
Abstract

Clinicians have huge amounts of patient information at the fingertips. Health informatics, through coded data, is expected to facilitate efficient decision making and improve care. Unfortunately physicians are bad coders, 1 and furthermore, the medical nomenclature available falls short. 2
Diabetes is a long-term condition where a poorly reflected timeline is clear, where care could be then undermined. Problem-orientated medical records have been found where Active Problems show simultaneously a combination of codes implying “Suspected diabetes,” “At risk of diabetes,” “Pre-diabetes,” “type I diabetes,” “type II diabetes,” and “Diabetes in remission” (see Figure 1).
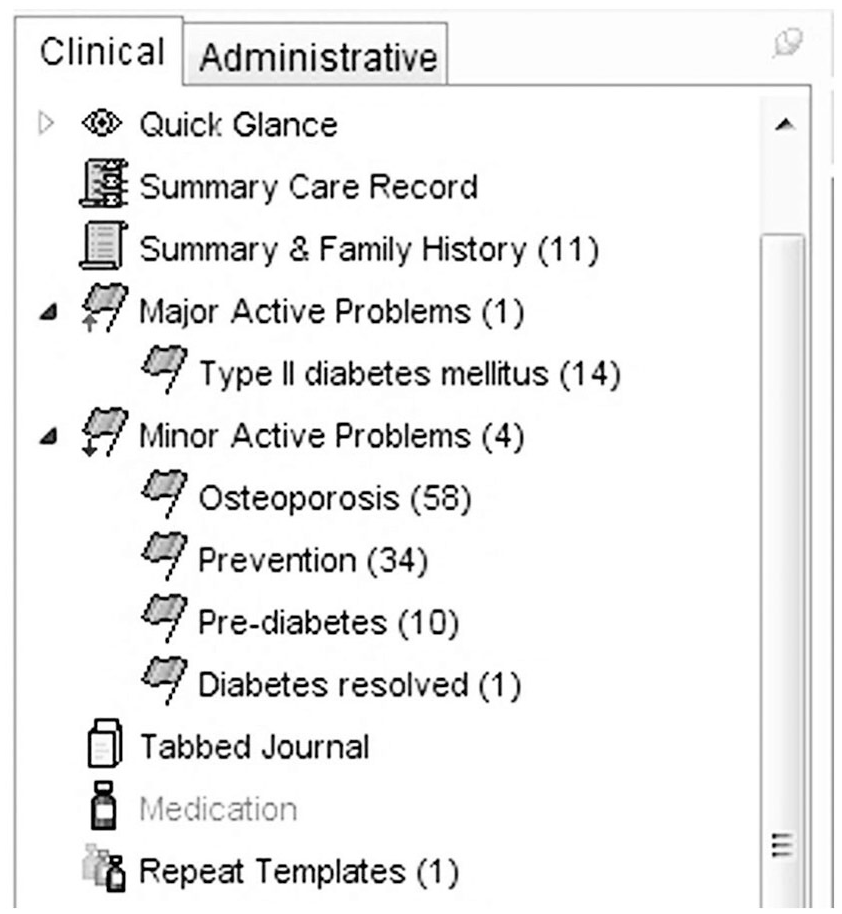
An inadequate active problem list.
Timeline is important, and an updated “Active Problem” is paramount. Unfortunately tidying up of the Problem List does not necessarily happen, 3 and general practitioners lack the time to keep the Problem List up-to-date. 4
There are coded clinical entries lacking coded dates: The user can omit dates, or add only month and/or year. The software handles it by creating an artificial date (eg, 1/1/1900 if undated), providing inaccuracy when related to other codes properly dated.
As information is shared among different organizations—their registered general practitioners, the out of hours services, community clinics providing foot care, eye care, . . . perhaps the hospice, and no doubt hospitals—there is a risk. Without sharing accurate information, without the time to confirm the adequate timescale of the entries, entry errors and interpretation faults are likely to be on the increase, and with that the prospect of iatrogenic consequences.
Electronic Health Records have been widely used by primary care in England for well over two decades 5 and appropriate coding is still poor. Other countries should assess as they embrace records digitalization if coding is as inadequate as in the United Kingdom.
In United Kingdom, SNOMED-CT nomenclature is used by all organizations, 6 it is a much vast than previously used ones in primary care.
Hierarchy of the nomenclature is not clear, with many codes representing the same condition. Software should facilitate creating a timeline. Coding needs to be adequately linked. A disease like diabetes type 2 may be suspected, confirmed, ruled out, complicated with other secondary conditions, resolved, relapsed. . . and having different codes expressing each stage unlinked prevents having a timeline that could help understanding clearly the condition and its management.
One has to wonder why, if medical records are to reflect current facts, there is no option to class any diagnostic code as “no longer current” or “currently considered an error” with the appropriate coded date. Clinical practice is to delete codes (mark them as errors) or to leave them alone. Both alternatives are wrong.
Coding needs to be simplified so busy clinicians use it instead of free text, or the huge opportunity that health informatics could provide is lost.
There is an urgent need to move from electronic papers to electronic interactive records, to use the benefits informatics can provide, and a review of the current medical code nomenclature should be a first step. Clinicians should demand a change that otherwise will not happen on its own.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.