
Abstract
Background:
Diabetes treatment and management provide a unique opportunity for examination of the effectiveness of electronic health records (EHRs) on patient health outcomes, continuity of care, and areas for further development. This systematic literature review was designed to identify the strengths and limitations of EHR and opportunities for improvement proposed in original research and recent rigorous systematic reviews.
Methods:
This review utilized methodology adapted from PRISMA. Inclusion criteria for original research were published between March 2003 and November 2017; included randomized controlled trial design with participants ≥18 years of age with diabetes diagnosis ≥1 year; measured outcomes included HbA1c, blood pressure, and LDL cholesterol levels. Criteria for systematic reviews included research focused on EHR outcomes, improvement of care for patients with diabetes, prevention of adverse outcomes, web-based communication, and limitations of EHR regarding chronic disease management. Thirteen articles qualified for inclusion.
Results:
Meta-synthesis of articles suggests that chronic disease patients benefit most by decision support tools that alert physicians of drug interactions, communication tools that keep them informed and engaged in their treatment regimens and detailed reporting and tracking designed to inform progress. Collective results suggest that EHR technology is advancing rapidly; however, patient outcomes documented via EHR systems remain largely unknown.
Conclusion:
A fertile area for inquiry designed to enhance patient outcomes in diabetes and chronic disease management is determining how EHR systems can be utilized for new drug and treatment options in addition to enhancing the quality, cost-effectiveness, and continuity of care.
In 2009, the American Recovery and Reinvestment Act mandated that all health care providers must adopt electronic health records (EHRs) by January 1, 2014. 1 The adoption of EHR has intended to make a variety of practice support procedures considerably more efficient. Progress note keeping, test ordering, and electronic prescribing seek to simplify and save time but EHR has also allowed for better data sharing between providers, the development of data-driven decision support mechanisms, utilization of new research capabilities, and more congruent chronic disease management (for a full list of benefits, see Table 1). 2 Diabetes management provides a unique opportunity for examination of the effectiveness of EHRs on patient health outcomes, continuity of care, and opportunities for further development.
EHR Advantages and Suggested Improvements.
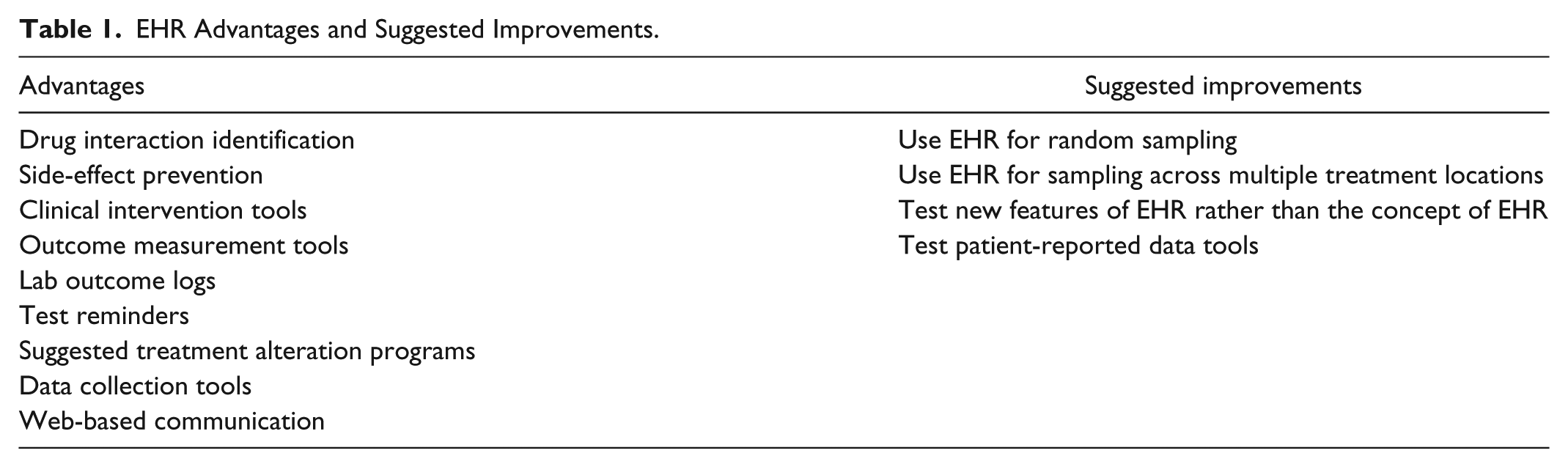
Many studies have sought to quantify benefits such as quality of care improvements, data tracking, cost reductions, and medical error minimization but a lack of consensus and inconsistent results leave the true effects of EHR widely unrecognized. As a condition requiring diligent supervision by primary care physicians, specialists, and patients, diabetes management provides a case study to evaluate the numerous effects EHR has on both quality of care and treatment outcomes.
This systematic literature review sought to uncover the major discrepancies in EHR research findings while describing the opportunities for improvement that have been proposed through a variety of analyses, experiments, and other published systematic reviews. By understanding the methodological flaws and author-acknowledged limitations in some studies, it is possible for researchers to retest the effects of certain aspects of EHR on a variety of outcome measurements to develop better clinical practices, technological advancements, and features for EHR software and workflow processes.
Methods
This systematic literature review utilized a methodology adapted from PRISMA as illustrated in Figure 1. After screening 1190 studies by title and abstract, the studies included in this systematic literature review met the following inclusion criteria.
Published between March 2003 and November 2017 or research conducted prior to 2003.
Employed a randomized or controlled trial design or be a systematic review of studies focused on EHR outcomes, improvement of care for patients with diabetes, prevention of adverse outcomes, web-based communication, and limitations of EHR regarding chronic disease management.
Diagnosed with diabetes or prescribed a medication expressly for the treatment of diabetes within the last year. Participants in randomized or controlled trials were 18 years of age or older.
Measured outcomes included HbA1C, blood pressure, and LDL cholesterol levels.
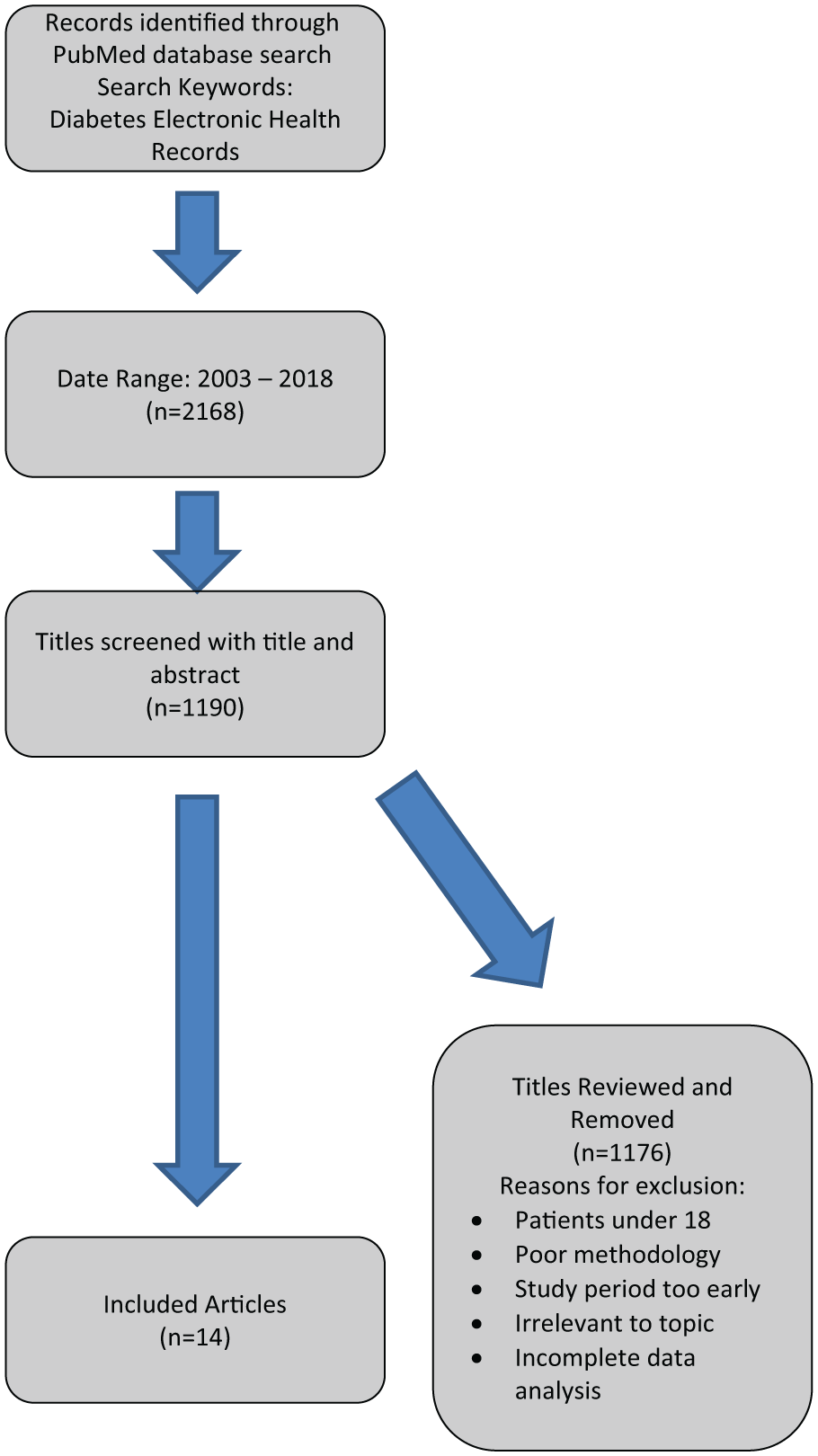
Article Review Methodology.
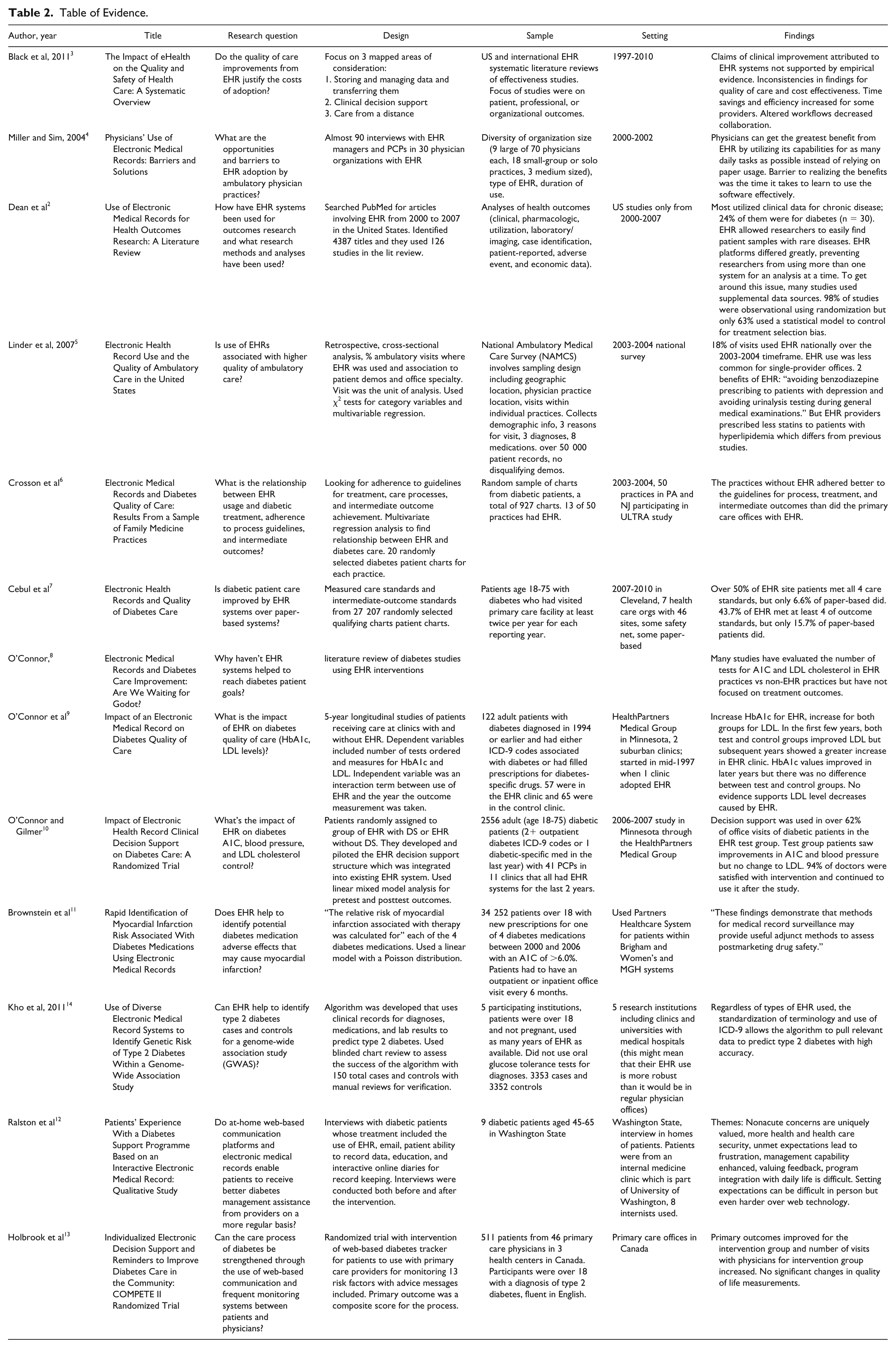
Table 2 presents information for each of these articles including design, sample, setting, and findings.
Table of Evidence.
Results
Previous studies have focused on a variety of uses of EHR systems as well as a variety of outcome measurements. To provide a comprehensive view of EHR effects for diabetes management specifically, results are categorized as either studies demonstrating improvement, focusing on prevention of adverse outcomes, or measuring successes of web-based communication systems.
Improvement Studies
Five of the publications analyzed in this systematic review focused on improvement of quality of care of patients with diabetes. Particular attention has been paid to process adherence, test ordering, decision support tools, and patient outcome measurements.
Focusing solely on practices in New Jersey and Pennsylvania between 2003 and 2004, Crosson and colleagues 6 conducted a multivariate regression analysis on data gathered from randomly selected charts of patients with diabetes from 50 practices to assess adherence to care processes, treatment guidelines, and intermediate outcomes measured by HbA1C, LDL cholesterol, and blood pressure. 6 Of the 50 medical practices, 13 were using EHR but had only adopted their systems within the last year through the Using Learning Teams for Reflective Adaption (ULTRA) study. Approximately 20 charts of patients with diabetes were randomly selected from each practice, leaving the researchers with a total of 927 for analysis.
The results of hierarchical logistic regression analysis showed, contrary to common belief, paper-based practices performed better with respect to adherence to process and treatment guidelines as well as intermediate outcomes as compared with practices using EHR systems. This suggests that the integration of EHR within medical offices either takes longer than a year or should be strengthened in the early stages. Furthermore, decision support tools within EHR might be useful in increasing practitioner adherence to processes and guidelines through the use of reminders for tests or follow-up questions and suggested treatment alterations.
Due to inexplicit data analysis methods, this study is difficult to replicate and the results cannot be generalized because the data were not representative of regional or national systems. This study, however, is a starting point for understanding the deficits of EHR systems for chronic disease patients. EHR does not guarantee a higher quality of care, just a higher quality of reporting.
Expanding the scope but focusing strictly on diabetic care and outcome standards, Cebul et al 7 conducted a cross-sectional multivariate regression analysis on the practice level using 27 207 randomly selected patient charts from 46 clinics in Cleveland from 2007 to 2010. Patients were 18 to 75 years of age and had visited a primary care facility at least twice per year in each of the reporting years. 7 The 46 practices were diverse in their use of EHR systems versus paper-based, patient population sizes, and demographics.
EHR system use was viewed as the treatment while care standards and intermediate-outcome standards served as the dependent/outcome variables. Care standards included a variety of tests, prescription, examinations, and vaccines, while intermediate-outcome standards were measurements against specified thresholds for blood pressure, LDL cholesterol, dosage of statin medications, body mass indices, and smoking status. The multivariate regressions showed that over 50% of patients being treated at EHR sites met all 4 care standards while only 6.6% of paper-based practice patients did. 7 The gap was slightly smaller for outcome standards where 43.7% of EHR practice patients versus 15.7% of paper-based practice patients met at least four of the outcome standards. While methodologically strong, there was potential for selection bias due to the observational nature of the study. Cebul et al provide no explanation for why the EHR practices outperformed the paper-based practices for both care and outcome standards.
Cofounder and codirector of HealthPartners Center for Chronic Care Innovation Patrick J. O’Connor, MD, MPH spent decades researching chronic disease management with a recent focus on EHR systems and their impact on patients with diabetes. In 2003, O’Connor published a literature review which pointed out that recent studies simply evaluated the number of A1C and LDL cholesterol tests through EHR versus paper-based practices rather than focusing on treatment outcomes. 8 Answering his own call for future research in 2005, O’Connor and his colleagues conducted a 5-year longitudinal study of 2 Minnesota suburban clinics starting in mid-1997 to assess EHR impacts on quality of diabetic care. One clinic had already adopted EHR in its early availability while the other remained paper-based, both with similar practice sizes and patient populations. A total of 122 adults who had been diagnosed with diabetes in 1994 or earlier were randomly selected. Fifty-seven were from the treatment group or the EHR based clinic. 9 The dependent variables included the number of tests ordered per patient and measurements of A1C and LDL cholesterol levels. The independent variable was an interaction term between the use of EHR and the year the outcome measurement was taken.
In the first few years of the study, results indicated that both groups improved LDL cholesterol levels but the benefits for the test group were greater in later years. A1C levels also improved over the course of the study but there was no significant difference between the improvements of treatment versus control group patients. The number of tests ordered by the EHR based clinic increased significantly, allowing the researchers to conclude that a focus needed to be placed on better treatment processes, not testing frequency. They advised that enhancements to EHR systems should be made to provide clinical decision support tools rather than simple test reminders. This preliminary and very early study was limited by its small sample size and only two testing sites. In a 2011 study, O’Connor and two of his previous collaborators reconvened with new collaborators to retest the effects of EHR systems after implementing their own custom-designed decision support tool for EHR practices in Minnesota through the HealthPartners Medical Group.
Conducted in 2006-2007, this randomized trial included 41 primary care physicians in 11 clinics that had been using EHR for at least the last two years. A total of 2556 adults with diabetes were randomly assigned to treatment groups using EHR systems outfitted with the new decision support tool or to control groups which utilized EHR systems without the decision support tool. The same outcome measurements from the 2005 study of A1C and LDL cholesterol were used with the addition of blood pressure.
The decision support tool, which served as the treatment, was capable of providing recommendations for medications and dosages based on current treatment plans and the distances patients were from achieving their clinical goals. 10 The algorithm informing the decision support tool also took comorbidities and renal function into consideration and was able to alert physicians of potential drug interactions. Of all 1652 office visits of patients with diabetes in the treatment groups, over 62% utilized the decision support tool. More than 94% of the physicians expressed satisfaction with the intervention and many continued to utilize the decision support functionality after the trial concluded.
Using a linear mixed model analysis for pre- and post-test outcomes, O’Connor et al found that the test group patients saw improvement in their A1C levels and blood pressure but no significant changes in LDL cholesterol. This study demonstrates that fully integrated decision support tools within EHR systems can improve the quality of care and measured outcomes for patients with diabetes. These findings conflict with some previous studies that focus on decision support tools that are only capable of sending test ordering reminders or general prompts.
Prevention of Adverse Outcomes and Diagnostic Tools
Several relatively recent studies have demonstrated that EHR systems have previously unrecognized capabilities as side-effect prevention and diagnostic tools. These are particularly useful tools for diabetic treatment due to the differences in commonly prescribed diabetes medications, potential for myocardial infarction, and hazards of combining medications. 11
Brownstein et al’s 11 signal detection analysis of four common diabetes medications (sulfonylurea, metformin, rosiglitazone, or pioglitazone) and their associated risk of myocardial infarction involved over 34 000 patients within the Brigham and Women’s and Massachusetts General Hospital systems. All patients met the inclusion criteria, had an A1C of 6.0% or higher, and had been prescribed one of the four diabetes medications between 2000 and 2006. Patients who were prescribed more than one medication were excluded from the study as were patients who had out-patient office visits less frequently than every 6 months. The dependent/outcome variable of the analysis was the need for hospitalization due to acute myocardial infarction. Using a cumulative temporal approach, the researchers were able to identify increased myocardial infarction risk within 18 months of risk ratio thresholds for each of the four medications using features within EHR systems. A comparator group of patients exhibited lower risk of myocardial infarction and was treated with an oral medication and was not exposed to rosiglitazone.
All data for this study were obtained through the Partners Healthcare Network so there is potential for incomplete prescription data for any patients who received prescriptions from physicians outside of the network. Despite this limitation, Brownstein et al’s work exemplifies how EHR systems can be used as alternative drug evaluation methods to identify risks from medication use and interactions before serious complications arise.
After developing an algorithm to be integrated into EHR systems, Kho et al 14 assessed the program’s ability to use EHR data to identify patients at risk for type 2 diabetes for the purposes of collecting groups of these cases and controls for use in genome-wide association studies. The algorithm uses clinical diagnosis records, medications, and lab results to predict risk but did not utilize oral glucose tolerance test results. Nearly 7000 patient charts from 5 participating institutions were randomly selected to test whether the algorithm could distinguish between type 1 and type 2 diabetes. Because the algorithm used ICD-9 (International Classification of Diseases) codes that standardize terminology, cases could be categorized regardless of EHR system. 14 After running the algorithm, 150 selected patient charts were subjected to a blinded manual review for verification which found that the algorithm had properly identified 98% of the cases.
These two experiments illustrate that while EHR systems may be able to increase quality of care and treatment outcomes for patients with diabetes through decision supports, they can also be used as data collection tools. By building and integrating new tools into existing systems, physicians can be alerted of potential risks of both disease development as well as adverse reactions to medications. If used effectively, EHR can contribute to better preventative measures and early and more adaptive treatment of chronic diseases.
Web-Based Communication and Monitoring
Some electronic health systems come equipped with communication channels that enable patients to correspond directly with providers. This feature can facilitate frequent progress updates (outside of office visits) from patients with complex diagnoses or those with mobility issues. Two complementary studies by Ralston et al 12 and Holbrook et al 13 provide insights into the successes of EHR patient participation.
By conducting a qualitative study using interviews with patients with diabetes, Ralston et al assessed the effectiveness of their new diabetes support program in meeting patient needs and expectations for the purposes of self-management support. Eight internists practicing at a University of Washington clinic were selected for the trial along with a total of nine patients with diabetes between the ages of 45 and 65. 12 Interviews with the patients were conducted in their homes, once before the trial began, and again six months after enrollment. The program allowed for email correspondence, education portals and handouts, and interactive online diaries for patients to record data and access to test results.
Interviews revealed that expectation setting is vital to patient perception of the value of the program but expectations were best set in person than by Internet communications. Major benefits of the program were features that allowed patients to take a more active role in their own medical care. First, Internet-based communication allowed providers to answer questions at their convenience which enabled them to send more thoughtful information, thus increasing patient perception of being taken care of. Similarly, nurses would reach out to patients if they saw something unusual in the patient daily logs. Finally, having access to their test results empowered patients to take control of their medical care and ask better questions. While this study did not assess treatment outcomes, a study conducted by Holbrook et al 13 in Canada helped to fill this knowledge gap.
Using three health centers in Canada involving 46 primary care providers and 511 type 2 diabetes patients, Holbrook et al conducted a randomized trial with the intervention of a web-based diabetes tracker and message center. The web-based program was developed through the Computerization of Medical Practices for the Enhancement of Therapeutic Effectiveness study II. 13 Statisticians blind to patient allocation to the groups conducted t-tests to assess the differences between the treatment and control groups. Primary outcomes were process improvement measurements including tests such as blood pressure, BMI, LDL cholesterol, foot check, and smoking status, while secondary outcomes evaluated the results against baselines and targets. The intervention group met more of the primary outcomes and saw more improvement with secondary outcomes as compared to the control group. In addition, a 6-month questionnaire revealed that the intervention group members had greater optimism in their diabetes management, quality of care, and relationship with their doctors. This was also evidenced by the treatment group’s better office appointment attendance.
From these two studies, it is evident that web-based communication with patients diagnosed with chronic diseases can empower patients to take a more active role in their health care, allow for the development of stronger relationships and trust between health care providers and patients, and perhaps lead to better health outcomes.
Goldstein et al 15 conducted a systematic review of 107 articles published between 2009 and 2014 in informatics, health services, and medical journals to assess how other studies have used EHR data to predict an outcome. Five of those papers strictly focused on diabetes or diabetic remission as the outcome. 15 The authors found that a considerable advantage of EHR data was the ability to use regional hospital networks in research studies. Reliability of internal data was increased as all patient visits across all provider locations were captured, thus strengthening prediction models. Goldstein et al raise an important question as to whether optimization of prediction models should be on regional or network level or be generalizable. Regardless, the authors find that more must be done to verify results of prediction models across networks and centers. They recommend external validation, analysis of longitudinal data which is readily available through EHR, and use of evaluation metrics.
Discussion and Conclusion
The advancements made to EHRs have changed the landscape of medical care across the US and globally. While the benefits and shortcomings of this technology have influenced the way researchers study diseases and medical care appears to be more integrated, the actual patient outcomes of these systems remain largely unknown.
The methodology employed by the studies analyzed in this literature review are robust in terms of randomization for controlled trials but often only reflect on one aspect of care rather than the entire system of practitioners, diagnoses, treatment coordination, patient participation, and ultimate outcomes. Due to the variability between experiences of different sizes and demographic characteristics of medical practices and their patients, it is nearly impossible to generalize EHR experiences across large, diverse populations. There is expansive space for further research in EHR ranging from how systems can be better utilized for new drug and treatment options for chronic diseases, benefits of personalized patient portals and daily diaries, and diagnostic support tool optimization possibilities. As new opportunities for further development are being explored, the design of new features should be tested using randomized studies to strengthen researchers’ understanding of effects with a more representative method.
This systematic review reveals that EHR has progressed substantially in providing benefits to both patients and practitioners. Chronic disease patients seem to benefit most by decision support tools that alert physicians of drug interactions, communication tools that keep them informed and participating in their treatments, and detailed reporting and tracking that informs progress without over-testing. As EHR technology continues to improve, it is likely that the treatment outcomes of chronic disease patients will also improve considerably.
Footnotes
Abbreviations
EHR, electronic health record; LDL, low-density lipoprotein.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.