
Abstract
Understanding all aspects of diabetes treatment is hindered by the complexity of this chronic disease and its multifaceted complications and comorbidities, including social and financial impacts. In vivo studies as well as clinical trials provided invaluable information for unraveling not only metabolic processes but also risk estimations of, for example, complications. These approaches are often time- and cost-consuming and have frequently been supported by simulation models. Simulation models provide the opportunity to investigate diabetes treatment from additional viewpoints and with alternative objectives. This review presents selected models focusing either on metabolic processes or risk estimations and financial outcomes to provide a basic insight into this complex subject. It also discusses opportunities and challenges of modeling diabetes.
Diabetes mellitus is a chronic and complex disease with multifaceted complications and comorbidities. 1 Looking at cause-specific mortality, diabetes is ranked fifth place, 2 underlining the importance of understanding treatment of this chronic disease in detail. Basic research and clinical trials are key instruments to investigate fundamental disease related processes such as glucose turn-over as well as efficacy and safety of antidiabetic medication. Clinical trials also provide information on cost effectiveness of treatment options or (long-term) side effects of antidiabetic therapy on patients.
A study area, which applies mathematical algorithms to simulate diabetes and its potential outcomes, has gained increasing attention.3-5 These approaches include the modeling of biological processes such as insulin receptor dynamics or whole-body insulin-glucose dynamics, economic interests such as diabetes costs effectiveness but also diagnostic tests such as glucose tolerance tests. In addition, complex scenarios such as study outcomes and disease progression can be simulated.6-8 The latter can be used to support and verify clinical trials (eg, McEwan et al, 9 Eddy and Schlessinger, 10 Valentine et al, 11 Heijden et al, 12 American Diabetes Association, 13 Palmer et al 14 ). These models are often extrapolations or statistical junctions that are based on epidemiologic data used to estimate expectable effects and the joined costs. In 2004 guidelines for the modeling of diabetes and its complications were introduced by the American Diabetes Association (ADA; reviewed in Philips et al 15 ) relating to transparency, data, consistency, and validation of the models to assess the quality of the simulated results. 16 The Mount Hood Diabetes Challenges Network provides a platform to validate simulations by “challenging” models to verify various study outcomes in a competitive environment.10,11 In the last decade, the Food and Drug Administration (FDA) proceeded to accept simulation models for the approval of a variety of medical devices. The UVa/Padova Type 1 Diabetes Metabolic Simulator (T1DMS) was accepted in 2008 as the first in silico model that can substitute for animal studies in the preclinical testing of diabetes treatment by means of artificial pancreas (AP) systems. 17 We aim at providing a basic understanding of modeling in diabetes by giving an overview of selected, important in silico models for metabolic processes and clinical outcomes in diabetes treatment as well as discussing their advantages and disadvantages. The models presented in this review were chosen as representative examples for the according model type. We did not do a full literature search, as this article does not intend to provide a complete summary of modeling in diabetes but rather give insight into specific publications.
Current Status
In general, a model is defined as a representation of an object or a process that is frequently used for simplification. It can either describe parts of a complex system or depict the system as a whole. A model can be a physical as well as a mathematical representation. In contrast, a simulation is used to generate behavior of a model. It is used to change parameters of a model to predict outcomes. 18
Metabolic and Measurement Models
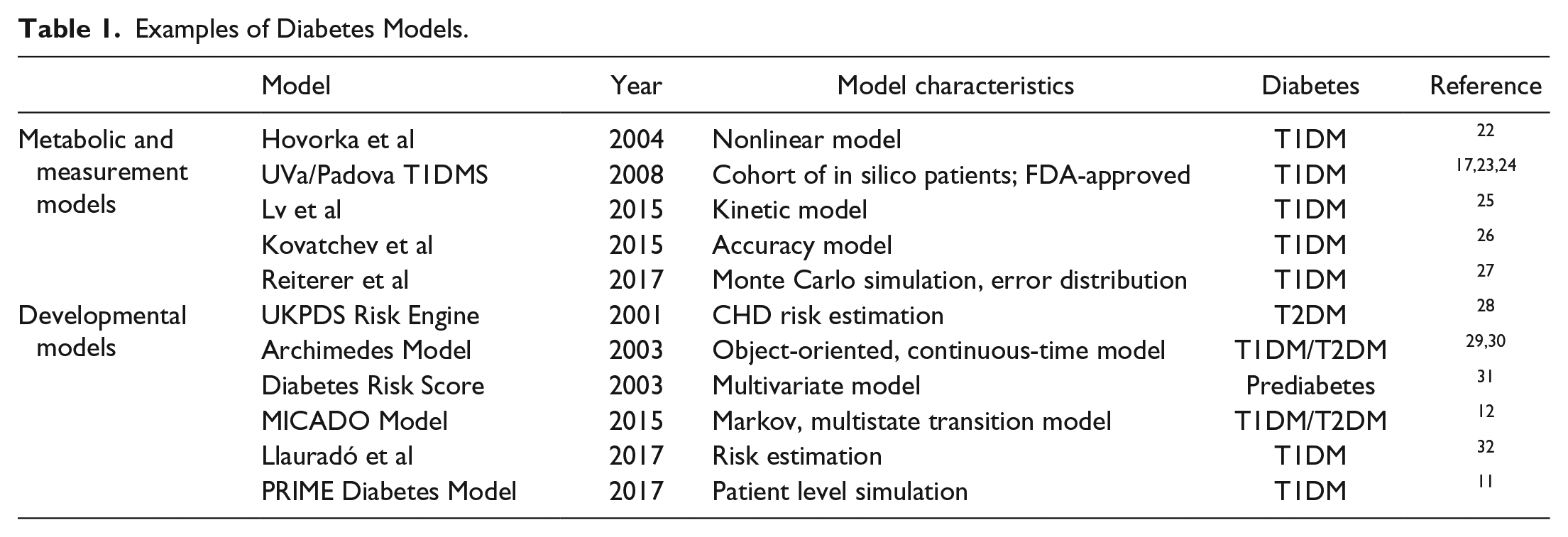
Models and simulations that aim to describe processes related to diabetes such as glucose dynamics, transport of insulin but also accuracy of glucose measurements are summarized here under the term metabolic and measurement models. These processes are difficult to assess in vivo and therefore understanding especially of metabolic processes can benefit from the use of such mathematical approaches. The next paragraph briefly presents examples of metabolic and measurement models that may be representative of this group (Tables 1 and 2). A number of other review articles specific to metabolic models provide additional information.1,19-21
Examples of Diabetes Models.
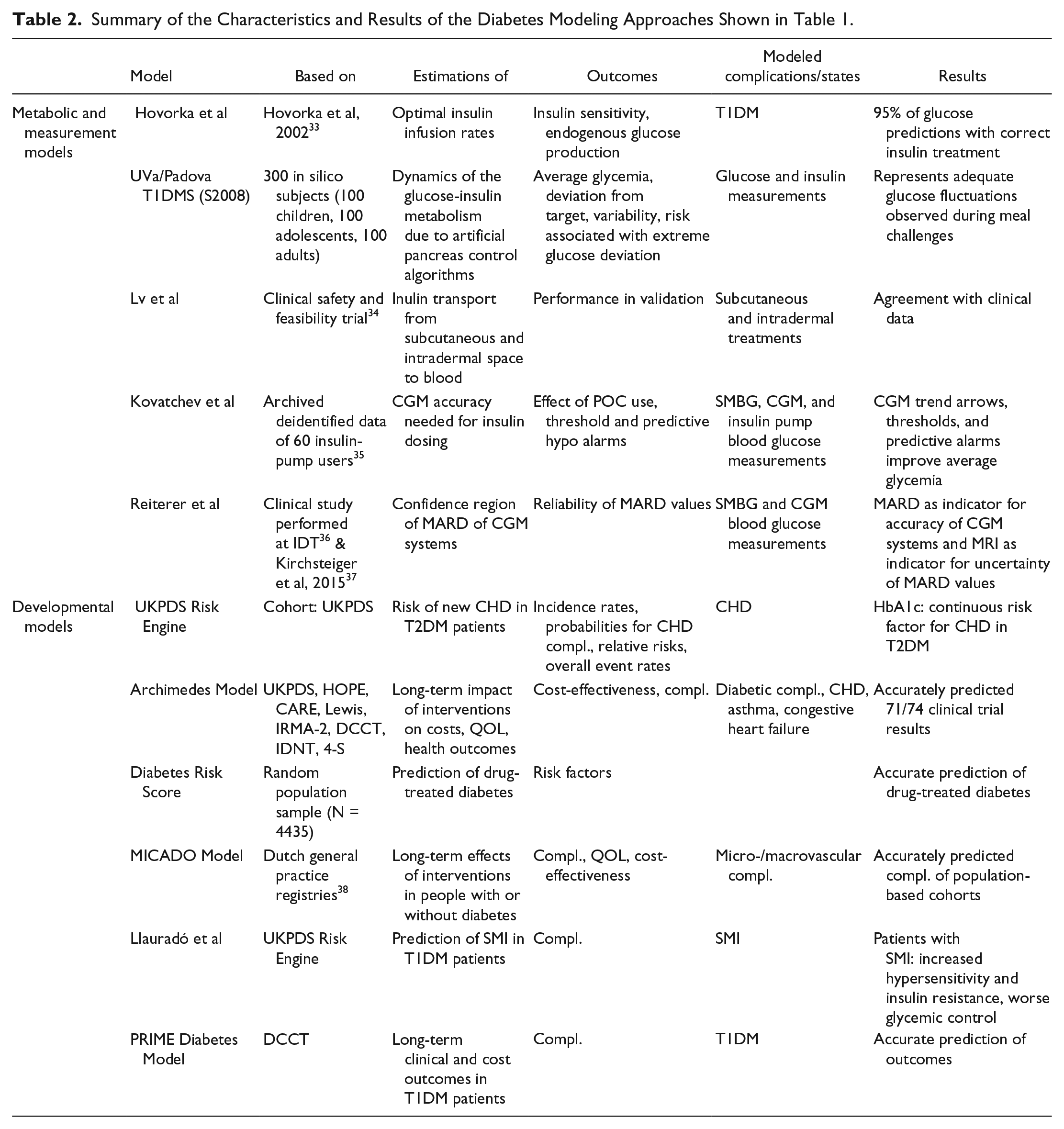
Summary of the Characteristics and Results of the Diabetes Modeling Approaches Shown in Table 1.
Glucose Dynamics and Insulin Transport
In 2004 Hovorka et al developed a nonlinear model for glucose kinetics aiming to control blood glucose (BG) levels especially during the night, allowing subjects with type 1 diabetes mellitus (T1DM) to start the day in euglycemic conditions.
The mathematical model links insulin delivery to BG excursions and uses model-predicted glucose levels to determine optimal insulin application rates. This allows adaptation both to a particular subject and to the time-varying characteristics of the glucoregulatory system. 22
The UVa/Padova model aimed to support the development of an AP system by simulating the dynamics of the glucose-insulin metabolism of subjects with T1DM. Realistic simulation provides a reliable connection between continuous glucose monitoring (CGM) in the interstitial fluid in the subcutaneous tissue and continuous subcutaneous insulin delivery via an insulin pump (CSII) based on appropriate control algorithms. The model consists of a set of continuous-time differential equations with several subsystems: for example, an insulin subsystem, one for meal glucose absorption, and one for glucose kinetics. The simulator has been accepted in 2008 by the FDA as a substitute for animal trials in the preclinical testing of closed-loop control strategies.17,23 Since its development, the UVa/Padova model has frequently been updated and extended.24,39-41
Pharmacokinetic (PK) models describing the transport of insulin from the application site in the subcutaneous tissue into to the blood stream are part of in silico platforms for developing and testing of insulin delivery strategies for diabetes treatment. In 2015 Lv et al presented a new mathematical model of fast-acting insulin analogs transport from subcutaneous and intradermal spaces to blood on the basis of nine existing models. The newly developed model has an increasing complexity and coincides better with the clinical data as compared to commonly used models. It is expected to improve the in silico development and testing of insulin treatment strategies, including AP systems. 25
Diabetes Management With BGM Systems
As it is important to ensure reliability of glucose measurements, there are a number of models that investigate the accuracy of BGM systems and relations to diabetic management. Using Monte Carlo simulation, Boyd and Bruns modeled glucose values measured with imprecise glucose meters to investigate the influence of this imprecision and bias on insulin dosing errors 42 and clinical outcomes. 43 Based on the original model Karon and colleagues simulated the effect of various glucose meter errors on insulin dosing decisions in patients with tight glycemic control. 44 In three independent calculations Breton and Kovatchev simulated the impact of SMBG accuracy on risk for hypoglycemia, glucose variability, and long-term glycemic control, observing a substantial decrease in glycemic control with increasing SMBG errors. 45 Further models, for example the model of SMBG measurement error, were incorporated into the most recent version of the UVa/Padova model.24,40
Diabetes Management With CGM Systems
Similarly a number of models investigate the accuracy of CGM systems. Kovatchev and colleagues examined the influence of inherent CGM errors on the quality of glycemic control and aimed to characterize which accuracy levels of CGM systems are needed for insulin dosing. The basic idea was to use real-life “true” glucose traces and then replay in silico “what-if” treatment scenarios. This allows to evaluate how dosing errors/hypoglycemia risk increases with gradually increasing sensor errors. The parameter used was the MARD (mean absolute relative difference), this is used most often to characterize the analytical performance of CGM systems. The modeling outcome of increasing the MARD from 3% to 22% showed that using CGM values for insulin dosing decisions is feasible. It was discussed that MARD = 10% can be seen as a cutoff value, below which sensor accuracy does not contribute to better glycemic outcomes. 26
Two other studies based on mathematical methods investigated the significance and validity of MARD as a reliable value to compare the accuracy and performance of CGM systems. Kirchsteiger et al developed a model to evaluate the effect of the most important factors on the MARD statistical properties. The results indicated the necessity for establishing new guidelines on clinical studies for the assessment of CGM performance. 37 This conclusion was confirmed by another study that used clinical trial data, Monte Carlo simulations, and a mathematical model to determine the confidence region of MARD as a function of the number and the accuracy of the reference measurements. The authors propose a newly introduced MARD reliability index (MRI), which quantifies the uncertainty of the computed MARD values and independently mirrors the reliability of the evaluation. 27
Developmental Models
In addition to the investigation of metabolic processes, models and simulations are often used to assess the clinical or economic outcome of diabetes treatment. A variety of
models analyzing the risk of diabetes and its complications have been described. 46 The next paragraph shortly summarizes important features of modeling and highlights selected developmental models and simulations (Tables 1 and 2).
Models and Simulations for Diabetes Progression
There are different combinations of models available to simulate the progression of diabetes during the course of the disease in patients. Examples of modeling techniques are presented here.
Decision trees, in which every potential alternative and the joined consequences are selected for the moment, have a limited and fixed time horizon. For the developmental modeling of diabetes, in which parameters change over time (with age, health status, and time), decision trees are seldom used due to the inflexible characteristics of the model. More complex state-transition models like Markov chains are more suitable for the development of diabetes over time as it is possible to change/adapt parameters.
For progression models the likelihood of the transition from one health status into another can be estimated for an individual patients or a patient cohort at a defined time interval. A limitation of Markov chains is that the probability distributions at the parameter level are ignored. To simulate outcomes discrete-time micro-simulations are often chosen as the predicted events can be arranged along a time axis with a strict order. For uncertainty analysis Monte Carlo simulations are used where the simulation chooses random values from the probability distribution and applies them as variables into the algorithms of the model. For diabetes progression, a combination of Markov models and Monte Carlo simulations are often used to analyze a problem in more detail.47,48
Examples of Models Investigating Risk Estimations, Cost Outcomes or the Prevention of Diabetes
One frequently used risk engine that provides a risk equation of new coronary heart disease (CHD) events in patients with type 2 diabetes mellitus (T2DM) is based on data from one important outcome study, the United Kingdom Prospective Diabetes Study (UKPDS). This risk engine incorporates glycemia, systolic blood pressure, and lipid levels as risk factors, in addition to age, sex, ethnic group, smoking status, and time since diagnosis of diabetes. The parametric model allows estimation of event rates and survival probabilities in a variety of applications, such as resource use estimation for health planners, power calculations for clinical trials and estimation of effectiveness and cost-effectiveness in early stages of drug development cycles. 28
The mathematical model “Archimedes” was initially designed for simulating health care systems and then extended to replicate the pathophysiology of diabetes at a high level of biological and clinical detail. The aim of the model was to provide a trial-validated method that can be used to address questions that cannot feasibly be addressed through empirical or clinical studies. The model is continuous in time, represents biological variables continuously and can be applied and used for patients with T1DM or T2DM. It has been validated for a variety of clinical trials and reproduced their results with good accuracy.10,29
In 2003 Lindström and Tuomilehto developed the Diabetes Risk Score to provide a simple, practical and informative scoring system to characterize individuals according to their future risk of T2DM. They collected data from a random population of individuals without prior antidiabetic drug treatment with a follow-up of 10 years and used a multivariate logistic regression model coefficient to assign each investigated variable category a score. These scores were summarized into the Diabetes Risk Score which could reliably identify individuals at high risk for developing T2DM. 31
More recent simulation models, such as for example MICADO, aimed to evaluate long-term cost-effectiveness of interventions in both patients with diabetes and the general population. For this purpose the RIVM Chronic Disease Model was modified and extended with modules for microvascular complications in subjects with T1DM or T2DM. The resulting MICADO model is a Markov-type, multistate transition model linking risk factors to incidence of diabetes and micro- and macrovascular complications and can be used to describe the natural course of diabetes and its complications. 12
The approach of Llauradó and colleagues provides the first risk estimation model for predicting silent myocardial ischemia (SMI) in individuals with T1DM. The model combines only two clinical variables: active smoking and insulin-resistance. The evaluation of the model showed that it correctly classified more than 80% of patients with T1DM with SMI. It also significantly enhanced the capacity to detect such subjects compared with current risk estimation models as the UKPDS Risk Engine or the equation derived from the Pittsburgh Epidemiology of Diabetes Complications Study.28,49 The model has the potential to improve coronary artery disease (CAD) care in patients with T1DM through a strategy focused on accurate, cost-effective detection of SMI. 32
PRIME is a model capable of predicting long-term clinical and cost outcomes in patients with T1DM based on long-term follow-ups from landmark trials and diabetes registries. It runs as a patient-level simulation, making use of covariance matrices for cohort generation and risk factor progression. Validation analyses comparing modeled outcomes with published studies demonstrated that PRIME projects long-term patient outcomes consistent with those reported for a number of long-term studies. Macrovascular end points were reliably reproduced across five different populations and microvascular complication risk was accurately predicted. The model aims at influencing decisions toward improved diabetes management and/or prevention. 11
Fortwaengler and colleagues modeled risk and cost estimation of insulin-treated patients with diabetes by assessing the association of complications with HbA1c changes, the incidence of complications and the average cost per event of the complications associated with HbA1c changes. 50 Based on this, they combined their modeling approach with data provided by the UVA/Padova type 1 diabetes simulator to investigate the influence of SMBG system accuracy on clinical outcomes and their financial impact. They could show an increase in costs associated with less accurate SMBG systems as a result of an increased incidence of complications. 51
Opportunities of In Silico Modeling
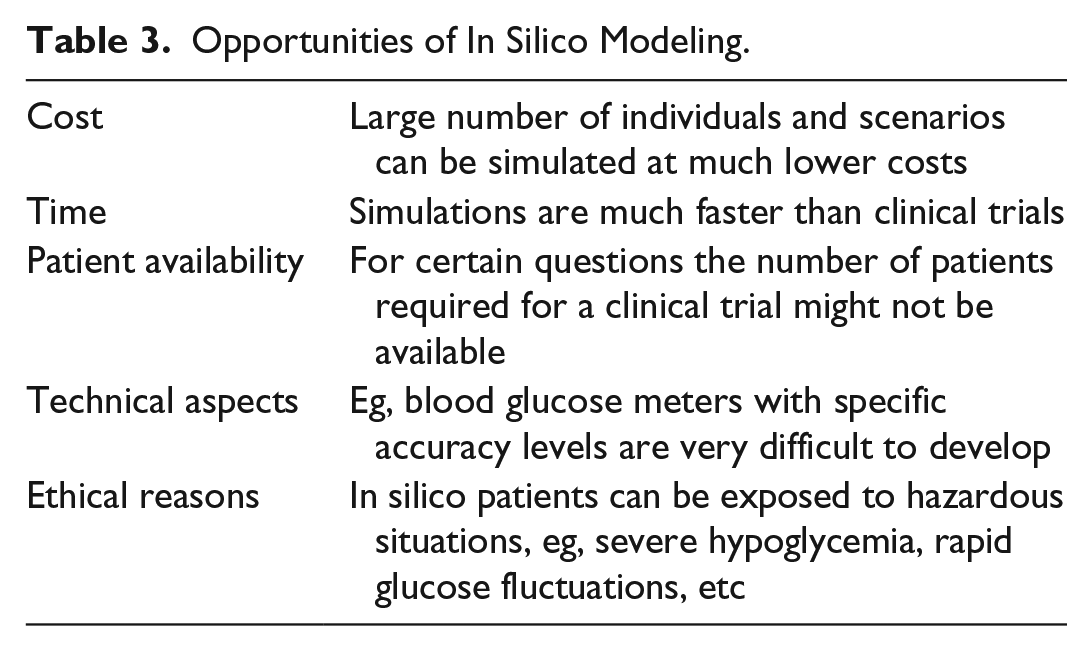
In silico studies offer a large number of opportunities to investigate questions and relations, which are difficult to answer and unravel completely in vivo or in clinical trials (summarized in Table 3). Patients with diabetes highly depend on effective treatment options and reliability of diagnostics devices for their diabetes management. The understanding of metabolic processes can open the route for new treatment options and enables complex regulated systems like AP systems.7,8,17 High accuracy of BG meters/CGM systems is rightly a precondition for the approval of new devices.52-54 A simulation model for diabetes is able to simulate both micro- and macrovascular complications and every other possible outcome (eg, quality of life, life expectancy, etc) that is unlikely to test completely in clinical trials. Thus, simulations are much less expensive and extensive. In a simulation, long time intervals (years instead of months) can be modeled, nonetheless being much faster than clinical trials and helping patients in earlier health states. In addition, results obtained from clinical trials are always only directly applicable to the study population and set-up which they are derived from the ADA. 16 Another opportunity is the high rate of parameter changes in diabetic models that can be readjusted in comparison to clinical studies, where readjustments are not possible. A further advantage of in silico simulations is the ability to include patients, which normally would not be integrated in clinical studies (eg, pregnant women). Here, in silico estimates could avoid dangerous interventions. 55 Therefore, simulations can help decision makers to highlight every possibility or outcome and find the right treatment for the individual patients. Last but not least, models have already confirmed the results of clinical studies proving their effectiveness (eg, McEwan et al, 9 Eddy and Schlessinger, 10 Valentine et al, 11 Heijden et al, 12 ADA, 13 Palmer et al 14 ).
Opportunities of In Silico Modeling.
Challenges of In Silico Modeling
Using computer modeling, different challenges may occur. The models have to be regularly updated and validated to ensure accurate predictions, especially if involved in diabetes treatment or management. The validation of the models is a challenge, as there is for example only a limited number of clinical data to provide a variety of options (eg, UKPDS, Diabetes Control and Complications Trial [DCCT], and Wisconsin Epidemiologic Study of Diabetic Retinopathy [WESDR]).56-59 Thus, many simulation models are validated against the same data sets. This challenge also extends into the design of developmental models, as they are often based on the same cohort real-world data, resulting in a limited representation of certain patient groups. In addition, some of those clinical data are simply outdated. The risk to develop diabetes and its complications has drastically decreased since publication of most of these landmark studies. Furthermore, accuracy of models is a big issue, especially if treatment or management of patients with diabetes relies on simulated outcomes. 17 Comparing the results of two or more different models can be complicated due to the great variety of models, algorithms, patient cohorts, and parameters available. Models using Monte Carlo simulations increase the difficulty of comparability as there is no empirically based recommendation for the required number of replications to ensure accurate results. 60 As every model has its limitations, these could lead to extended simulation times (up to weeks), limited data availability, limited representation for other cohorts, underestimation of costs, or false outcomes (under-/overestimation of complications; eg, Heijden et al, 12 Hoerger et al, 61 Clarke et al, 62 Hoerger et al, 63 McQueen et al, 64 Barhak, 65 Willis et al, 66 Breeze et al, 67 Gillies et al 68 ). One should be aware that simulation models currently cannot replace in vivo clinical studies. Therefore, in silico studies should be seen as a support for decision makers, but not as an exclusive basis for new guideline for the proper intervention.
Summary of the Clinical Impact of Diabetes Modeling
Simulation of either metabolic processes or disease and economic outcomes have a high clinical relevance for the treatment and management of diabetes. The UVa/Padova T1DMS is the best example to illustrate this relevance: the simulation model provided insight into the dynamics of the glucose-insulin metabolism thereby supporting the development of AP systems. 17 It was also used to provide evidence on safety and effectiveness of nonadjunctive CGM use to support the approval of a CGM sensor by the FDA.69,70 Similarly, the modeling of the accuracy of CGM systems is required for a reliable management of diabetes and can improve a patients overall health and quality of life (eg, Kovatchev et al, 26 Kropff et al 71 ). This improvement, measured by glucose values, reductions in hypoglycemic events, and so forth, can result in an improved long-term outcome—it might reduce the incidence of diabetes related complications. This in turn could improve economic outcomes, as treatment of complications is often associated with higher costs than the treatment of diabetes itself. Developmental models on the other hand have a more indirect clinical impact. Decision makers might require cost outcomes when evaluating new medications/guidelines in addition to medical outcomes. They might have the need for a direct comparison of cost and medical efficacy of different treatment options, which can be provided by appropriate models. Risk estimations can give insights into treatment or management options. A risk score, as provided by several models, can help identify high-risk patients and intervene at an early stage of disease. Thus, both metabolic and measurement as well as developmental models have a high clinical impact on the treatment and management of diabetes.
Conclusion
The trend to use in silico studies in chronic diseases like diabetes is quite positive as it allows extracting better conclusions from clinical studies and answering multiple questions concerning, for example, intervention methods, treatment costs, and consequences of imprecise medical devices or incorrect measurements, chances for severe outcomes, life expectancy, or quality of life. In silico studies cannot replace clinical studies; however, a combination of in silico and clinical studies is recommended to get as much insight into a given topic as possible. In the future, in silico simulations can also be used as a prerun for clinical studies to get a first estimate of feasibility and thus save huge amounts of budgets that can be used for life-saving interventions. Taken together, modeling of glucose metabolism and diabetes outcomes is an attractive opinion to estimate long-term effects and costs of medication, but every decision maker should carefully observe the results and their consequences.
Footnotes
Acknowledgements
The authors thank Luigi del Re for critical reading and discussion of the manuscript.
Abbreviations
4-S, Scandinavian Simvastatin Survival Study; ADA, American Diabetes Association; AP, artificial pancreas; BG, blood glucose; CAD, coronary artery disease; CARE, cholesterol and recurrent events; CGM, continuous glucose monitoring; CHD, coronary heart disease; CSII, continuous subcutaneous insulin infusion; DCCT, Diabetes Control and Complications Trial; FDA, Food and Drug Administration; HOPE, Health Outcomes Prevention Evaluation; IDNT, Irbesartan Diabetic Nephropathy Trial; IDT, Institute of Diabetes Technology; IRMA, Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria; MARD, mean absolute relative difference; MICADO, modeling integrated care for diabetes based on observational data; MRI, MARD reliability index; PK, pharmacokinetic; POC, point of care; QOL, quality of life; SMBG, self-monitoring of blood glucose; SMI, silent myocardial ischemia; T1DM, type 1 diabetes mellitus; T1DMS, Type 1 Diabetes Metabolic Simulator; T2DM, type 2 diabetes mellitus; UKPDS, United Kingdom Prospective Diabetes Study; WESDR, Wisconsin Epidemiologic Study of Diabetic Retinopathy
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: An unrestricted educational grant of Roche Diabetes Care GmbH (Mannheim, Germany) was provided to support the editorial needs of this publication. Roche Diabetes Care GmbH is not responsible for content.