
Abstract
Background:
The implementation of electronic health records (EHRs) may support evaluations of health care delivery, such as the prescription of newly approved medications, to adults with diabetes. We aimed to evaluate prescribing patterns of thiazolidinediones and novel glucose-lowering drug classes using electronic prescribing data contained in an outpatient EHR from 2002–2010.
Methods:
We identified adults with type 2 diabetes seen from 2002–2010 who were newly prescribed rosiglitazone (ROSI), pioglitazone (PIO), or a novel glucose-lowering drug class (other). The annual number of new prescriptions and their relative percentages (per 1000 patients) were calculated.
Results:
From 2002–2010, 6209 patients with type 2 diabetes were newly prescribed 8858 eligible medications. In 2006, ROSI and PIO accounted for 44% and 37% of new prescriptions, respectively. After 2007, the relative percentage of new ROSI prescriptions declined more rapidly than PIO prescriptions, falling to 7% and 47% of peak levels, respectively, by 2010. By 2010, the relative percentages of new ROSI, PIO, and other prescriptions were 2%, 18%, and 80%, respectively.
Conclusions:
Evaluations of EHR data represent a cost-effective method for evaluating diabetes medications with new Food and Drug Administration warnings or indications. Validation of demographic and clinical data will expand the scope of EHR-based evaluations of health care delivery and outcomes for adults with diabetes.
Keywords
Introduction
The epidemic of type 2 diabetes has fostered a rapid expansion of glucose-lowering medications, including a fourfold increase in Food and Drug Administration (FDA)-approved, new diabetes drug classes since the late 1990s.1,2 The promise of this new armamentarium has been tempered by concerns regarding the safety of established medications, including the 2007 FDA warning for restricted use of rosiglitazone (ROSI)3,4 and unknown long-term cardiovascular risks or benefits with newest agents at the time of approval. There is an interest in cost-effective methods for evaluating prescribing patterns of new and established diabetes medications.5–7 The proliferation of electronic health records (EHRs), and electronic prescribing in particular, offers a means to capture and describe changing prescribing patterns from the provider perspective. 8 The evaluation of provider-level EHR data and patient-level claims data could improve our assessment of the quality of health care delivery for adults with diabetes. We aimed to demonstrate the ability to utilize EHR-based electronic prescribing data to describe provider trends regarding the prescription of thiazolidinediones (TZDs) and new diabetes drug classes in adults with type 2 diabetes from 2002 to 2010.
Methods
The Joslin Diabetes Center is an academic outpatient specialty center in Boston, MA, that cares for approximately 12,000 adults with diabetes annually. The Joslin EHR (NextGen 5.6, Horsham, PA) was internally customized for outpatient diabetes care and fully implemented with integrated electronic prescribing in 2002. The EHR interfaces with the practice management and central laboratory systems and serves as a central repository for all patient records.
We identified adult patients with type 2 diabetes seen between 2002 and 2010 using ICD-9 codes and a field specifying diabetes type; a validation procedure demonstrated >90% concordance between these fields. We then identified those patients who were newly prescribed ROSI, pioglitazone (PIO), or any of the new glucose-lowering drug classes (other) introduced during this period; “other” included an amylin analog (FDA approved in 2005), glucagon-like peptide-1 agonists (FDA approved first in class in 2005), dipeptidyl peptidase-4 inhibitors (FDA approved first in class in 2006), and a bile acid sequestrant, which received a new diabetes indication in 2008; all dopamine agonist prescriptions were for non-diabetes indications and were excluded. New prescriptions for insulin and other diabetes medications introduced before 2002, besides TZDs, were excluded.
For patients continued on an eligible medication at their initial clinic visit, that first visit date was used as the start date. Only the first start date was used for eligible medications that were subsequently discontinued and later restarted. Patients could have more than one eligible prescription—one for each of the TZDs and new medications.
We determined the number of unique adult patients with type 2 diabetes seen annually between 2002 and 2010. The annual number of new ROSI, PIO, and other prescriptions, per 1000 patients, was calculated. Then the relative percentage of new ROSI, PIO, and other prescriptions over the 9-year period was calculated.
Results
From 2002 to 2010, between 7300 and 9300 adults with type 2 diabetes were seen annually. In this cohort, 54% were male and the mean age was 59 ± 14 years. Overall, 6209 patients were newly prescribed 8858 eligible medications; 22% (n = 1918) were for ROSI, 34% (n = 2981) were for PIO, and 45% (n = 3959) were for other diabetes medications introduced between 2002 and 2010.
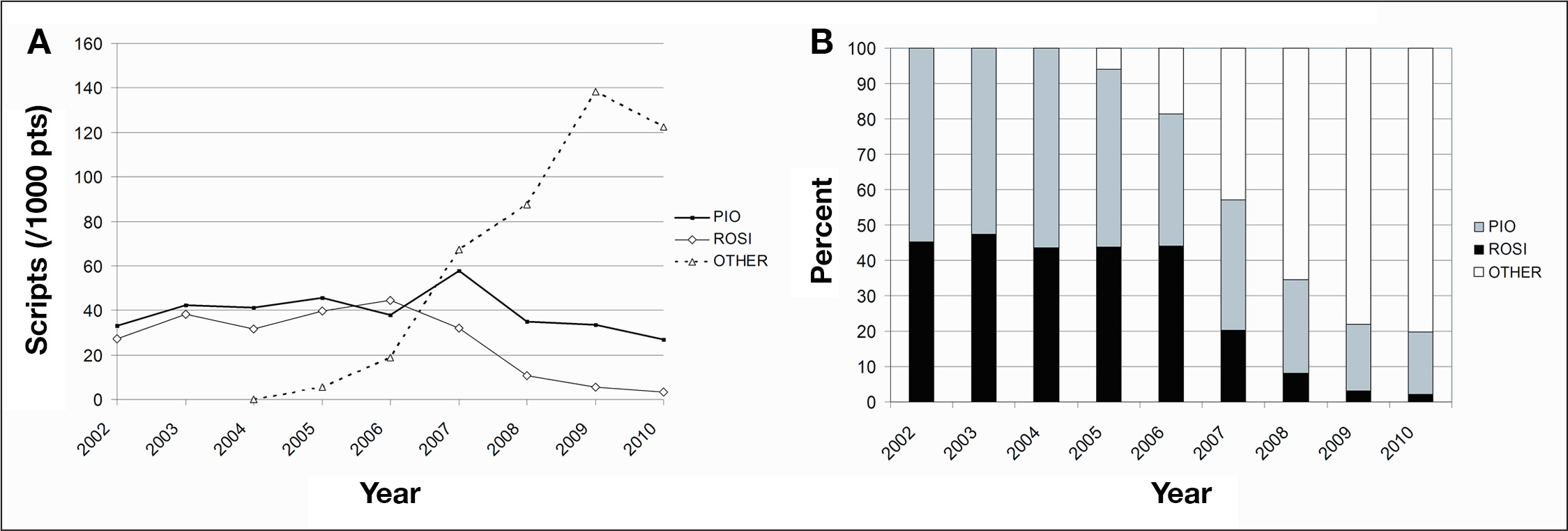
The relative percentages of new prescriptions in the three categories are presented in
Discussion
These data demonstrate the potential for an outpatient center to use EHR-based clinical information to evaluate prescribing patterns of diabetes medications. We evaluated provider prescribing patterns over a 9-year period that included a FDA safety warning and new classes of therapeutics for diabetes management. Insulin and other medications introduced before 2002 were excluded, as there were no changes in their FDA indications. This analysis of EHR-based clinical prescribing information may reflect clinician responsiveness to a widely reported FDA safety warning for ROSI as well as a possible class effect, given the decline in PIO prescriptions after 2007. The data also demonstrated a rapid adoption of novel diabetes drug classes, suggesting provider responsiveness to new FDA-approved medications or indications and possibly to continued unmet need for new hypoglycemic therapies.
The current analysis is not intended to inform the rationale behind providers' prescribing patterns or their impact on patient outcomes such as glycemic control. Retrospective analyses of clinical databases require extensive validation and are generally reserved for research-quality databases, and represent an important future goal. 9 However, we believe our approach to diagnostic coding coupled with prescription information was captured with integrity and adds confidence to our findings. Future investigations of EHR-based demographic and clinical data with confirmatory validation procedures will permit broader evaluation of all available diabetes medications and health outcomes to further our understanding of evolving patterns over time.
Pharmacy and claims databases may reliably capture patient use of diabetes medications but have modest clinical information, typically limited to ICD-9 codes, which can be difficult to validate. 10 Electronic health records are increasingly recognized as an alternative, cost-effective resource for evaluating trends in health care delivery and outcomes, and EHR data may best reflect provider behaviors, as clinical content is not limited to patient claims.8,11 Efforts to support broader EHR adoption may offer novel opportunities to evaluate the care of patients with diabetes. 12
We believe the patient volume of a large outpatient academic specialty center permitted reliable estimates of prescription changes over time. The validity of EHR data is suggested by the similarity of these findings to analyses of large, nationally representative pharmacy databases evaluating TZD use.13,14 However, validation of a broader network of EHR-based electronic prescribing data, including the use of primary care practice data, may improve generalizability of these findings for adults with type 2 diabetes. Indeed, some patients might have received outpatient diabetes care across multiple care settings, which could impact the present analysis. Finally, we did not systematically collect information related to comorbidities or other patient factors that might have influenced prescribing patterns due to absolute or relative contraindications to the medications under investigation.
Conclusions
This article demonstrates the ability to capture provider-level data around health care delivery, which can supplement patient-focused claims data when evaluating the quality of diabetes care delivered to adults with type 2 diabetes. Additionally, EHR-based evaluations may be useful in future investigations aimed at describing the impact of external influences on prescribing patterns, including scientific and lay publications.
Footnotes
Abbreviations:
Sanjeev N. Mehta received internal funding from the Herbert Graetz Award.