
Abstract

Early diagnosis of diabetes and prediabetes may help decrease the severity and prevalence of type 2 diabetes (T2D) complications.1,2 Incorporating continuous glucose monitoring (CGM) into worksite health screenings may help individuals gain insight into their glycemic patterns. 3 In this study, we conducted a worksite diabetes screening that included a 10-day blinded CGM wear and HbA1c test. The objective was to assess the feasibility and acceptability of the worksite diabetes screening augmented by blinded CGM wear, and to determine the extent of undiagnosed diabetes and prediabetes among study participants.
Participants were US residents ≥18 years old, not currently using CGM, and eligible as employees or de-pendents for an employer-sponsored health plan. The study protocol was approved by the Western Institu-tional Review Board and registered as a clinical trial (NCT04529824). All study visits were conducted at one employee health center in a suburban town in the southeastern United States. At the first visit, participants provided informed consent and were trained by study staff on how to insert and wear the CGM system (Dexcom G6, San Diego, CA). Participants returned to the health center after 10 days; the CGM was removed from participants and a point-of-care HbA1C was collected (unless a recent HbA1C result was available). Participants received a $25 gift card after completing each visit. After the second visit, participants were mailed a personalized report that included visual summaries of their CGM data and a recommendation to discuss the report with their healthcare professional. Participants were categorized into subgroups based on self-reported diabetes diagnosis and HbA1C: no diabetes, prediabetes, T2D, and type 1 diabetes (T1D). 4
Between April and August 2019, 207 people (mean ± SD age 51 ±10 years, 84% female, 16% African American, 15% Hispanic, 64% obese) enrolled in the study. HbA1c screening identified seven participants with undiagnosed T2D and 29 with previously unknown prediabetes. The final prevalence was 91 (44%) no diabetes, 42 (20%) prediabetes, 69 (33%) T2D, and five (2%) T1D. Satisfaction with the screening was high, and all participants reported they would recommend the screening to family and coworkers. Most participants (94%) reported that the study provided personalized information about their health that was helpful and that receiving CGM data in real-time (unblinded) would be “extremely” or “very” useful.
A total of 176 (85%) participants provided sufficient CGM data (ie, 60% of possible values) for analysis. The mean, standard deviation, and coefficient of variation of CGM-measured glucose showed increasing linear trends across subgroups (P < .001); while HbA1C and percent time in range (70-130 mg/dL and 70-180 mg/dL) had decreasing linear trends across subgroups (P < .001) (Table 1).
Mean and Standard Deviation of CGM-Measured Glucose Metrics Over Wear Period by Diabetes Subgroups (N = 176). 1
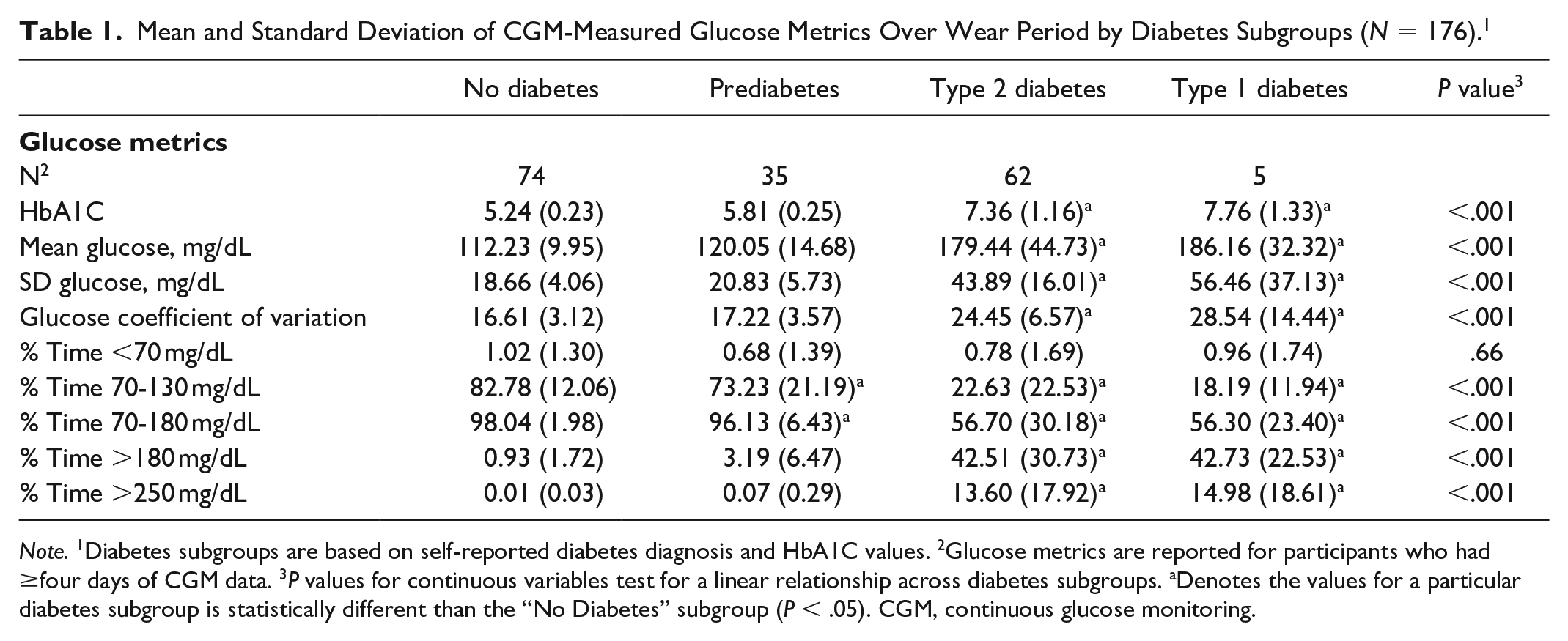
Note. 1Diabetes subgroups are based on self-reported diabetes diagnosis and HbA1C values. 2Glucose metrics are reported for participants who had ≥four days of CGM data. 3P values for continuous variables test for a linear relationship across diabetes subgroups. aDenotes the values for a particular diabetes subgroup is statistically different than the “No Diabetes” subgroup (P < .05). CGM, continuous glucose monitoring.
Incorporating blinded CGM into a worksite diabetes screening was feasible and acceptable to participants. Including CGM in diabetes screenings could be used to triage participants into more personalized behavior change and diabetes management programs.3,5 While these findings may not be generalizable to all health care centers, this study indicates that participants valued the personalized feedback they received about their glycemic patterns—even among people without known diabetes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Margaret Crawford, Matthew Johnson, Kazanna C. Hames and Gregory J. Norman are employees of Dexcom, Inc. Ilene J. Klein is an employee of Healthstat, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.