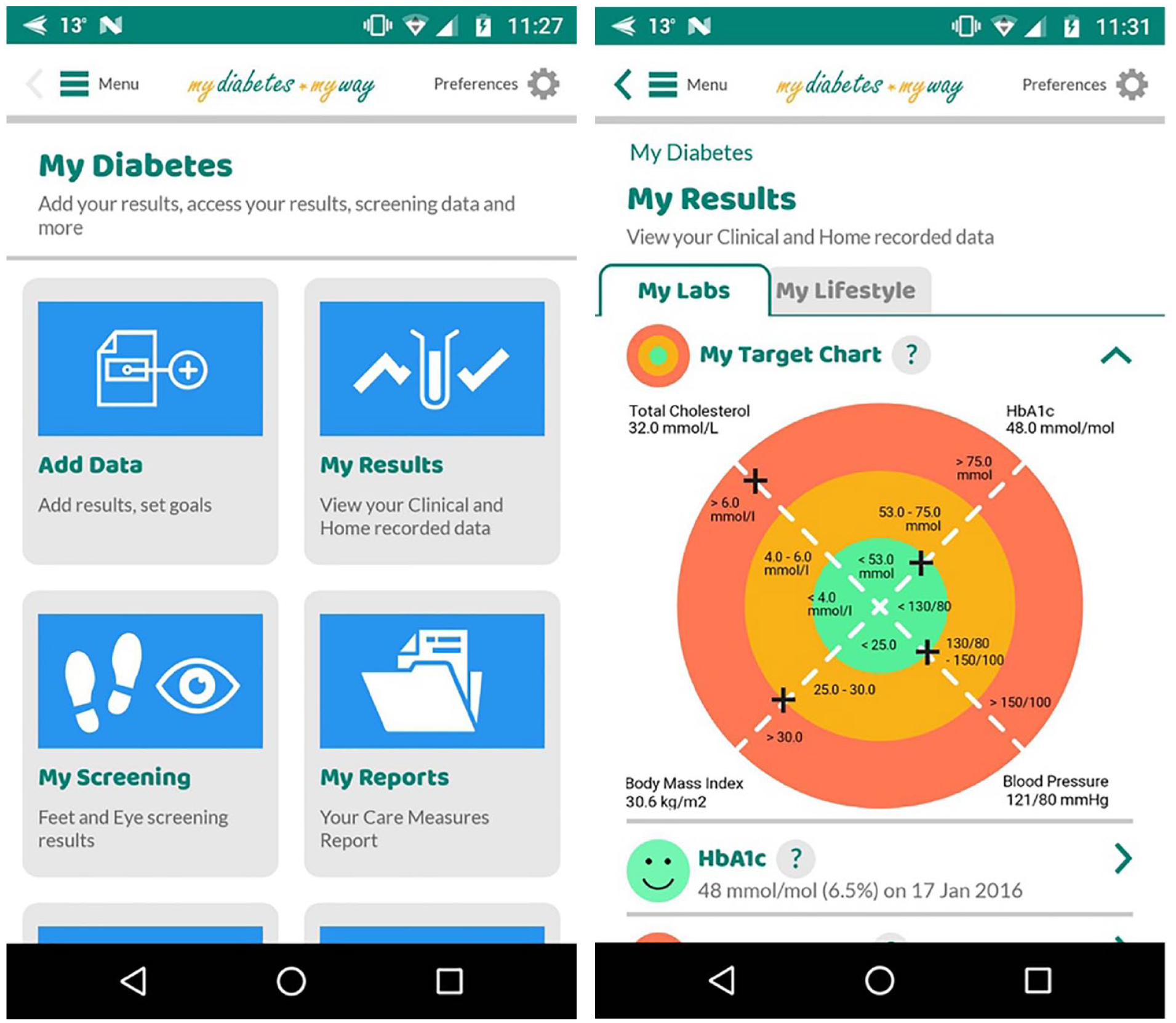
Screenshots from MDMW app showing a menu page and “target chart” mapping HbA1c, cholesterol, blood pressure, and body mass index for a hypothetical patient.
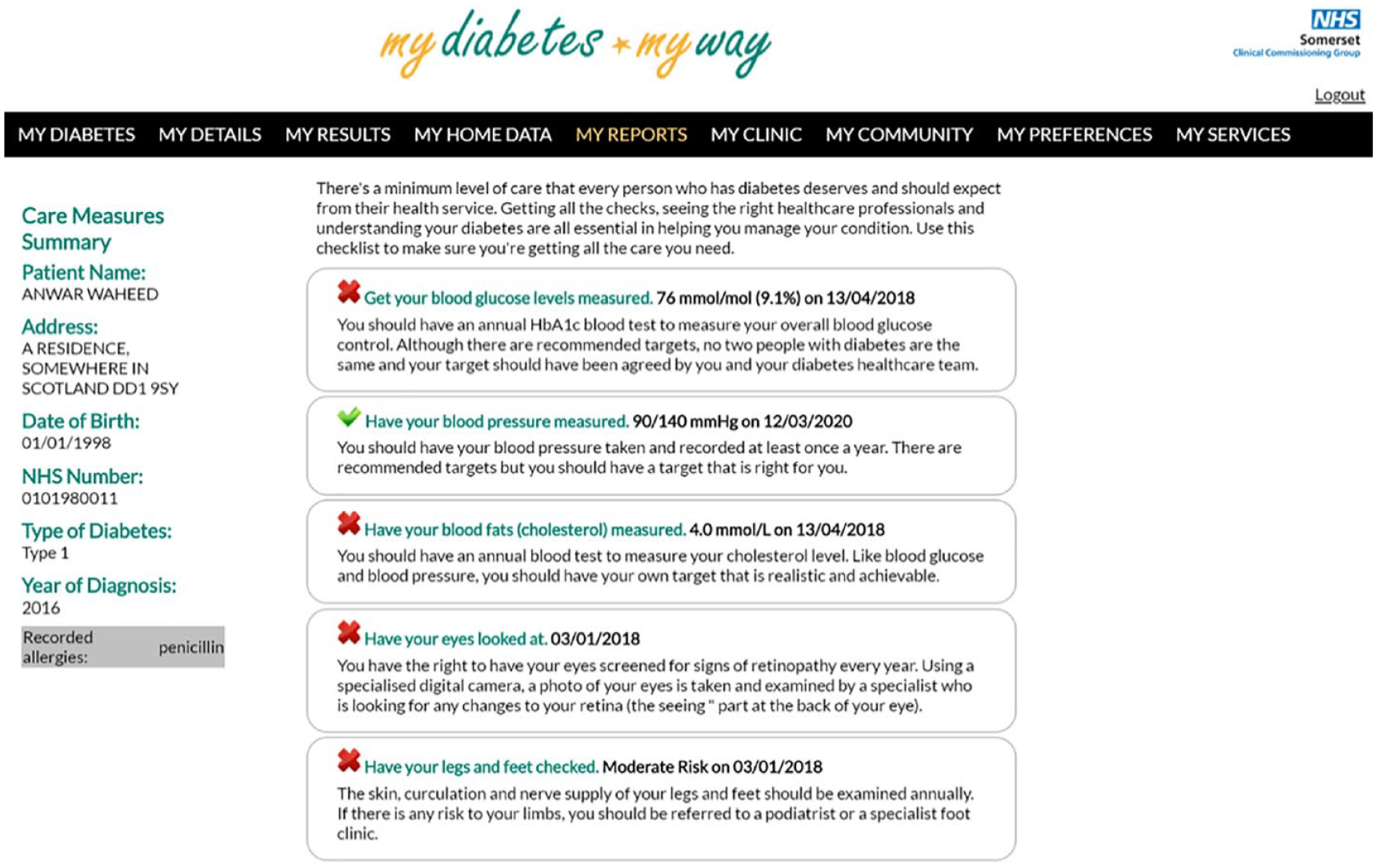
A screenshot from the MDMW web platform mapping an individual’s care parameters (hypothetical patient) to a national standard (the Diabetes UK 15 healthcare essentials).
MDMW launched in 2008, initially as an online repository for diabetes-related education. 10 Full ePHR linkage with SCI-Diabetes was established in 2010 and is freely available to all people 14 years or older within Scotland with any type of diabetes (proxy access for parents/carers of younger people with diabetes is currently under development). Patients self-register for MDMW via the online site, followed by postal identity verification and consent (this process can also be completed by their healthcare team via SCI-Diabetes). Thereafter, access to the site is via the MDMW web-based service or mobile app. It is associated with high user satisfaction 13 and improvements in key parameters such as HbA1c, resulting in an overall cost-saving (approximately 3:1-5:1 return on investment). 14
In the UK in 2020, 96% of households had access to the internet and 84% owned a smartphone. 15 Both internet access and smartphone ownership are close to 100% in younger age groups, however the prevalence of both is consistently lower in the over 65 years old age group. As internet access increases, the concept of a “digital divide” within society has evolved to include not only the sociodemographic determinants of internet access, but how this access is used, and how inequities in digital skills and digital literacy can impact on the consequences of that use. 16 Cross-sectional studies have demonstrated that those who access diabetes-related health information via ePHRs are more likely to be white and from a well-educated background. 17 Those with diabetes with lower socioeconomic status and (SES) from non-white ethnic groups have been found to be more likely to access PHRs via a mobile device rather than a desktop computer. 18
These cross-sectional studies offer a snapshot of behaviours at any given timepoint. However, a longitudinal perspective is important to understand how ePHR adoption varies through time. The diffusion effect describes the cumulative influence on an individual to adopt or reject a technology as that technology becomes more ubiquitous through time, resulting in a change to societal norms. 19 So called “early adopters” tend to be more affluent and educated than the majority who adopt the innovation at a later stage. 19 Until widespread adoption is achieved, there is a risk that eHealth innovations serve to exacerbate existing health inequalities. 20
This study aims to characterize MDMW uptake within the Scottish diabetes population over a period of 10 years, with respect to user demographics and rate of adoption. In doing so, it will seek to identify sub-groups that have yet to engage with MDMW with a view to developing strategies to encourage adoption and mitigate against health inequalities.
Methods
Aggregate data were retrieved from the MDMW database for MDMW users over a 10-year period (December 2010 to December 2020). MDMW users were defined as those that had registered to use the service and have completed the enrolment process (including identity verification). Variables of interest included type of diabetes, sex, age category (thresholds as defined by the Scottish Diabetes Survey 5 ), socioeconomic status, ethnicity, and glycemic control. All MDMW users (defined as those individuals that had registered to use the system and had completed the enrolment process) were included in the analysis.
Corresponding demographic characteristics of the Scottish diabetes population were obtained via aggregate data extracted from the Scottish Diabetes Survey 5 over the same 10-year period. Missing data items of interest were collated by an analyst within the National Health Service (NHS) Research Scotland Diabetes Network, using data archived from previous surveys and obtained via direct correspondence. Similarly, aggregate data that will contribute to the 2020 Scottish Diabetes Survey (not yet published) were obtained via direct correspondence with the SCI-Diabetes team.
The prevalence of MDMW enrolment was calculated for each calendar year of the study period by dividing the number MDMW users by the total number of people with Type 1 Diabetes (T1D) or Type 2 Diabetes (T2D) (derived from the SDS) in that year, and expressed as a percentage. The prevalence of MDMW usage within each demographic subgroup was also calculated using the corresponding SDS aggregate data as the denominator and presented graphically. Chi Square for trend was used to investigate effect of year on number of MDMW users compared with the number of non-MDMW users. Chi Square was also used to compare MDMW users between years and strata, via a series of 2 × 2 contingency tables.
Socioeconomic status was defined by Scottish Index of Multiple Deprivation (SIMD) quintile 21 and was derived retrospectively using SIMD 2016 applied to current address. SDS SIMD status was only available from 2012 onwards. HbA1c categories (<58 mmol/mol, 58-75 mmol/mol and >75 mmol/mol) were derived from last available HbA1c from January 1 of any given year. For SDS publications, this HbA1c is only reported if it was obtained within the previous 15 months. In order to maximize data capture from MDMW users, this date threshold was removed to include glycemic data for all users, irrespective of date of last HbA1c.
Results
Overall Uptake
By the end of 2020, 55,605/312,326 (18%) people with T1D or T2D in Scotland had registered to use the MDMW system, of which 39,881 had completed the enrolment process and were considered MDMW users. The total number of MDMW users compared to people with diabetes rose significantly from 77/237,468 (0.02%) in 2010 to 39,881/312,326 (13%) in 2020 (P < .001). Proportionately more people with T1D were MDMW users compared to those with T2D, with greater engagement from the start of MDMW implementation. By 2020, the gap had widened to 10,548/34,087 (31%) T1D compared to 29,333/278,239 (11%) T2D (P < .001). – see Table 1 and Figure 3.
Overall Uptake of the MDMW System—Number of MDMW Users and Corresponding Number of People with T1D or T2D Extracted from the Scottish Diabetes Survey (SDS), by Calendar Year. Annual % MDMW Usage Calculated Using Annual SDS Data as Denominator.
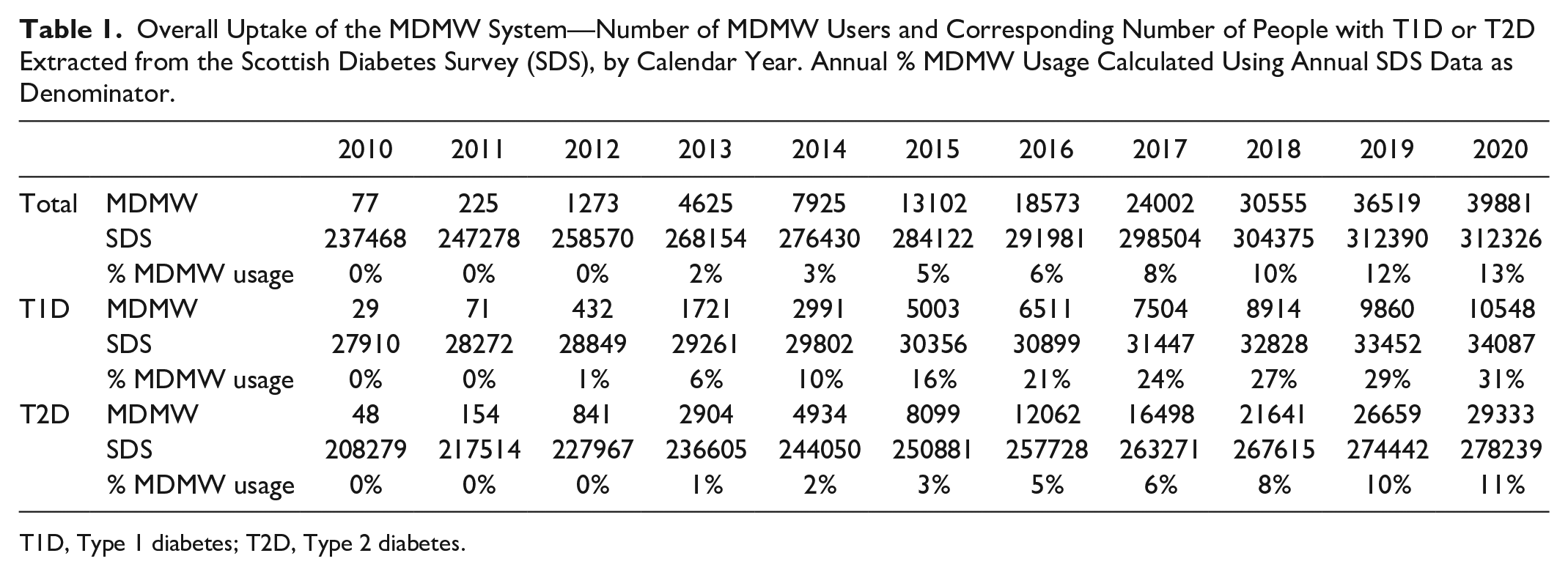
T1D, Type 1 diabetes; T2D, Type 2 diabetes.
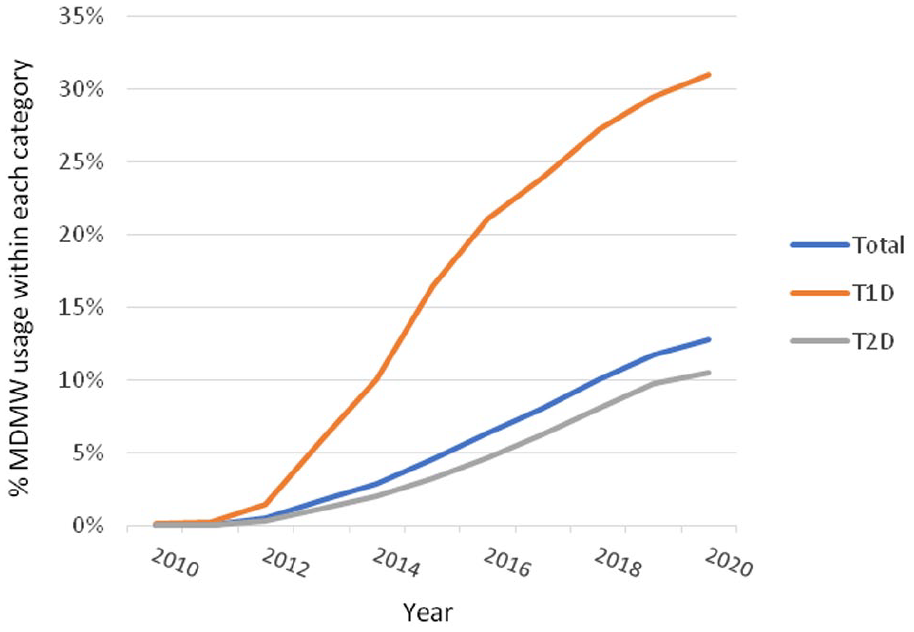
Overall uptake of the MDMW system—Annual % MDMW usage with respect to total number of people with T1D or T2D in Scotland and stratified by diabetes type.
Gender
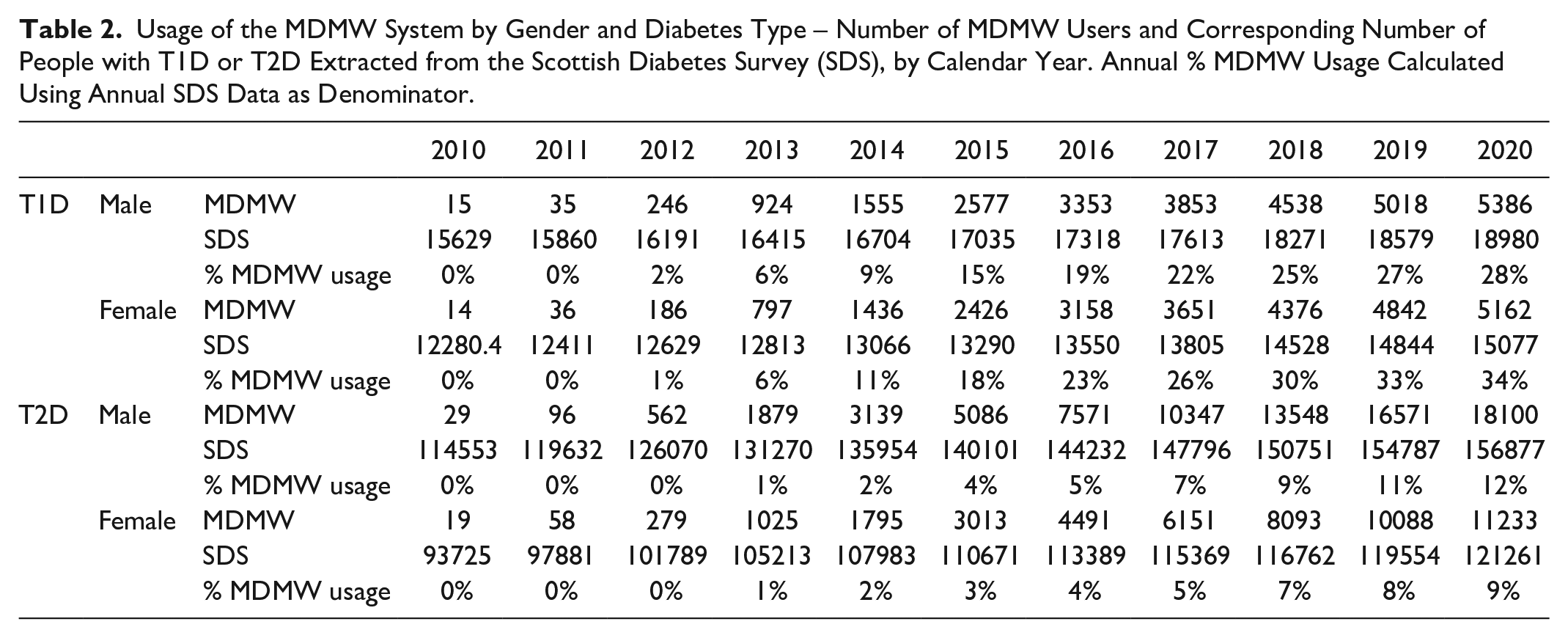
Both males and females demonstrated a significant increase in MDMW uptake throughout the period of study, regardless of diabetes type (P < .001). Proportionately more females than males with T1D were MDMW users, while this was reversed for those with T2D—see Table 2 and Figure 4. There was a widening gender gap through time for both types of diabetes, so that by 2020 significantly more females with T1D were enrolled compared with males (5,162/15,077 (34%) vs 5,386/18,980 (28%) P < .001) and significantly more males with T2D were enrolled compared with females (18,100/156,877 (12%) vs 11,233/121,261 (9%) P < .001).
Usage of the MDMW System by Gender and Diabetes Type – Number of MDMW Users and Corresponding Number of People with T1D or T2D Extracted from the Scottish Diabetes Survey (SDS), by Calendar Year. Annual % MDMW Usage Calculated Using Annual SDS Data as Denominator.
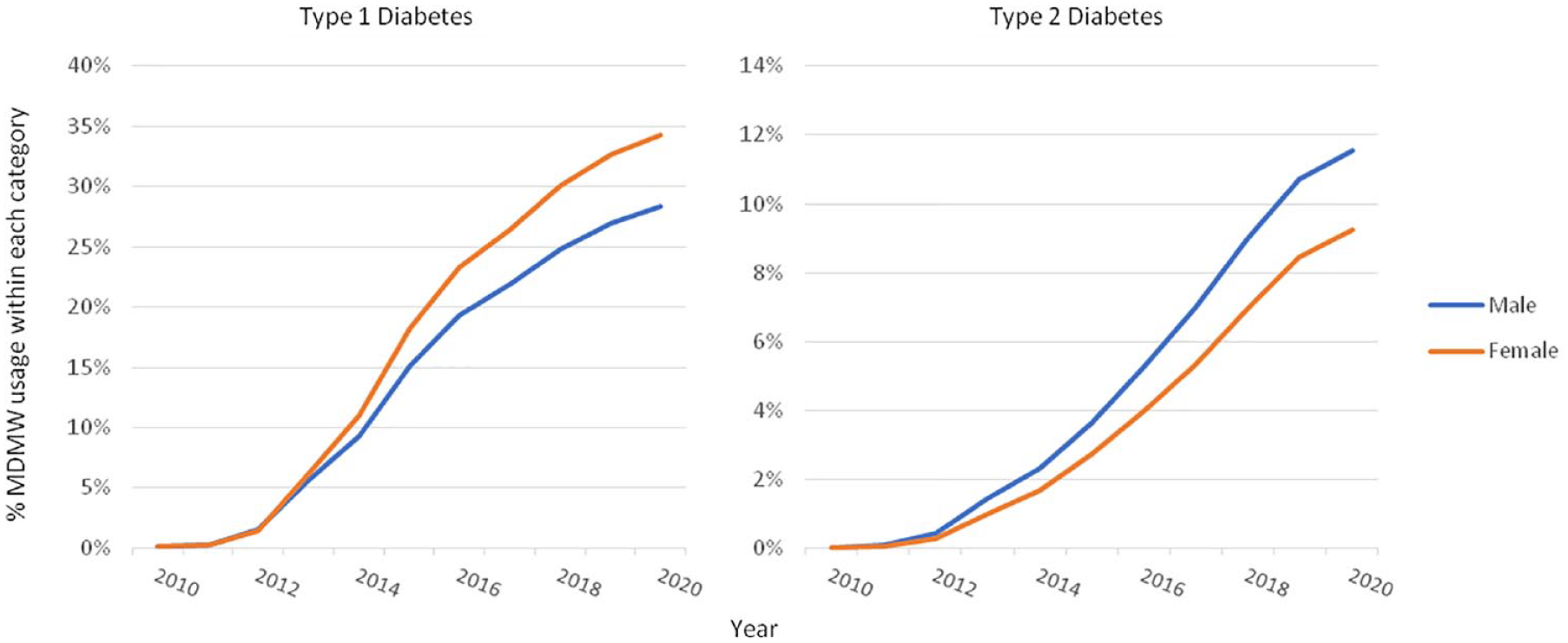
Usage of the MDMW system by gender and type of diabetes—Annual % MDMW usage calculated using number of MDMW users divided by corresponding population level data obtained from the Scottish Diabetes Survey.
Age
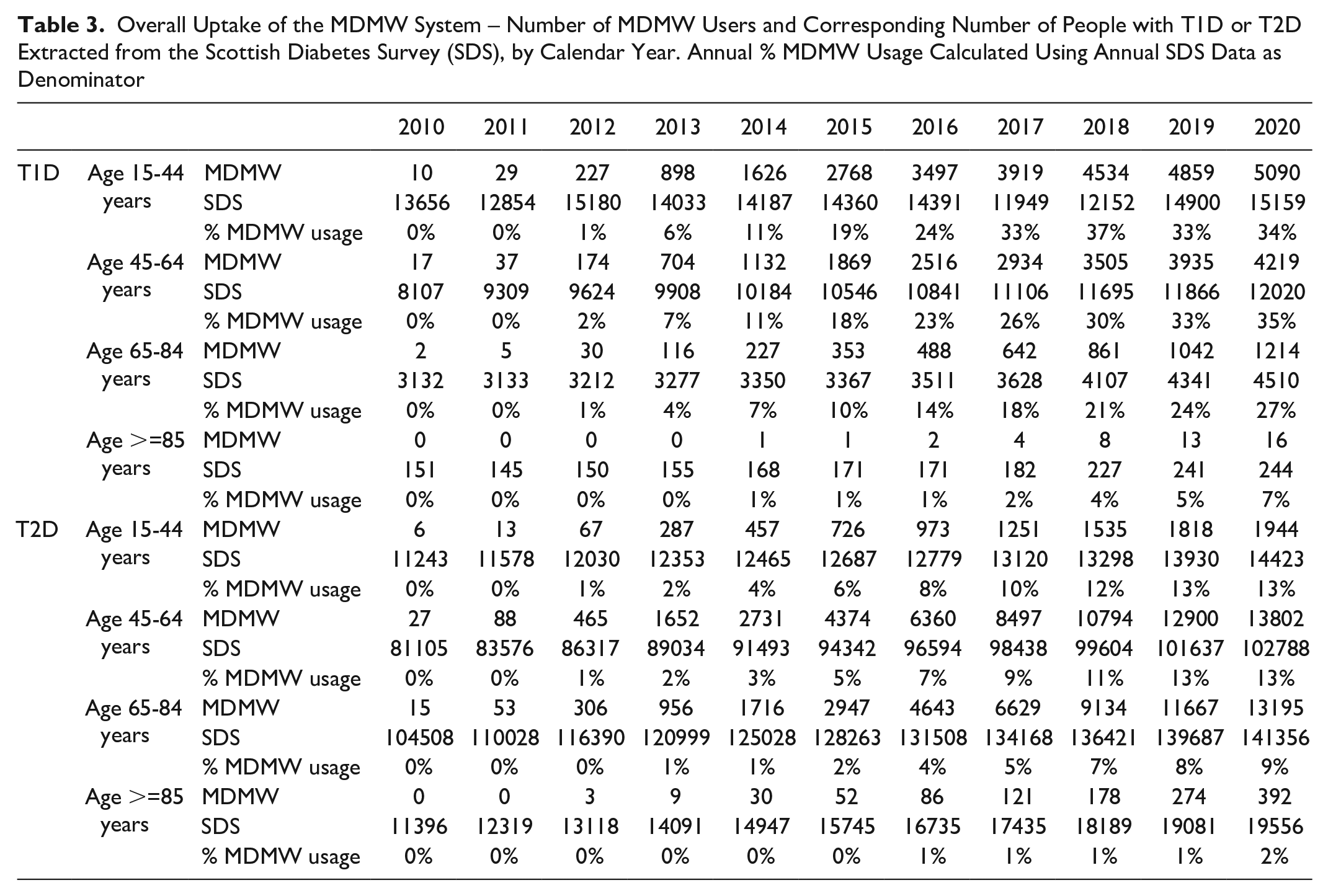
All age groups demonstrated a significant increase in MDMW uptake throughout the period of study, regardless of diabetes type (P < .001). Those within the younger age categories (15-44 years old and 45-64 years old) consistently demonstrated the greatest uptake of MDMW in both T1D and T2D – see Table 3 and Figure 5. The proportion of MDMW users rose in all age categories through time, with evidence of increased users among older age groups in recent years. A large increase in the background T1D population in 2019 resulted in a relative decrease in MDMW users in this age category.
Overall Uptake of the MDMW System – Number of MDMW Users and Corresponding Number of People with T1D or T2D Extracted from the Scottish Diabetes Survey (SDS), by Calendar Year. Annual % MDMW Usage Calculated Using Annual SDS Data as Denominator
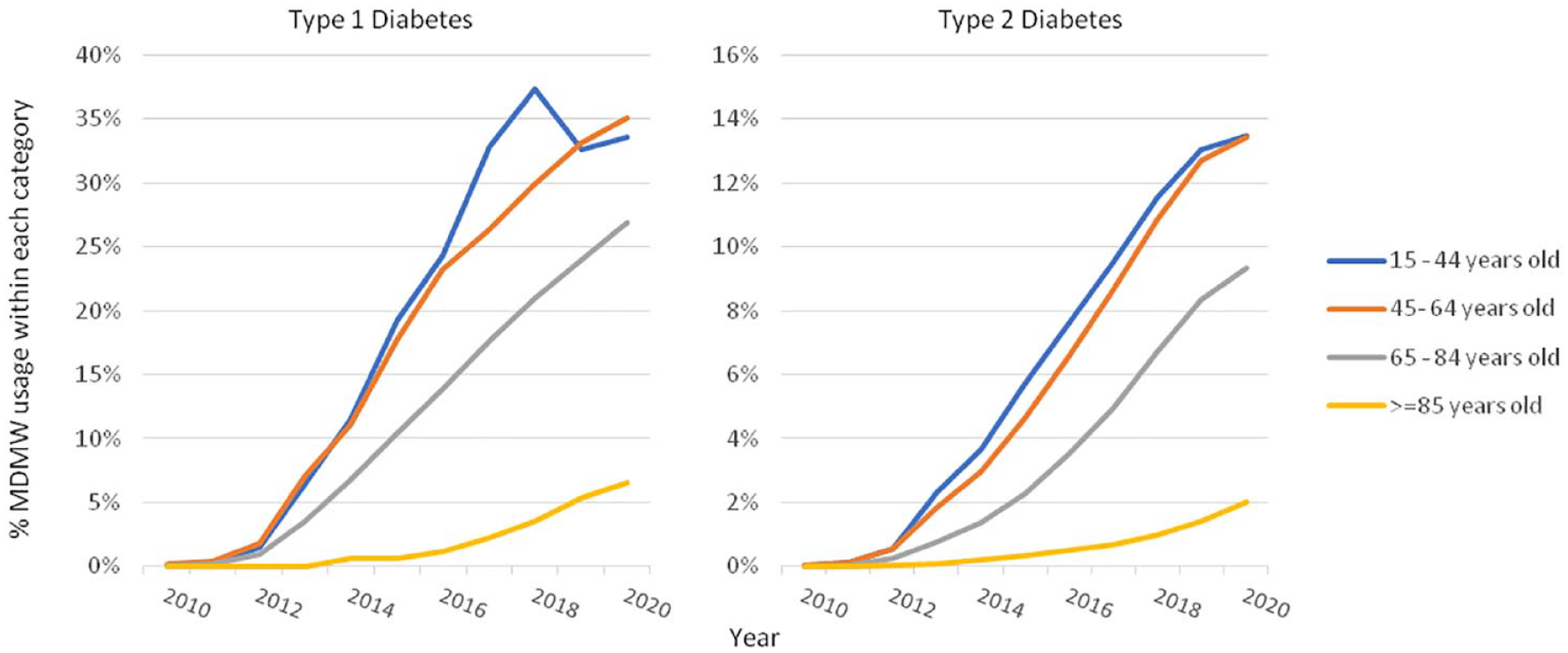
Usage of the MDMW system by age category and type of diabetes - Annual % MDMW usage calculated using number of MDMW users in each category divided by corresponding population level data obtained from the Scottish Diabetes Survey.
Socioeconomic Status
SES data were available from 2012 onwards. Since then, all SIMD quintiles demonstrated a significant increase in MDMW uptake throughout the period of study, regardless of diabetes type (P < .001). There was a clear social gradient, whereby MDMW use was more prevalent among those less deprived. The proportion of users in all SIMD quintiles increased through time, however the gap between SIMD 1 (most deprived) and SIMD 5 (least deprived) grew as usage has become more prevalent, resulting in approximately twice as many users in the least deprived quintile—see Table 4 and Figure 6. In 2020, for those with T1D, usage in SIMD 1 was 1,497/6,753 (22%), compared to 2,557/6,321 (40%) in SIMD 5 (P < .001). Similarly, for those with T2D in SIMD 1, 4,832/65,952 (7%) were users of the system, compared with 6,625/40,703 (16%) in SIMD 5 (P < .001).
Usage of the MDMW System by Socioeconomic Status and Type of Diabetes. Number of MDMW Users and Corresponding Number of People with T1D or T2D Extracted from the Scottish Diabetes Survey (SDS), by Calendar Year. Annual % MDMW Usage Calculated Using Annual SDS Data as Denominator.
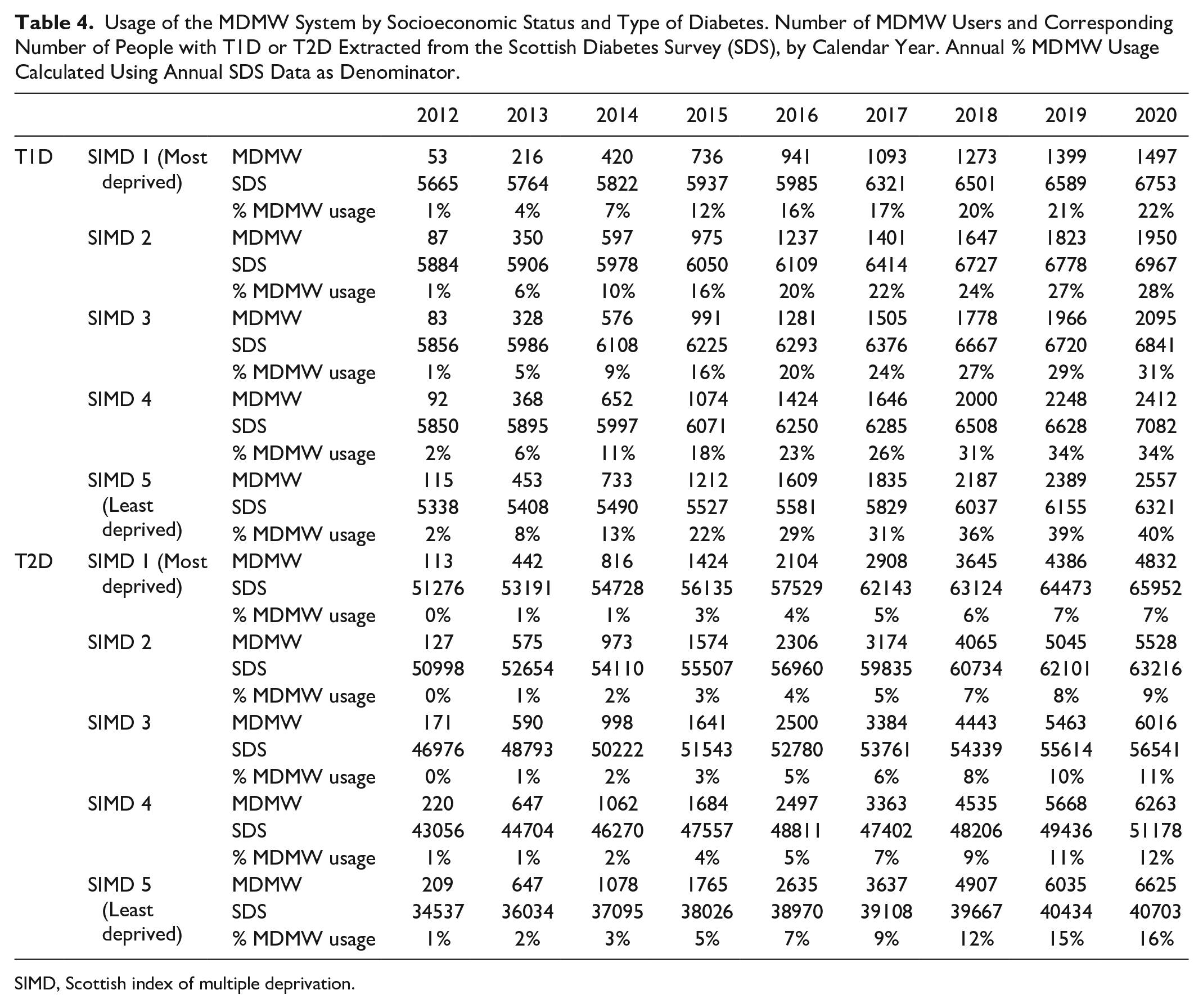
SIMD, Scottish index of multiple deprivation.
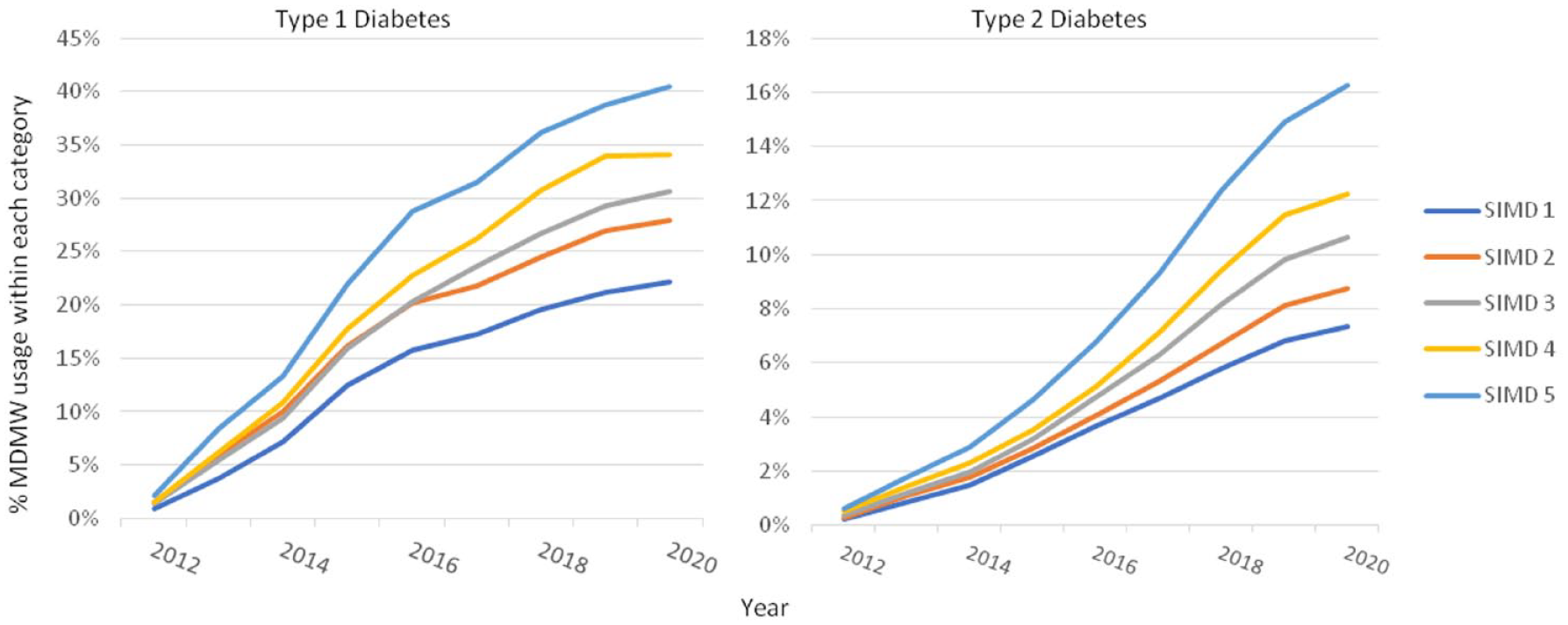
Uptake of the MDMW system by socioeconomic status (SIMD quintile) and type of diabetes. SIMD 1 is most deprived; SIMD 5 is least deprived. Annual % MDMW usage calculated using number of MDMW users in each category divided by corresponding population level data obtained from the Scottish Diabetes Survey.
Glycemic Control
Of the MDMW users, a minority had no recorded HbA1c in the 15 months prior to each calendar year, in which case the last available HbA1c (ie, HbA1c obtained >15 months previously) was used as a proxy for current glycemic control. In 2019, this accounted for 1,890/19,720 (9.5%) MDMW users. In 2020, this grew to 5,720/21,096 (27%) MDMW users, presumably as a result of COVID-19 emergency measures negatively impacting upon routine clinical activity.
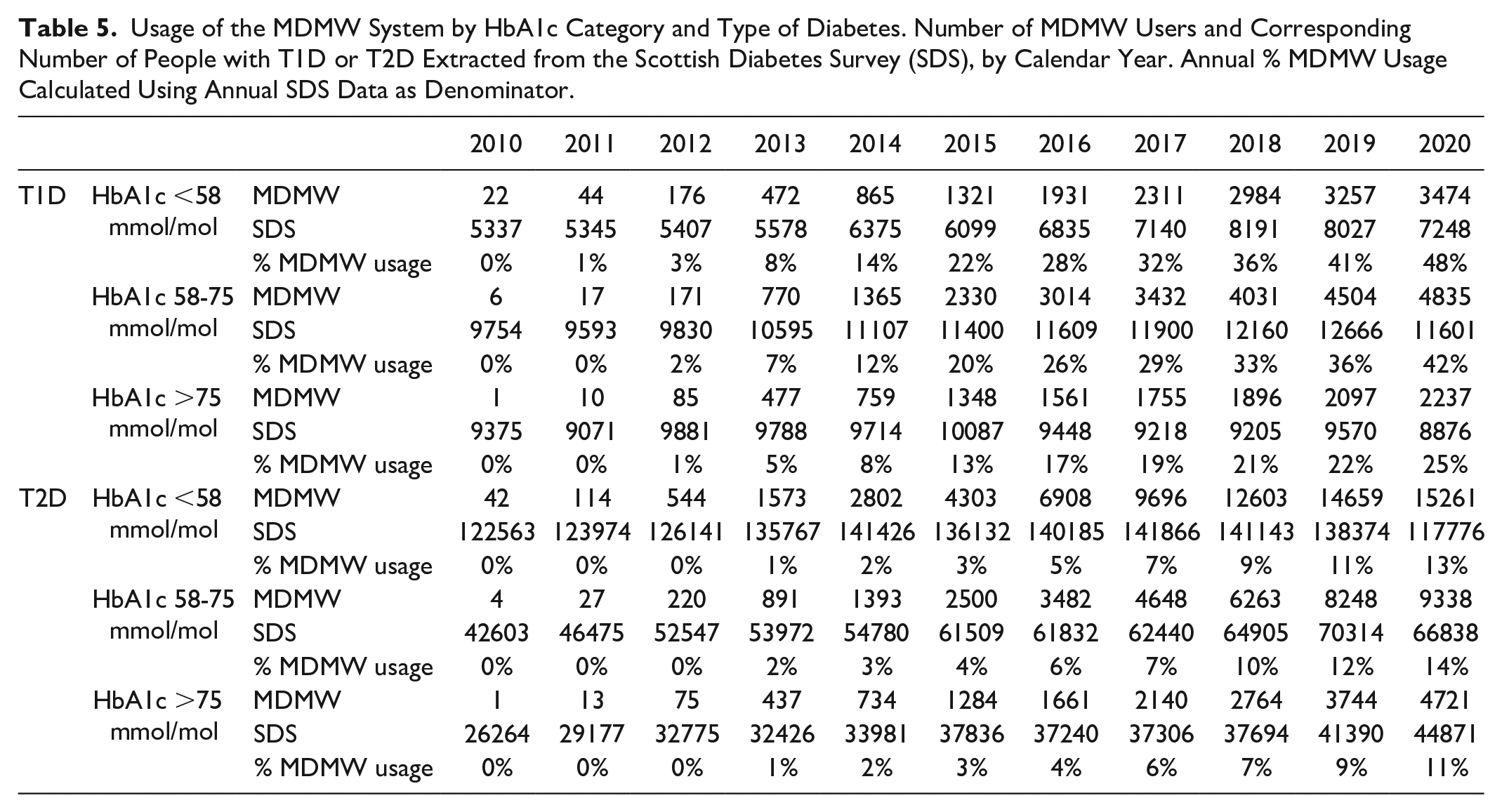
Across all categories of glycemic control, the numbers of people using MDMW significantly increased throughout the period of study, regardless of diabetes type (P < .001). The proportion of T1D users with glycemic control within target (HbA1c <58 mmol/mol) was consistently higher than those with poorer control (HbA1c >75 mmol/mol), with usage among the former approximately twice as prevalent by 2020 (3,474/7248 (48%) vs 2,237/8,876 (25%) P < .001)—see Table 5 and Figure 7. For those with T2D, the gradient in usage across HbA1c categories was less marked, however by 2020 there were proportionately fewer users with poorer glycemic control (15,261/117,776 (13%) HbA1c <58 mmol/mol vs 4,721/44,871 (11%) HbA1c >75 mmol/mol, P < .001).
Usage of the MDMW System by HbA1c Category and Type of Diabetes. Number of MDMW Users and Corresponding Number of People with T1D or T2D Extracted from the Scottish Diabetes Survey (SDS), by Calendar Year. Annual % MDMW Usage Calculated Using Annual SDS Data as Denominator.
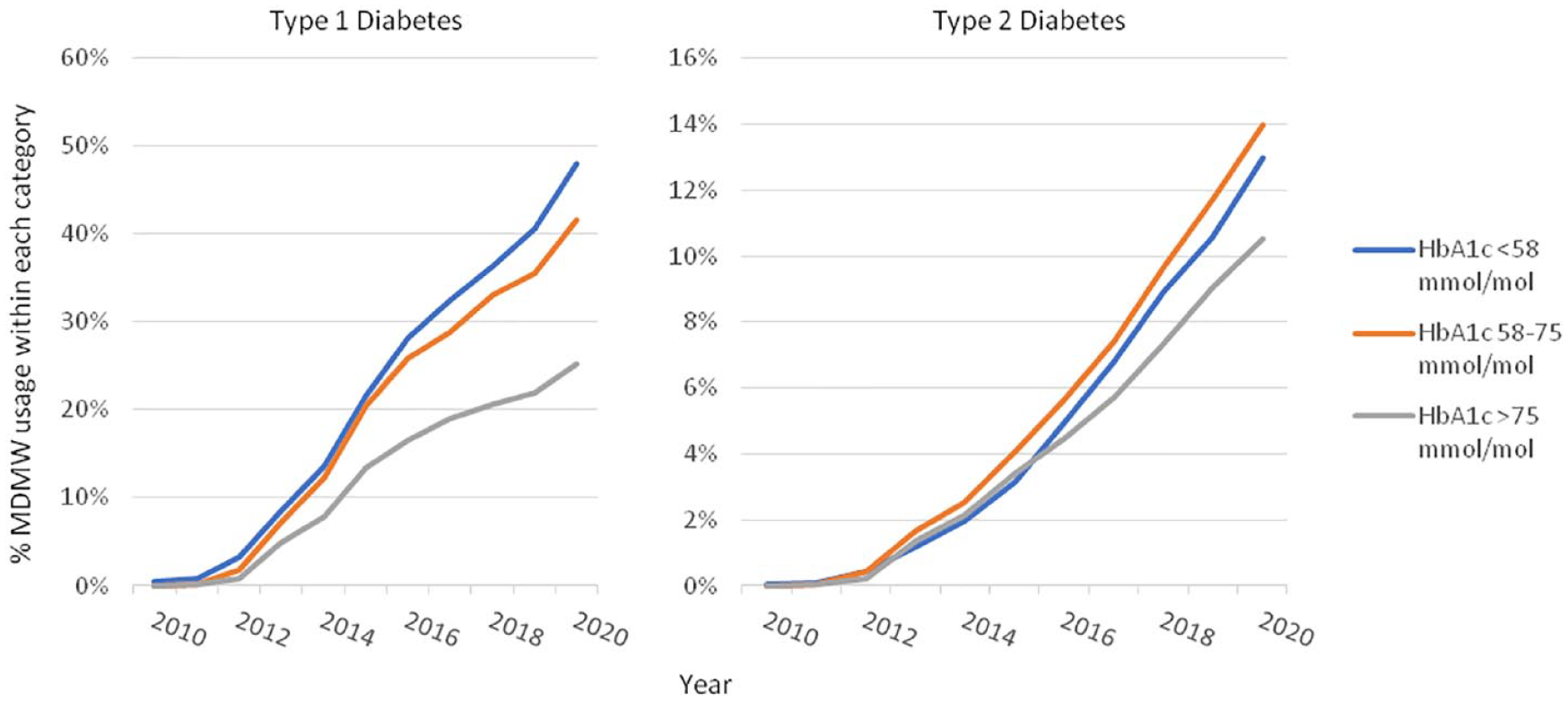
Uptake of the MDMW system by HbA1c category and type of diabetes. Annual % MDMW usage calculated using number of MDMW users in each category divided by corresponding population level data obtained from the Scottish Diabetes Survey.
Ethnicity
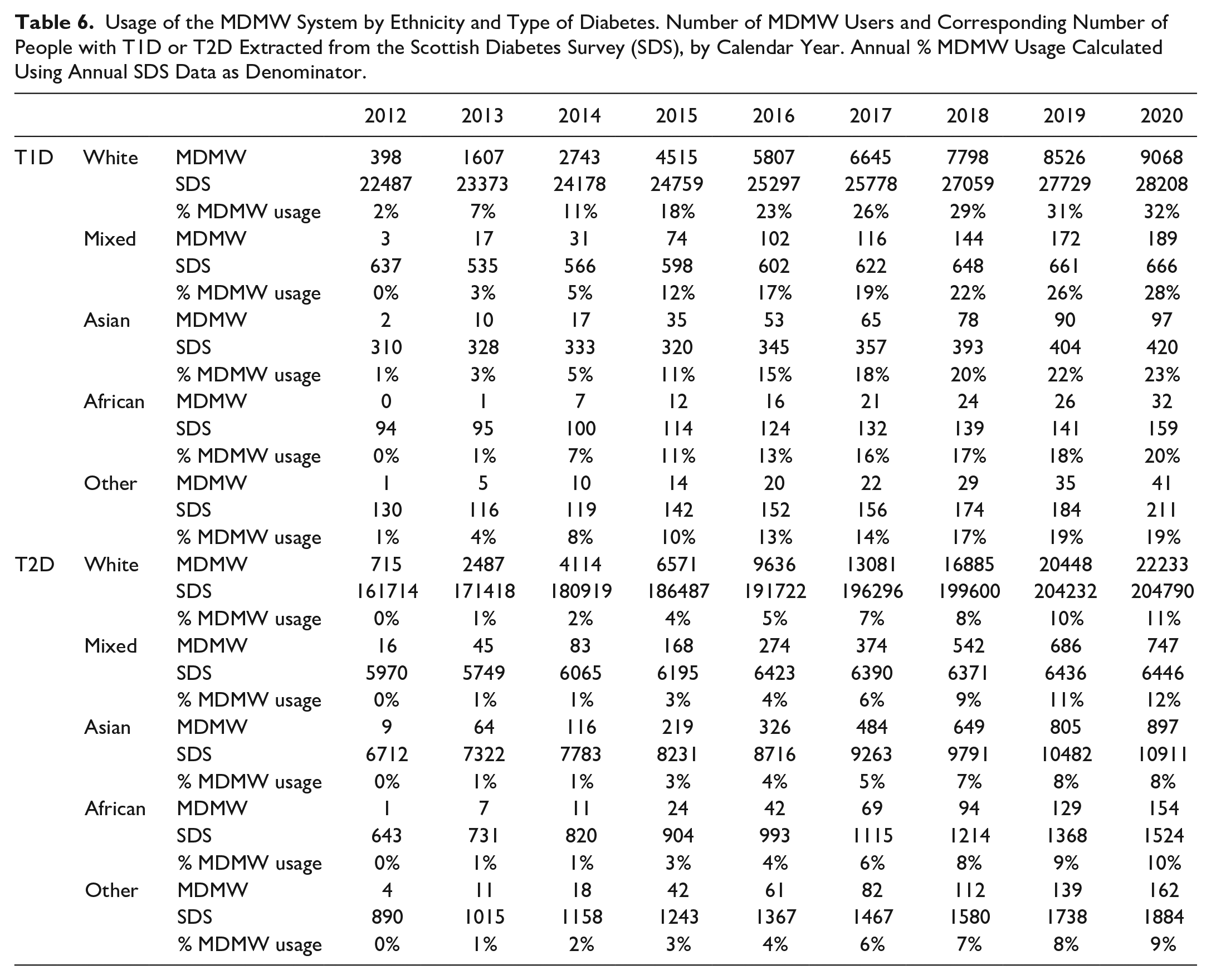
Ethnicity data was published within the SDS from 2012 onwards. Since then, all ethnic groups demonstrated a significant increase in MDMW uptake throughout the period of study relative to diabetes population of the same ethnicity, regardless of diabetes type (P < .001). The majority of MDMW users were within the White ethnic group (2020: 232,998/312,326 (75%) were White)—see Table 6 and Figure 8. It is notable that the proportion of people using MDMW with T2D from Asian ethnic groups was significantly smaller compared to White, African and Mixed groups (897/10,911 (8%) vs 23,134/212,760 (11%), P < .001).
Usage of the MDMW System by Ethnicity and Type of Diabetes. Number of MDMW Users and Corresponding Number of People with T1D or T2D Extracted from the Scottish Diabetes Survey (SDS), by Calendar Year. Annual % MDMW Usage Calculated Using Annual SDS Data as Denominator.
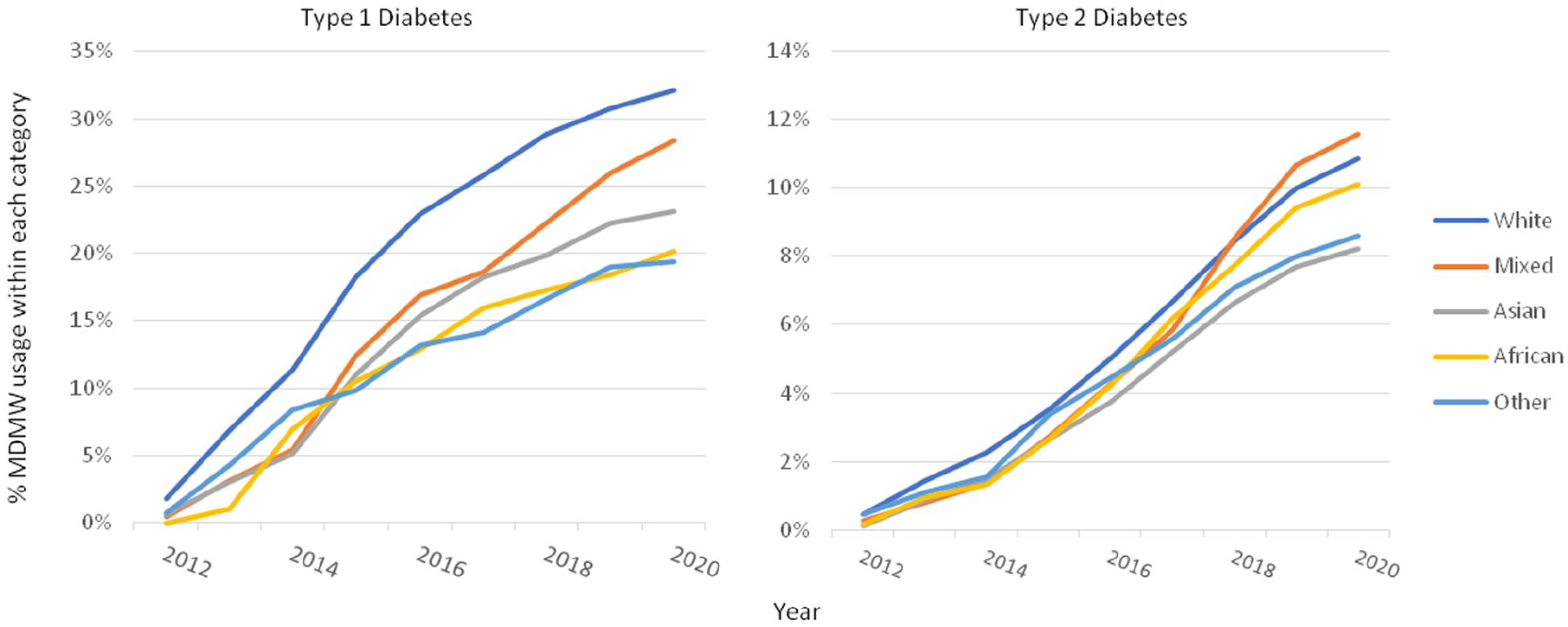
Uptake of the MDMW system by ethnicity and type of diabetes. Annual % MDMW usage calculated using number of MDMW users in each category divided by corresponding population level data obtained from the Scottish Diabetes Survey.
Discussion
This study has demonstrated the incremental uptake of a national diabetes electronic PHR over an 10-year period. By the end of 2020, 13% of people with diabetes in Scotland had enrolled to MDMW and were able to access their diabetes ePHR.
While the number of people accessing the MDMW electronic PHR for people with diabetes has steadily increased since implementation, proportionately more people with T1D use the system compared to T2D. In addition, MDMW users tend to be younger, more affluent, and with better glycemic control. This finding is neither surprising nor novel, given the known demographic predictors for being at either side of the digital divide. However, the longitudinal perspective obtained in this study demonstrates a widening gap through time between some demographic subgroups, with the potential to exacerbate health inequalities.
Given that overall penetration is 13%, MDMW could still be regarded as being within the initial phase of technology diffusion—users being characterized as “early adopters.” 19 It is hoped that as the affluent, educated early adopters are joined by the majority, then the observed digital divide should narrow. However, usage within those with T1D is more ubiquitous, with almost a third of people with T1D in Scotland being users of MDMW (the so called “early majority” 19 ). The reasons for greater uptake among those with T1D remain speculative, but might include: a lower average age in those with T1D; a greater focus on diabetes data and technologies for those with T1D; and/or greater awareness of MDMW within secondary care HCPs. Despite this increased prevalence of use among those with T1D, there continues to be a notable social and age gradient, as well as under-representation of ethnic minority groups.
The use of technology to provide patient-tailored support and education is associated with improved clinical outcomes, 9 as demonstrated by improvements in glycemic control within MDMW users. 14 While it is tempting to infer that the growing number of MDMW users with an HbA1c <58 mmol/mol is a result of MDMW usage, the use of aggregate data does not allow this hypothesis to be tested. Artificial intelligence-powered innovations have the potential to improve precision diagnostics, therapeutics and prognostics within diabetes care. 22 Work is currently underway to develop and implement clinical decision support within MDMW, driven by predictive analytics derived from machine learning techniques. As the scope for communication technologies to improve diabetes care increases, so too does the risk of exacerbating existing health inequalities.
This study demonstrates the need to proactively engage with under-represented sections of the community, to ensure that all can benefit from such advances. Previous efforts have been made to understand facilitators and barriers to increasing uptake of MDMW, 13 as well as publicity campaigns aimed at improving awareness. A MDMW steering group consisting of clinical and lay representation reviews site content on a regular basis to ensure relevance for all users of the system. In addition, users of the system are encouraged to provide feedback on their experiences with the site. 13 More recently, co-design principles have been used to improve usability of the site (unpublished). MDMW has contained multi-language content since implementation, albeit in a limited amount in comparison with the resources available in the English language. In 2018, a large amount of additional content in 5 key non-English languages was added to the site. MDMW are working toward complete site translation for priority languages, however the pace of work is limited by funding and resources. MDMW has engaged with both the NHS Lothian Minority Health Inclusion Service, and with individual specialist practitioners (eg, diabetes dieticians and educators (including bilingual speakers and individual with roles supporting ethnic minority populations) to support resource development. MDMW has also worked closely with the creators of the Carbs and Cals world food book, 23 and includes images and resources supporting African, Arabic, Caribbean and South Asian diets.
In addition to ensuring that content is relevant and accessible to all sections of society, clinical endorsement is a key facilitator of user engagement with eHealth interventions. 24 Since inception, MDMW has worked closely with healthcare professionals involved within diabetes care in Scotland, to ensure validity of content and promote awareness. MDMW is endorsed by the Scottish Diabetes Group (SDG), which works at a national level in collaboration with clinicians, experts and government to promote good diabetes care. 25 The SDG also publishes the annual Scottish Diabetes Survey, which includes MDMW uptake as a quality performance indicator. 5
It is perhaps surprising that the increase in the number of users of MDMW in 2020 has not been more marked. The COVID-19 pandemic resulted in a sea-change to our use of technology, with approximately half of the UK working population now doing some work from home (the vast majority of whom are doing so due to the pandemic). 26 In the UK, internet usage has increased by a third, with evidence of a move away from traditional modes of communication (ie, landline and SMS text) to embrace newer technologies. 27 UK healthcare services in both primary and secondary care have experienced a similar shift to online connectivity,28,29 yet this is not reflected in the uptake of MDMW, which, if anything, reduced in 2020. The reason for this remains speculative, however could be due to less patient exposure to MDMW signposting (leaflets and posters are displayed in hospital outpatient clinics and primary care waiting rooms), less healthcare exposure in general (most elective work within NHS Scotland was halted during the initial COVID emergency response) and difficulties with the postal consent and identity verification process (eg, supply chains, home working).
By the end of 2020, the total number of MDMW registrants was greater than the total number of MDMW users, resulting in 5% of the total diabetes population who have registered to use the MDMW ePHR but have never used the site. Previous work has identified barriers to accessing the ePHR, which included difficulties with the postal identity verification process. 13 This process has been simplified to encourage system usage. It should be noted that registrants who do not use the ePHR system are still able to access educational content and receive regular newsletters.
Limitations
This study includes all MDMW users that have completed the enrolment process, regardless of subsequent use of the system. The frequency of usage varies among those who have enrolled, and ranges from individuals that are highly engaged to those who do not subsequently use the system (approx. ¼ of the enrolled individuals—data not shown). This study aims to describe user uptake of the system and not subsequent usage. MDMW usage patterns were described recently, 30 with a plan to investigate further as new content is developed.
The SES of MDMW users (as defined by SIMD quintile) was derived retrospectively, using current address and SIMD 2016. 21 SIMD is recalculated every 3-4 years; therefore, SES as defined by SIMD in 2016 may not be reflective of SES in the previous or subsequent years. The majority of SIMD rankings are relatively constant are across each iteration, and so the use of contemporaneous SIMD rankings is unlikely to change the observed social gradient in MDMW users.
Glycemic control (as defined by HbA1c status) was defined as the last available result prior to any given calendar year. For SDS, this was limited to within the previous 15 months, whereas this limit was not applied to MDMW data. More than 90% of people with diabetes in Scotland had HbA1c recorded within the previous 15 months. 5 The decision to include more historical data for MDMW glycemic control was made to maximize completeness of glycemic categories (especially in view of the COVID-19 effects on routine clinical care in 2020).
The majority of the Scottish population is within the white ethnic group (96% in the 2011 census 31 ). The number of people with diabetes in Scotland from ethnic minority groups is proportionately higher than the background population, however numbers are still relatively low, making it difficult to generalize these findings to settings with greater ethnic diversity.
Conclusion
Since its inception in 2010, MDMW PHR usage within Scotland has steadily grown to include a substantial minority of people with diabetes in Scotland. As uptake has increased, so too has the gap in uptake between different demographic groups, with regards to age, socioeconomic status, ethnicity, and glycemic control. As the innovation diffuses throughout the majority of the diabetes population, it is hoped that these gaps will narrow through time. The COVID-19 pandemic (and the associated poor outcomes in people with diabetes) has brought into focus the need for effective digital solutions to augment clinical care. 32 We must act to ensure that such innovations are accessible and relevant to all, to mitigate against widening health inequalities.
Footnotes
Abbreviations
ePHR, electronic personal health record; HbA1c, Haemoglobin A1c; MDMW, My Diabetes My Way; NHS, National Health Service; SCI, Scottish Care Information; SDG, Scottish Diabetes Group; SDS, Scottish Diabetes Survey; SES, Socioeconomic status; SIMD, Scottish Index of Multiple Deprivation; T1D, Type 1 Diabetes; T2D, Type 2 Diabetes; UK, United Kingdom.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DW and SC are co-founders and shareholders of MyWay Digital Health ltd, who deploy commercial IT platforms solutions (including a My Diabetes My Way equivalent outside Scotland). MDMW in Scotland is run by the University of Dundee and funded by the Scottish Government.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Scottish Diabetes Survey and My Diabetes My Way are funded by the Scottish Government