
Abstract
The necessity of strict glycemic control is unquestionable. However, hypoglycemia remains a major limiting factor in achieving satisfactory glucose control, and evidence is mounting to show that hypoglycemia is not benign. Over the past decade, evidence has consistently shown that real-time continuous glucose monitoring improves glycemic control in terms of lowering glycated hemoglobin levels. However, real-time continuous glucose monitoring has not met the expectations of the diabetes community with regard to hypoglycemia prevention. The earlier trials did not demonstrate any effect on either mild or severe hypoglycemia and the effect of real-time continuous glucose monitoring on nocturnal hypoglycemia was often not reported. However, trials specifically designed to reduce hypoglycemia in patients with a high hypoglycemia risk have demonstrated a reduction in hypoglycemia, suggesting that real-time continuous glucose monitoring can prevent hypoglycemia when it is specifically used for that purpose. Moreover, the newest generation of diabetes technology currently available commercially, namely sensor-augmented pump therapy with a (predictive) low glucose suspend feature, has provided more convincing evidence for hypoglycemia prevention. This article provides an overview of the hypoglycemia outcomes of randomized controlled trials that investigate the effect of real-time continuous glucose monitoring alone or sensor-augmented pump therapy with a (predictive) low glucose suspend feature. Furthermore, several possible explanations are provided why trials have not shown a reduction in severe hypoglycemia. In addition, existing evidence is presented of real-time continuous glucose monitoring in patients with impaired awareness of hypoglycemia who have the highest risk of severe hypoglycemia.
Keywords
The benefits of intensive glycemic control in reducing the microvascular and macrovascular complications of diabetes are well established.1,2 Although strict glycemic control has been associated with an increased risk of hypoglycemia, 1 more recent observational data do not confirm this association.3,4 However, in daily practice, hypoglycemia remains the main side effect of insulin therapy and barrier to achieving glycemic targets. 5
The categorization of hypoglycemic episodes is a matter of continuous debate. 6 Mild hypoglycemia is usually defined as an episode in which a person is able to recognize and self-treat a low level of blood glucose. Severe hypoglycemia is often defined as a hypoglycemic event requiring assistance of a third party. 7 The American Diabetes Association proposed a biochemical definition of hypoglycemia as a plasma glucose of ≤70 mg/dl (3.9 mmol/L). However, many trials use different (biochemical) definitions of hypoglycemia, which makes their comparison difficult. In type 1 diabetes, the mean incidence of mild hypoglycemia is 1-2 events per patient per week and the incidence of severe hypoglycemia is approximately 0.1-1.5 events per patient year.4,8,9
Hypoglycemia is not benign, but has important physical and psychosocial consequences.10,11 Hypoglycemia interferes with many aspects of daily life, including sleep, driving, exercise, social functioning and employment. 11 In people with type 2 diabetes with significant cardiovascular risk, hypoglycemia probably increases the risk of cardiovascular events,12-14 although causality remains difficult to prove. 15 Furthermore, hypoglycemia impairs cerebral function and might promote permanent cognitive decline.16,17 Recurrent hypoglycemia induces defective glucose counterregulation and impaired awareness of hypoglycemia (IAH).18,19 IAH is associated with a 3- to 6-fold increased risk of severe hypoglycemia which considerably impairs their quality of life.20,21 Hypoglycemia can also have a profound effect on psychosocial well-being and causes fear of hypoglycemia.22-24 Health care costs are substantially increased because of hypoglycemia. 25 Importantly, hypoglycemia can be fatal, with mortality estimates ranging from 4% to 10% of deaths in T1DM patients diagnosed in childhood or early adulthood and dying before the age of 40 years.26,27 A recent registry-based observational study showed that in T1DM patients younger than 30 years, 31.4% of deaths was caused by diabetic ketoacidosis or hypoglycemia. 28 Therefore, new treatment and monitoring strategies to prevent hypoglycemia are a necessity.
Although the technique of continuous glucose monitoring became available during the late 1990s, it was not until 2006 that real-time continuous glucose monitoring (CGM) was introduced to assist patients in their self-management. 29 Present CGM systems that are available use small minimally invasive sensors which measure interstitial glucose levels via the glucose-oxidase reaction and translate this into blood glucose values by means of calibrations.30,31 The CGM systems provide this information every 5 or 10 minutes, with a delay of approximately 5 to 15 minutes. The added value lies in the semicontinuous display of “current” glucose values, visualization of glucose trends and the availability alarms that can be set to warn for impending hypoglycemia or hyperglycemia. 32 First generation CGM systems were used as stand-alone devices. Next generation CGM systems are connected to insulin pumps (sensor-augmented pump therapy; SAPT), but do not interfere with insulin delivery automatically. These CGM systems therefore only act as behavior modifiers, rather than insulin dose adjustment tools. The newest generation SAPT systems however have a (predicted) low glucose suspend (LGS) feature, which automatically interrupts insulin administration when glucose falls below a preset threshold.33,34 This steady improvement and development of CGM systems over the last 15 years is welcome, although to some extent it has frustrated evaluation of the clinical evidence. In some trials the benefit of CGM itself was studied, while other trials evaluated the combined effect of CGM and insulin pumps (sometimes with a built-in bolus calculator or automated insulin suspension).
CGM enabled the development of new (CGM-derived) measures to assess glycemic control (ie, time in target, area under the curve and different variability measures).35,36 Most CGM trials used time below target to assess effect of CGM on hypoglycemia. Although time below target is a simple and easy to understand measure, formal evidence demonstrating the usefulness of assessing time below target compared to other measures (ie, frequency of hypoglycemic events), in evaluating clinical benefit of CGM, is lacking. In this narrative review we have provided an overview of the CGM trials and mainly focus on the hypoglycemia outcomes. SAPT with (predictive) LGS will be discussed separately. Also, we discuss trials that were performed in patients with IAH. 20 Relevant articles were identified by searching the PubMed database using the following search terms: “continuous glucose monitoring,” “sensor-augmented pump therapy,” “low glucose insulin suspension,” “predictive low glucose suspension,” “automated insulin pump suspension,” “threshold insulin pump interruption,” “diabetes mellitus,” and “type 1 diabetes.” In addition, references of selected articles were searched for additional relevant articles. The closed-loop systems are beyond the scope of this review, but are reviewed elsewhere. 37
Real-Time Continuous Glucose Monitoring
Mild Hypoglycemia
Most randomized controlled trials (RCTs) investigating the effect of CGM on glycemia primarily aimed at lowering HbA1c, rather than on preventing hypoglycemia. These trials often included patients with suboptimally controlled diabetes and evaluated HbA1c as primary endpoint.38-48 The 2008 JDRF trial was the first landmark RCT investigating the efficacy and safety of CGM. 38 In total, 322 children, adolescents and adults with T1DM using insulin pumps or multiple daily injections (MDI) were randomized to receive CGM or to continue self-monitoring of blood glucose by finger prick (SMBG) for 26 weeks. The study demonstrated a significant reduction in HbA1c of 0,5% in adult participants. However, no significant effect was found on time spent in hypoglycemia. In addition, other trials comparing conventional CGM with SMBG and focusing on HbA1c reduction either did not report on mild hypoglycemia or did not demonstrate any effect on mild hypoglycemia.39-41
Two RCTs compared SAPT with MDI and SMBG.42,43 In the STAR-3 trial, 485 T1DM patients used SAPT or continued using MDI and SMBG for 1 year. 42 Patients who experienced 2 severe hypoglycemic events or more in the year prior to enrollment were excluded. HbA1c improved significantly more in the SAPT group, with a between group difference of 0.6% (P < .001). However, the STAR-3 trial demonstrated no difference in mild hypoglycemia. These findings were supported and extended by the EURYTHMICS trial, which evaluated 83 patients for 6 months and found an impressive HbA1c reduction in the SAPT group (–1.2%, P < .001), but again no significant reduction was observed in time spent in hypoglycemia or the number of mild hypoglycemic events. 43
Several RCTs investigated the incremental effect of CGM when using an insulin pump.44-48 Overall, these studies either did not find a significant44,45 or relevant 46 reduction in mild hypoglycemia or did not report on the occurrence of mild hypoglycemic episodes. 47 However, the SWITCH Study Group did find a significant effect of adding CGM to insulin pump therapy on time spent in hypoglycemia. 48 This cross-over trial randomized 153 children and adults with T1DM using CSII to a Sensor On or Sensor Off arm for 6 months. After a washout of 4 months, participants switched to the other arm. During CGM use, less time was spent in hypoglycemia, with 19 min/day <70 mg/dl (3.9 mmol/L) in the Sensor On arm and 31 min/day <70 mg/dl (3.9 mmol/L) in the Sensor Off arm (P = .009). In addition, the average daily AUC <70 mg/dl (3.9 mmol/L) was significantly lower in the Sensor On arm group. Notably, this cross-over trial gathered 8 weeks of blinded CGM values. Other trials often used less than 14 days of blinded CGM data to analyze CGM-derived outcomes, such as time spent in hypoglycemia or mild hypoglycemia event rate.38,42,43 It is possible that this relatively small amount of blinded CGM data lacked power to demonstrate between group differences.
Few RCTs evaluating the efficacy of CGM primarily aimed at hypoglycemia prevention.49,50 Interestingly, these studies did demonstrate a significant reduction in mild hypoglycemia. The 2009 JDRF trial examined the effect of CGM versus SMBG in 129 adults and children with T1DM and a HbA1c <7.0%. 49 Time spent in hypoglycemia decreased significantly in the CGM group from 91 min/day ≤70 mg/dl (3.9 mmol/L) at baseline to 54 min/day ≤70 mg/dl (3.9 mmol/L) at 26 weeks (P = .002). Marginally nonsignificant, the mild hypoglycemic event rate was less pronounced in the CGM group, with 0.25 events/day versus 0.47 events/day in the control group (P = .07). Moreover, in 2011, Battelino et al assessed the impact of RT-CGM versus SMBG specifically on hypoglycemia in 120 children and adults with T1DM and a HbA1c <7.5%. 50 The authors reported less time spent in hypoglycemia in the CGM group compared with the control group (0.91 hours/day <70 mg/dl [3.9 mmol/L] vs 1.6 hours/day <70 mg/dl [3.9 mmol/L], respectively; P = .01). Furthermore, the number of mild hypoglycemic events per day was lower in the CGM group (0.53 events/day in the CGM group vs 0.76 events/day in the control group, P = .08).
Nocturnal Hypoglycemia
Nocturnal hypoglycemia is of major concern to people with T1DM. Studies using CGM report a prevalence of nocturnal hypoglycemia of up to 68%.51-53 In the DCCT, half of the severe hypoglycemic events occurred during sleep. 54 In addition, in children, up to 75% of hypoglycemic events associated with seizures or coma occur at night when counterregulatory responses are impaired.54-56 Furthermore, the “dead-in-bed” syndrome accounts for approximately 6% of all deaths in people with T1DM under the age of 40 years, which is probably related to severe nocturnal hypoglycemia. 57
CGM studies reporting on nocturnal hypoglycemia should be interpreted with caution due to concerns around the accuracy of glucose sensors at night (ie, due to compression artifacts, disconnections and lack of calibrations at night).58-60
The impact of CGM on nocturnal hypoglycemia has seldom been reported.29,50 In a study by Garg et al, nocturnal hypoglycemia (<55 mg/dl [3.1 mmol/L]) was reduced by 38% in the display on group compared with the control group (P < .001). 29 In addition, the trial of Battelino et al reported significantly lower hypoglycemic excursions during the night in the CGM group compared with control (0.13 vs 0.19 excursions/night <55 mg/dl [3.1 mmol/L], P = .01 and 0.21 vs 0.30 excursions/night <63 mg/dl [3.5 mmol/L], P = .009). 50 Other trials investigating the efficacy of CGM either did not evaluate the effect on nocturnal hypoglycemia, or did not report it. Future studies evaluating the effect of CGM on hypoglycemia should report nocturnal hypoglycemia.
Severe Hypoglycemia
CGM was expected to reduce severe hypoglycemia. 61 Unfortunately, evidence supporting this belief is still lacking. No RCTs investigating CGM showed a significant decrease in severe hypoglycemia (Table 1). One of the earliest trials even reported a significant increase of severe hypoglycemia in the CGM group. 46
Overview of CGM Randomized Controlled Trials in Type 1 Diabetes.
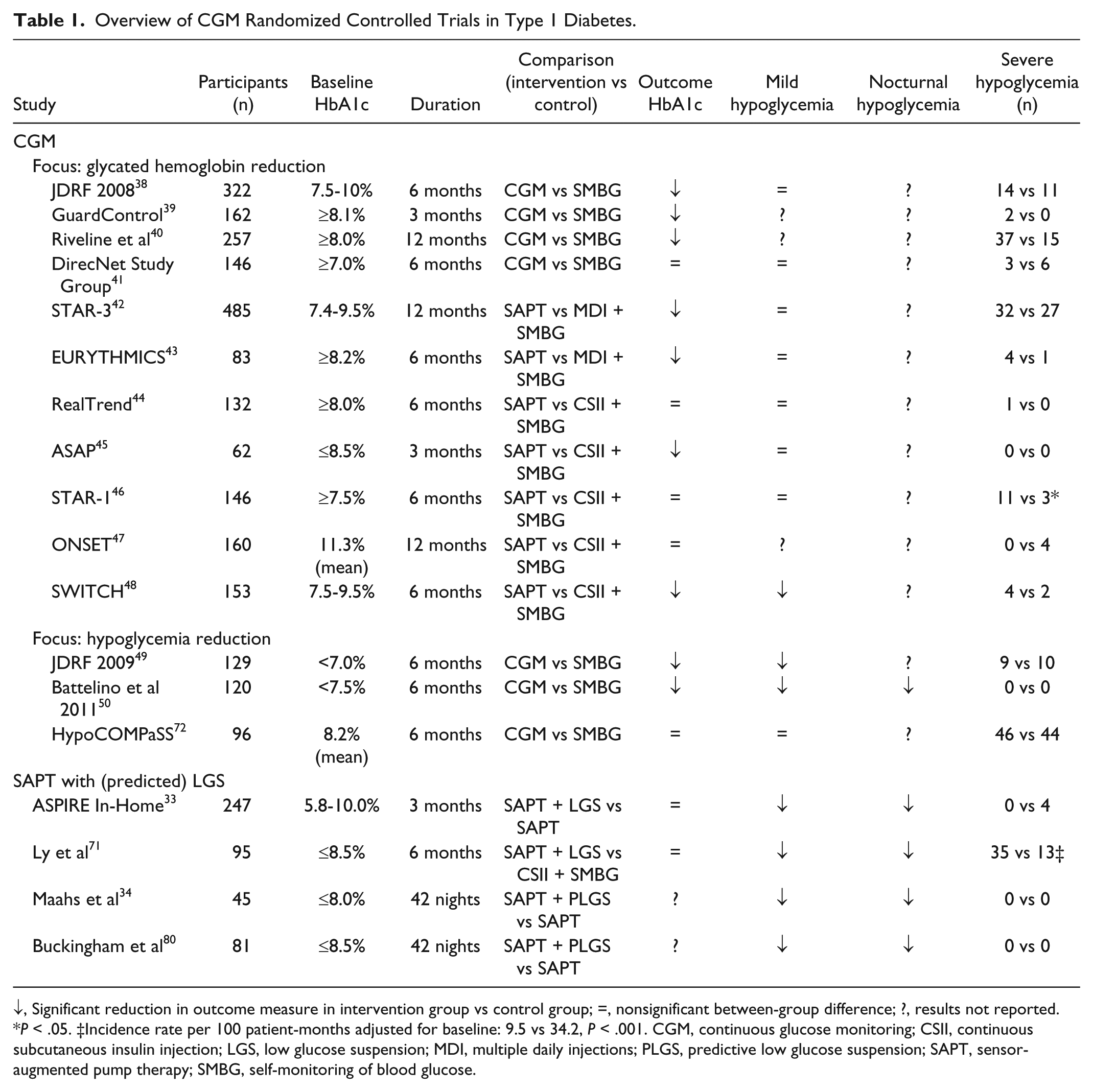
↓, Significant reduction in outcome measure in intervention group vs control group; =, nonsignificant between-group difference; ?, results not reported. *P < .05. ‡Incidence rate per 100 patient-months adjusted for baseline: 9.5 vs 34.2, P < .001. CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin injection; LGS, low glucose suspension; MDI, multiple daily injections; PLGS, predictive low glucose suspension; SAPT, sensor-augmented pump therapy; SMBG, self-monitoring of blood glucose.
Some meta-analyses are performed comparing severe hypoglycemic event rates during CGM versus SMBG.62,63 In 2011, Pickup et al performed an individual patient level meta-analysis. 62 The overall severe hypoglycemia incidence rate ratio on SMBG compared with CGM was 1.40 (0.87-2.25, P = .17). These findings were supported by the Cochrane Collaboration in 2012, which also found no difference in incidence rates of severe hypoglycemia between CGM and SMBG (risk ratio 1.05 (0.63-1.77). 63
Several explanations have been put forward to explain why CGM does not seem to prevent severe hypoglycemia, or, why trials are unable to demonstrate this. Importantly, none of the trials had sufficient power to demonstrate a difference in severe hypoglycemia. Moreover, most trials were designed to lower HbA1c instead of preventing (severe) hypoglycemia and in some trials, patients with recent severe hypoglycemia or IAH were excluded.42,45,48 In these trials, patients and study staff may have been less focused on preventing hypoglycemia. Since CGM devices act only as behavior modifiers, the focus of patient and caregiver to reduce hypoglycemia is of major importance to perceive this goal. Furthermore, although the accuracy of CGM systems have steadily improved over the last decade,64,65 the performance of CGM devices is still poorest in the hypoglycemic range, which may hinder its ability to provide an adequate alarm to prevent severe hypoglycemia. Also, qualitative studies show that frequent (inadequate) alarms irritate the user and are a major barrier to the effective use of CGM.66,67 Hypoglycemia-induced cognitive decline and sleep may cause inadequate responses to alarms.68,69
Impaired Awareness of Hypoglycemia
Whether CGM can prevent hypoglycemia in patients with IAH, either directly or by improving hypoglycemia awareness, has yet to be established. In 2011, a hyperinsulinemic hypoglycemic clamp study by Ly et al showed that 4 weeks of CGM improved epinephrine responses in young T1DM patients with IAH, suggesting that IAH can be restored in adolescents by using CGM. 70 This finding was not supported by a larger trial performed by the same study group. 71 In 2014, Little et al evaluated in the HypoCOMPaSS trial whether hypoglycemia awareness can be improved and severe hypoglycemia can be prevented by using strategies available in routine practice, including CGM. 72 This RCT had a 24-week 2 × 2 factorial design, comparing CSII with MDI and CGM with SMBG. All participants received written insulin titration guidelines, educational sessions, weekly telephone consultations and monthly visits to achieve rigorous avoidance of biochemical hypoglycemia. After 24 weeks, hypoglycemia awareness scores measured according to the method of Gold et al 21 (scale of 1 to 7) had improved from 5.1 to 4.1 (P = .0001), without between-group differences. The clinical relevance of this improvement in hypoglycemia awareness is unknown. Although the improvement in hypoglycemia awareness scores was accompanied by a significant reduction in severe hypoglycemia, from 8.9 events per patient-year at baseline to 0.8 events per patient-year after 24 weeks, this reduction in severe hypoglycemia was probably caused by the insulin adjustment algorithm, education, frequent telephone consultations and consultations rather than the improvement in hypoglycemia awareness. The authors did not demonstrate any difference in severe hypoglycemia or time spent in hypoglycemia between CGM and SMBG, which is also most likely explained by a floor effect, with maximal reduction already attained by this intensive guidance. Whether such intensive guidance is feasible in routine clinical practice is under debate.73,74
The first observational study performed in patients with IAH demonstrated a clear reduction of SH with CGM use, without change in hypoglycemia awareness scores, 75 addressing the need for further interventional studies in patients with IAH. An RCT investigating the effects of CGM in these patients is currently being conducted. 76
Sensor-Augmented Pump Therapy With (Predictive) Low Glucose Suspension
Mild and Nocturnal Hypoglycemia
Several feasibility studies evaluating the LGS feature have demonstrated less time spent in hypoglycemia and fewer hypoglycemic episodes, 77 less nocturnal hypoglycemia in those at greatest risk, 78 and shorter duration of hypoglycemic episodes 79 without an increased risk of ketoacidosis or hyperglycemia.
In 2013, the ASPIRE In-Home Study Group evaluated the effect of SAPT with LGS, compared with SAPT alone, on nocturnal hypoglycemia and glycated hemoglobin levels. 33 Patients were eligible if they experienced ≥2 nocturnal hypoglycemic events during the 2-week run-in phase. After 3 months the mean AUC for nocturnal hypoglycemic events was 980 mg/dl × minutes (54.4 mmol/L × minutes) in the LGS group and 1568 mg/dl × minutes (87 mmol/L × minutes) in the control group, a 38% reduction (P < .001). In addition, the frequency of nocturnal hypoglycemic events was significantly reduced by 31.8% in the LGS group (P < .001). The time spent in hypoglycemia was also significantly lower in the LGS group. There were no severe hypoglycemic events in the LGS group and 4 severe hypoglycemic events in the control group.
The In Home Closed Loop Study Group assessed the safety and effectiveness of a predictive LGS feature in a 42-night in-home randomized trial. 34 Each night, the 45 T1DM patients were randomly assigned to having the predictive LGS feature on (intervention) or off (SAPT only, control). The proportion of nights in which ≥1 sensor value ≤60 mg/dl (3.3 mmol/L) occurred was analyzed as primary outcome. At least 1 sensor value ≤60 mg/dl (3.3 mmol/L) occurred during 21% of the intervention nights, compared with 33% of the control nights (P < .001). In addition, the intervention reduced the duration, frequency and AUC of nocturnal hypoglycemia significantly. These findings were accompanied by the results of a similar RCT of the In Home Closed Loop Study Group performed in children with T1DM. 80 In both trials, morning ketosis did not differ between the intervention and control nights. Mean overnight and morning glucose values were slightly higher during and after the intervention nights.
These data suggest that using (predictive) LGS in addition to SAPT is safe and effective in reducing the size (AUC per hypoglycemic event) and the frequency of (nocturnal) hypoglycemic events.
Severe Hypoglycemia
In 2013, Ly et al investigated the effect of SAPT with LGS on the combined frequency of moderate (defined as a hypoglycemic event requiring third party assistance) and severe (defined as a hypoglycemic event resulting in seizure or coma) hypoglycemia in T1DM patients with IAH. 71 At baseline, the combined moderate and severe hypoglycemia rate was significantly higher in the LGS group, with 129.6 events per 100 patient-months, compared with 20.7 events per 100 patient-months in the control group. After 6 months, the incidence rate of combined moderate and severe hypoglycemia, adjusted for baseline rates, was significantly lower in the LGS group compared with the control group (9.5 events per 100 patient-months vs 34.2 events per 100 patient-months, respectively), resulting in an incidence rate ratio of 3.6 in favor of the LGS group (P < .001). In addition, combined daytime and night-time time spent in hypoglycemia was significantly lower in the LGS group. However, when 2 outliers with the highest baseline event rates of moderate hypoglycemia were excluded, the primary outcome lost significance (rate ratio 2.2, P = .08). Furthermore, the German Institute for Quality and Efficiency in Health Care reanalyzed the data from the Ly study, questioned its methodological quality and could not confirm its conclusions. 81 They argued that hypoglycemia rates are problematic as an endpoint, mainly because statistical tests require independent observations and therefore the patient should be the statistical unit, not an event, as hypoglycemia is known to cluster in a subgroup of patients.4,82 Indeed, the number of patients affected by severe hypoglycemia was 3 out of 45 in the control group versus 0 out of 41 in the intervention group and analyzed with the patient as a statistical unit this difference is not significant. 81 Nevertheless, event rates in the way as analyzed by Ly et al are an accepted endpoint in diabetes trials. In addition, by excluding the 2 outliers, Ly et al explored the effect of extreme values on the results and the issue of clustering. Furthermore, it should be pointed out that the authors prespecified their statistical analyses and the journal’s statistical advisor agreed to their appropriateness. Finally, from a clinical point of view, severe hypoglycemia is a clinically relevant outcome. We therefore find the results of this trial promising, since it is the first trial to demonstrate a reduction in severe hypoglycemia by CGM. Future trials attempting to confirm the findings of the Ly study could consider including a sufficient number of patients experiencing severe hypoglycemia, to show a reduction in the proportion of patients affected, instead of demonstrating a reduction of the incidence of severe hypoglycemia only in those with the highest incidence rates.
Conclusion
CGM/SAPT can decrease HbA1c without increasing hypoglycemia. Most trials investigating the effect of CGM in T1DM patients however, do not demonstrate a reduction in (severe) hypoglycemia. But, during these trials patients and investigators were possibly more focused on improving glycemic control by lowering glycated hemoglobin values than on preventing hypoglycemia. Since CGM devices without low glucose suspension only act as behavior modifiers, they can only prevent hypoglycemia through CGM-induced behavioral changes. To incorporate these behavioral changes into the self-management of patients, patients and caregivers must be focused on preventing hypoglycemia. This is strengthened by the fact that the trials focusing on hypoglycemia prevention also show a reduction in mild hypoglycemia, suggesting that CGM is able to prevent hypoglycemia when it is used for that purpose. In our opinion, this behavior factor is often undervalued. Trials investigating the effect of SAPT with LGS more convincingly show its benefit in mild, nocturnal and possibly even severe hypoglycemia prevention. Although self-management will always be an important factor in the management of T1DM, this underscores the need for further replacement of self-management by automated insulin therapy.
Footnotes
Abbreviations
CGM, real-time continuous glucose monitoring, DCCT, Diabetes Control and Complication Trial; IAH, impaired awareness of hypoglycemia; LGS, low glucose suspension; MDI, multiple daily injections; RCT, randomized controlled trial; SAPT, sensor-augmented pump therapy; SMBG, self-monitoring of blood glucose; T1DM, type 1 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JHDV is serving on an advisory board for Roche Diagnostics and has received research support from Abbott, Dexcom, Medtronic, and Senseonics.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.