
Abstract
Background:
These 2011-2013 analyses examined the authors’ hypothesis that relative diabetes care order changes would be measured after electronic health record (EHR) implementation for 291 Medicaid adults who received all of their office-based care at one midwestern federally qualified health center (FQHC) over a 24-month period (n = 2727 encounters, 2489 claims).
Method:
Beneficiary sociodemographic, clinical, and claims data were validated with clinic EHR and state Medicaid claims linked to providers’ national identifier numbers. Overall pre-post order rate comparisons, and a series of controlled within group binary logistic models were conducted under penalized maximum likelihood estimation terms.
Results:
After EHR implementation, both the overall order rates and odds ratios of per beneficiary hemoglobin A1C (HbA1C) orders increased significantly (ie, from mean of 0.65 [SD = 1.19] annual tests to 0.96 tests [SD = 1.24] [P < .001]). Although the overall post-EHR order rates of dilated eye exams and microalbumin urine tests appeared fairly stable, the odds of eye exam orders being placed at the claims level decreased significantly (OR = 0.774, P = .0030).
Conclusions:
These mixed results provide evidence of the varied diabetes care ordering patterns likely seen from increased office use of EHR technologies. The authors attempt to explain these post-EHR differences (or lack of) that generally resemble some of the authors’ results from another funded project. Ideally, these findings provide Medicaid and health care officials with a more realistic indication of how EHRs may, or may not, influence diabetes care ordering patterns for vulnerable lower-income primary health care consumers.
With the passage of the Health Information Technology for Economic and Clinical Health Act, 1 the federal government and states have offered considerable incentives for office-based providers to use electronic health records (EHR).2,3 In 2011, the Michigan (MI) Medicaid program began paying such EHR incentives to providers. 4
A growing number of recent studies have initially suggested that overall efficiency and guideline-adherent ordering patterns may be influenced for certain chronic conditions by the use of ambulatory EHR systems.5-17 Still, it is also clearly evident that the majority of the pre-post EHR projects to date have been conducted in hospitals.8-10,14,16 An increasing group of experts have therefore suggested that more controlled pre-post EHR analyses are required in ambulatory settings and/or with more vulnerable and lower-income adults.5,7-9,11,12,17 The manner in which EHR use may impact diabetes care adherence to major American Diabetes Association (ADA) guidelines 18 for annual tests and procedures also remains largely unknown.
Objective
The purpose of these covariate-controlled analyses was to evaluate how the use of a federally certified office EHR system in one setting might be associated with changes in three common diabetes care tests (ie, hemoglobin A1C [HbA1C], dilated eye exams, and microalbumin urine) for adults with different characteristics. For these analyses, a sample of continuously and exclusively covered MI Medicaid adults confirmed to have received all of their office-based care for an established diagnosis of diabetes at the same midwestern federally qualified health center (FQHC) during a 24-month (ie, 12 months pre-EHR and 12 months post-EHR) analytic period were followed.
Subjects
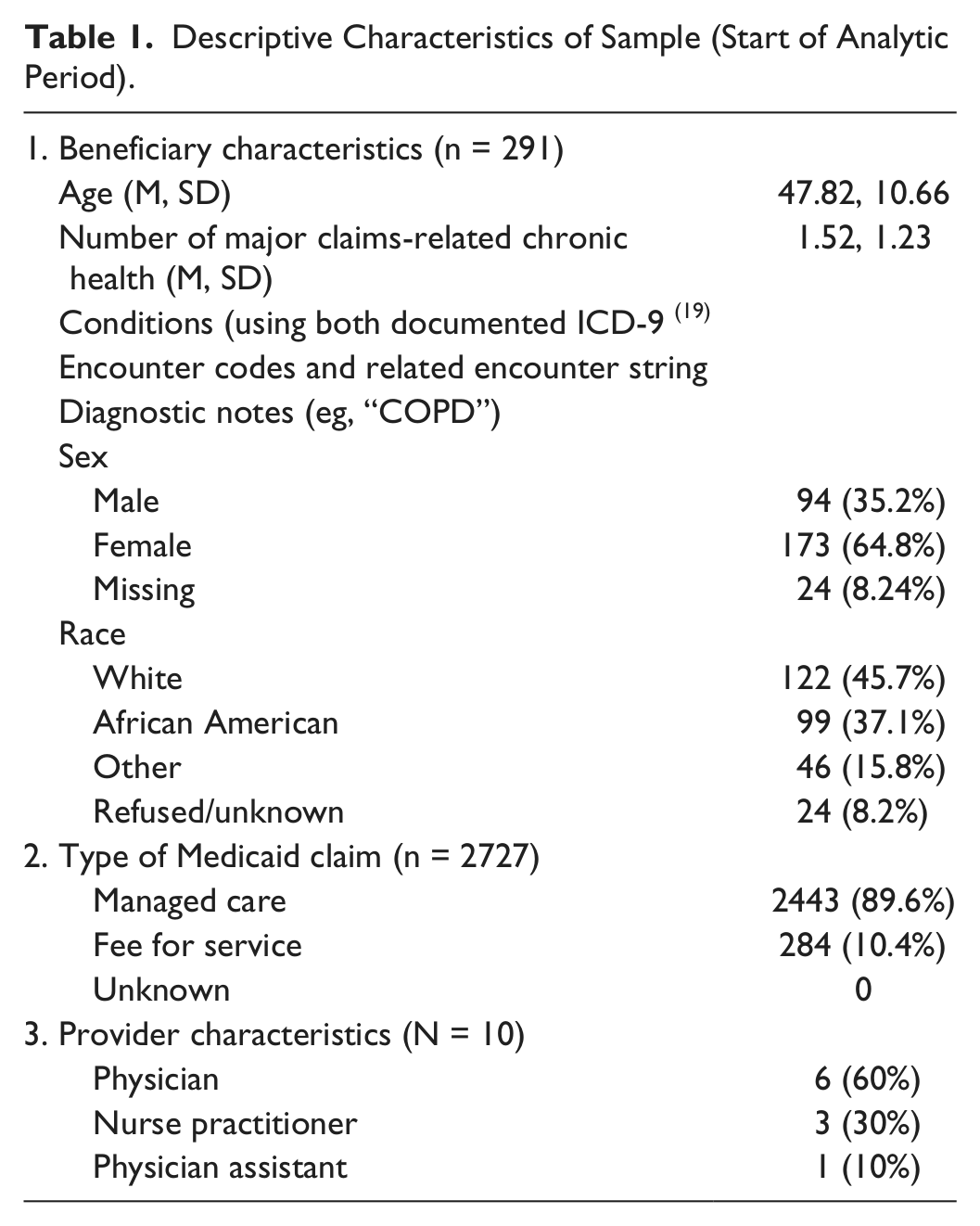
The analytic sample was comprised of all continuously enrolled MI Medicaid-covered adults at one midwestern FQHC who had (1) each been earlier diagnosed with some form of International Classification of Disease, 9th edition (ICD-9 coded 19 diabetes mellitus and (2) received all of their office-based care in this setting during the 24-month analytic period. The final working sample of 291 adults with at least one documented office visit encounter during the 24 months were included out of 891 total patients who were later determined to possibly possess inconsistent Medicaid coverage or had no encounter claims of any type.
Methods
Analytic Design
These retrospective analyses used a pre-post within group design to compare the order patterns of three major diabetes tests before, and after, the same FQHC clinic of 10 providers had fully implemented a federally certified EHR. The study had been approved by the FQHC board of directors and was found to be exempt from institutional review board review by the authors’ university as non–human subjects research using deidentified data.
Beneficiaries were linked to this particular setting by the designated honest broker at the authors’ Institute for Health Policy based on unique MI Department of Community Health (MDCH) master beneficiary record numbers. 20 All beneficiary sociodemographic, Medicaid coverage, and office diabetes claims data from the 24-month period were extracted from the MI Medicaid Data Warehouse from MDCH. 20 This reporting source of all statewide Medicaid lab and procedure claims was optimal since every single lab test/procedure claim that was ever ordered (through paper-based or EHR system), received and approved by the MI State Medicaid Program office during the period was included in these analyses of Medicaid-only patients. Although the authors could not precisely measure the proportion of unclaimed (ie, ordered, but never received) lab and procedure services, they could confirm that they had the entirety of approved claims from state MDCH claims for the entire 24-month period for their analyses. Complete provider data were obtained from state office processing provider EHR attestation applications, and cross-checked with state of MI licensure date and federal National Provider Identifier (NPI) numbers. 21
Study Measures
Diabetes Care Claims Measures
A total of 78 Current Procedural Technology 22 codes of the three laboratory tests were examined to most comprehensively capture all office diabetes care order claims:
HbA1C tests (6 codes)
Dilated eye exams (59 codes);
Microalbumin urine test codes (excluding patients with prior history of proteinurea or significant renal diagnoses): (12 codes)
Beneficiary-Level Factors
Over 90% complete data concerning the following beneficiary characteristics were included in each of the analytic models:
Age (in complete years)
Sex
Categorized racial/ethnic affiliation
Composite comorbidity (based on total number of all documented claims-related ICD-9 18 diagnoses during the 24 months)
Predominate type of Medicaid coverage (ie, managed care or fee-for-service)
Note: Marital status was not included into models due to 72.7% missing data.
Note: Although it is possible that some sample patients could have possessed certain additional chronic conditions that were not coded during their pre- and post-EHR analytic period encounters, the authors have concluded from other works that this is infrequently the case when working with both ICD-9 19 codes and encounter diagnostic notes data from MI Medicaid settings over such an extensive two-year period.17,23
Note: Although each working sample adult had at least one office visit claim during the entire 24-month analytic period, the authors opted to not to try to control for number of office visits since it was very unclear in some cases which visits were entirely or partially diabetes-related, which visits were for other discrete needs. In effect, those diagnoses codes once entered on one encounter and apparently carried over during the post-EHR period encounters by this particular setting EHR.
Analyses
All project analyses were conducted using Statistical Analysis Software 9.4 (SAS). 24 Descriptive statistics (Table 1) and a series of cross-tabulation charts were first generated to summarize the distribution of the characteristics of the sample beneficiaries and providers and both pre- and post-EHR order rates. Along with overall pre-post rate comparisons, a series of covariate-controlled within group (ie, 12 months pre- and 12 months post-EHR full implementation date, for the same adults linked to a single FQHC provider) binary logistic models were then completed under penalized maximum likelihood estimation procedures by using the Firth statement in the selected software25,26 were then conducted.
Descriptive Characteristics of Sample (Start of Analytic Period).
When possible, terms including beneficiary age, sex, reported racial/ethnic affiliation, and composite level of comorbid conditions were included into these initial models, with significant software convergence and differentiation problems imposed from the physician versus nonphysician order model term, which was not successfully included into any model.
Results
Number of Office Visits
A total of 1317 claims (48.3% of total) office visit encounters were documented during the 12 pre-EHR months, compared to 1410 (51.7%) encounters during the post-HER months. Sample patients during the pre-EHR 12-month period averaged 4.53 total office visit encounters, while the same patients averaged 4.84 total office visits during the post-EHR period. As indicated earlier in this article, the authors were unable to precisely gauge which office visits were entirely or partially diabetes-related, particularly during the post-EHR period in which diabetes diagnoses codes entered during earlier encounters were apparently carried over to the current office visit by this particular EHR.
Overall Pre-Post EHR Order Rates
The overall order rates for HbA1C tests increased significantly post-EHR per individual beneficiary from a mean of 0.65 (SD = 1.19) annual tests per year to 0.96 annual tests (SD = 1.24) (P = .0002). The overall order rates for dilated eye exams decreased very slightly per individual beneficiary after EHR from a mean of 3.16 (SD = 4.06) annual tests per year to 3.14 annual tests (SD = 3.93), although the odds ratio coefficient depicted in Table 2 was significant at the claims level (OR = 0.774, P = .003). Also, the overall (infrequent) order rates for microalbumin tests increased somewhat per individual beneficiary after EHR from a mean of 0.27 (SD = 0.654) annual tests per year before EHR to a mean of 0.36 (SD = 0.80) (P = .343).
Odds Ratio of Receiving One or More Diabetes-Related Test/Procedure After EHR Implementation (Binary Logit Penalized Maximum Likelihood Estimate Models) (N = 2727 Encounters, 2489 Claims).
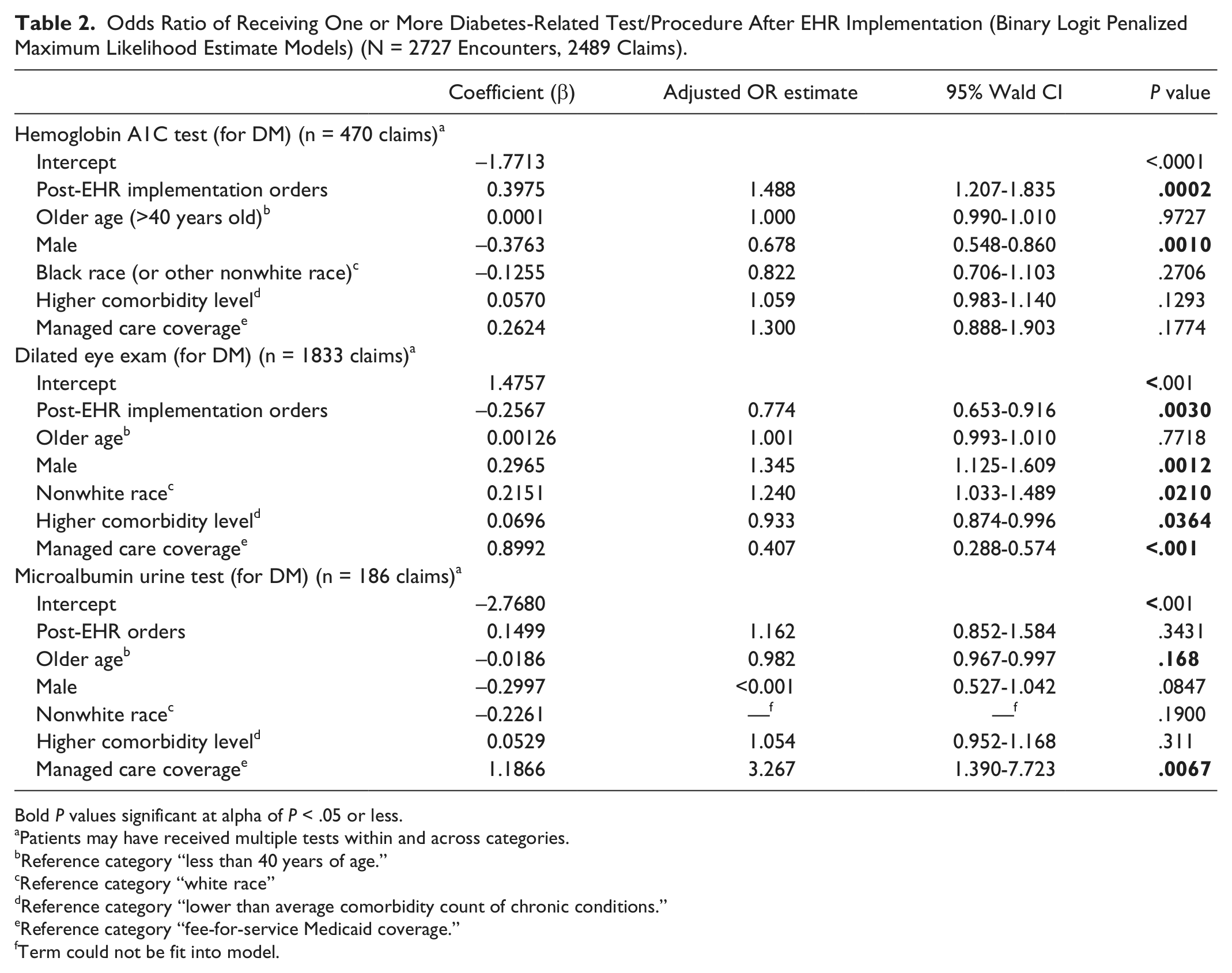
Bold P values significant at alpha of P < .05 or less.
Patients may have received multiple tests within and across categories.
Reference category “less than 40 years of age.”
Reference category “white race”
Reference category “lower than average comorbidity count of chronic conditions.”
Reference category “fee-for-service Medicaid coverage.”
Term could not be fit into model.
Pre-Post EHR Odds Ratios
As can be seen in Table 2, the adjusted odds of those beneficiaries with diabetes receiving one or more HbA1C test increased significantly during the post-EHR implementation months compared to pre-EHR claim rates (post-EHR OR point estimate = 1.448, P = .0002). However, the odds of received one or more forms of dilated exam for each diabetes patient decreased significantly during the same post-EHR period (post-EHR OR = 0.774, P = .0030). There were no significant pre-post change in rates of microalbumin tests after EHR implementation (post-EHR OR = 1.162, P = .3431).
In this sample, beneficiaries who were older, were more comorbid, were female, reported a nonwhite race, and/or were covered under Medicaid managed care terms demonstrated overall lower outcome likelihoods. In terms of the covariates successfully entered in these binary models, older adults, females, those with a higher level of comorbidity, and/or nonwhite beneficiaries demonstrated lower (significant or nonsignificant) effects on outcome likelihoods. Notably, those adults covered under Medicaid managed care terms received significantly fewer orders for all but the HbA1C outcome.
Discussion
These mixed results provide some of the first evidence of the varied changes likely to be measured in diabetes claims patterns from increased office-based use of EHR technologies. Although the authors are unable to fully explain these post-EHR differences (or lack of), they generally resemble some of the authors’ recent mixed results from another funded project concerning pre- and post-EHR preventive screening order patterns in a sample of over 10 000 MI Medicaid beneficiaries. 23 Other studies have shown somewhat similar mixed results in certain patient subgroups.5-7,11-14
Of course, these findings are subject to some inherent data-related limitations. The authors could not precisely discern from these claims data what proportion of diabetes tests may have actually been ordered and never completed due to variability among beneficiaries (eg, not coming to scheduled office visits, lacking subsequent transportation to have lab specimens obtained, functional limitations, etc). Neither were the authors able to model out potential pre-post EHR ordering differences of physician to nonphysicians for any selected outcome. We may have also lacked an adequate level of statistical power to detect significant pre to post differences in microalbumin order rates since we only collected data concerning 186 such tests for the entire 24-month analytic period.
At the same time, this sample of 291 patients was the same set of individuals before and after EHR implementation, albeit from a single midwestern setting with 10 providers, which could limit the generalizability of these results. Unless the clinical needs of these adults (ie, diabetes-related and otherwise) became considerably different after EHR compared to the pre-EHR months, these analyses may provide a unique context through which to understand what such systems may or may not be realistically capable of influencing during initial postimplementation months.
Conclusions
We can never realistically expect that EHR and administrative claims data will ever be capable of telling the full story for inherently vulnerable Medicaid beneficiaries. We should also acknowledge that our results may have been subject to considerable variations in how even this small group of 10 providers may have actually used the functionalities of their shared EHR for diabetes care during 12 postimplementation months. Primary care providers may simply require more than 12 months to fully capitalize on what EHR systems could contribute to the time-intensive office visit care provided complex lower-income health care consumers.
More focused larger-scale analyses with more heterogeneous samples of different types of providers and non-Medicaid-covered patients over longer periods comparing the varied ordering pattern changes derived from different EHR products for chronic health care will certainly be required.5,7,14,23 Ideally, these findings will provide Medicaid and other health care officials with a more realistic indication of how EHRs may, or may not, influence diabetes care ordering patterns for vulnerable lower-income primary health care consumers receiving care in FQHC settings.
Footnotes
Acknowledgements
The authors acknowledge Lori Baird, Ingham County Health Department, Lansing, MI; Jason Werner at the Michigan Department of Community Health (for providing statewide Medicaid EHR Incentive Program, Lansing, MI; and Robert Orem, Michigan State University Institute for Health Policy, serving as “honest broker,” East Lansing, MI.
Abbreviations
ADA, American Diabetes Association; EHR, electronic health record; FQHC, federally qualified health center; HbA1C, hemoglobin A1C; ICD-9, International Classification of Disease, 9th edition; MDCH, Michigan Department of Community Health; MI, Michigan; NPI, National Provider Identifier.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Health and Human Services/MI Department of Community Health, RC103164 2013 Health Information Technology Resource Center, 10/01/2013-09/30/2014 (WC, principal investigator).