
Abstract

Keywords
A growing number of evidence from observational studies and prospective randomized clinical trials in patients with and without diabetes as well as in critically ill and non–critically ill patients have shown an association between stress hyperglycemia and clinical outcomes.1,2 However, it is unclear whether stress hyperglycemia is the causal course of the poor outcome or if hyperglycemia is a marker of illness severity. 3 Increasing evidence indicates an amplified risk of complications and mortality in patients without a history of diabetes compared to patients with known diagnosis of diabetes in relation to stress hyperglycemia. 4 The aim of this study was to investigate hyperglycemia as a predictor for mortality and length of intensive care unit (ICU) stay in groups of patients with and without known diabetes.
The present study examines data from 200 859 patients included in eICU Collaborative Research Database, a large multicenter critical care database. 5 Data are obtained from several critical care units throughout United States, and cover patients who were admitted in 2014 and 2015. Data were stored and retrieved electronically using the Philips (Amsterdam, Netherlands) eICU program (Telehealth for the ICU). Data were anonymized before published for research analysis. Documentation on the database is available from www.eicu-crd.mit.edu.
In total, 164 290 had registered data on diabetes status; 34 247 patients without diabetes and 27 458 patients with diabetes had at least one episode of observed hyperglycemia defined as a blood glucose measurement above 180 mg/dL. The characteristics of each group is presented in Table 1.
Characteristics of ICU Patients Without Diabetes and With Diabetes, and Observed Hyperglycemia and No Observed Hyperglycemia.
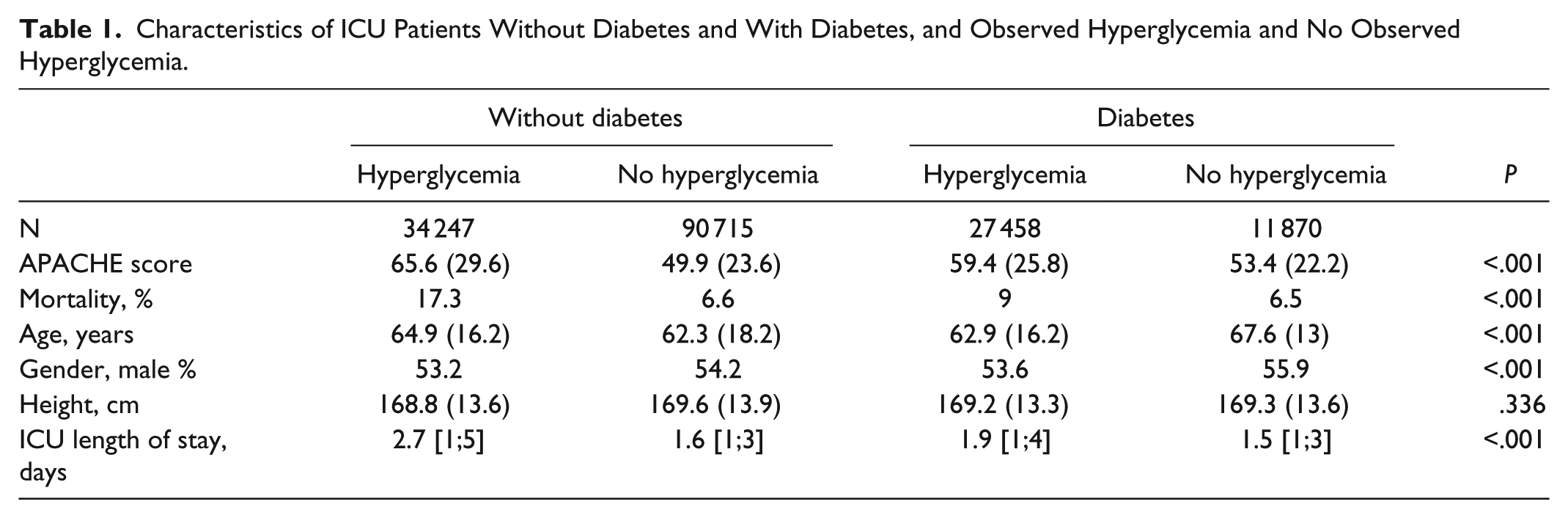
The calculated Acute Physiology and Chronic Health Evaluation (APACHE) score was higher among both groups where hyperglycemia was registered compared to the groups where no hyperglycemia was registered.
The mortality rate among ICU patients without diabetes was 17.3% for observed hyperglycemia and 6.6% for patients without hyperglycemia (P < .001). Length of ICU stay had a median of 2.7 days (hyperglycemia) and 1.6 (no hyperglycemia) (P < .001).
The mortality rate among ICU patients with diabetes was 9% for observed hyperglycemia and 6.5% for patients without hyperglycemia (P < .001). Length of ICU stay had a median of 1.9 days (hyperglycemia) and 1.5 (no hyperglycemia) (P < .001).
The results show that hyperglycemia among ICU patients without diabetes is strongly associated with adverse event. In comparison, hyperglycemia is not as strong among patients with diabetes. Both the mortality and length of ICU stay are increased among patient with diabetes and observed hyperglycemia, but the impact is smaller than observed among patients without diabetes. These results remained significant after adjusting for age and APACHE score using a logistic prediction model (P < .001).
One explanation could be that stress-induced hyperglycemia is a marker for severity of acute illness and that hyperglycemia caused by diabetes is not an equivalent marker. Another reason could be that the surveillance of glucose is more frequent when it comes to patients with diabetes, which may lead to identifying a higher prevalence of hyperglycemia without underlying deterioration of disease.
In conclusion, hyperglycemia is prevalent in ICU patients and in patients without diabetes are strongly associated with adverse outcome.
Footnotes
Abbreviations
APACHE, Acute Physiology and Chronic Health Evaluation; ICU, intensive care unit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.