
Abstract
Background:
Continuous glucose monitoring can improve glycemic outcomes in individuals with type 1 diabetes. However, the constant exposure to real-time glucose levels can sometimes lead the individual to make some risky choices to address the glycemic excursions. Hence, the purpose of this study was to explore the aberrant management behaviors of youth with type 1 diabetes on sensor-augmented pump therapy (SAPT).
Methods:
Participants in a clinical trial using SAPT on Medtronic MiniMed™ 640G pump who experienced deteriorating glycemic control or unexplained hypoglycemia were identified by the health care professional. The pump and/or sensor data uploaded to CareLink™ Therapy Management Software were reviewed in these participants.
Results:
Uncharacteristic management behaviors were identified in five adolescent males. Continuous exposure to high glucose levels resulted in obsessive behaviors displaying a perfectionistic attitude in two participants. Multiple boluses were delivered frequently as uneaten carbohydrates in participant 1 while participant 2 resorted to delivery of extra insulin by cannula fills. In contrast, participant 3 chose to remain hyperglycemic to avoid weight gain while participant 4 trusted the system and used sensor glucose readings for calibrations, with resultant deterioration in glycemic control in both participants. On the other hand, participant 5, due to mistrust in the pump suspend function, consumed carbohydrates with downward glucose trends with rebound hyperglycemia.
Conclusions:
Constant exposure to real-time data can lead to unsafe management responses in adolescents with the behavior influenced by trust or mistrust in the system. Adolescents should be empowered with problem-solving strategies for safe management.
Keywords
Continuous glucose monitoring (CGM) systems have empowered individuals with type 1 diabetes to respond and make adjustments to their diabetes management 1 with improved glycemic control and with reduction in severe hypoglycemia and overall health costs.2 -5 CGM provides real-time glucose readings with trends, alarms and automated insulin suspensions when used in conjunction with insulin pump. The information available to the user enables CGM to be utilized as a powerful tool in the improvement of glycemic control. However, although the CGM user is educated in sensor insertion, calibration, glucose testing and use of alarms, patients and health-care providers are now presented with an avalanche of information and have to determine the best utilization of the data available through CGM. Patients tend to perform fewer self-monitoring of blood glucose (SMBG) while on CGM 6 and also make relatively large insulin adjustments in response to display trends and arrows. 7 However, as yet, there are few uniform recommendations in the effective use of CGM. 8 This lack of knowledge and recommendations can lead at times to erratic and unsafe individual responses to glycemic excursions, especially in adolescence, a period that is prone to heightened engagement in risky and reckless behaviors. 9
Methods
We present a case series of adolescents on sensor-augmented pump therapy (SAPT) who exhibited these behaviors. The aim of this series is to create awareness of such practices in users of SAPT and to further explore the issue of trust and mistrust in medical technologies. Participants with deteriorating glycemic control or unexplained hypoglycemia who exhibited erratic and unexplained behaviors were identified by the diabetes nurse educator and/or the principal investigator of each center conducting the Predictive Low Glucose Management (PLGM) randomized controlled home trial . The trial aimed to determine the efficacy of the “suspend before low” function in real life. 10 During the course of the 6-month trial, all participants were required to wear the Medtronic MiniMed™ 640G pump and Enlite™ glucose sensor with the Guardian™ 2 Link transmitter. The pump was uploaded to CareLink™ Therapy Management Software at each research visit.
The pump and sensor training was delivered by a credentialed diabetes educator. All participants were experienced in the use of an insulin pump, and had knowledge of their carbohydrate ratios and insulin sensitivity. They all received technical training on the use of the pump. All participants were sensor naïve and CGM training was directed toward the participant and parent, depending on the age of the participant. All participants were taught the principles of CGM use, over a 2 hour individual session. The physiological difference between blood glucose and interstitial glucose and the time lag was explained. The education included the importance of regular calibration and calibration timing. All participants were advised to perform a confirmatory meter blood glucose check for diabetes treatment decisions and not base them on sensor glucose values alone. Only the low alerts were mandatory while all other alerts were individualized. No specific education around insulin adjustment with trend arrows and alerts was imparted. However, participants who had the “suspend before low” function turned on were taught the criteria within the algorithm for the pump to initiate a suspension with hypoglycemia prediction, being based on trend, direction, and speed of change. Scenarios were used to help participants understand the purpose of this function within the context of their own diabetes management.
Results
Five adolescent males with (mean ± SD) duration of diabetes of 6.4 ± 3.1 years and HbA1c of 58 mmol/mol (7.5 ± 1.3% ) on insulin pump therapy for 3.8 ± 1.7 years were identified. The erratic behaviors, participant rationale and health care practitioner (HCP) advice are described.
Participant 1
HCP concern
The concern was manual insulin boluses administered frequently.
Background
A 16.1-year-old with diabetes for 7.2 years and on insulin pump therapy for 4.2 years with HbA1c of 40 mmol/mol (5.8%) was commenced on SAPT. He was concerned about hyperglycemia and subsequent weight gain with treatment of multiple hypoglycemic episodes.
Behavior
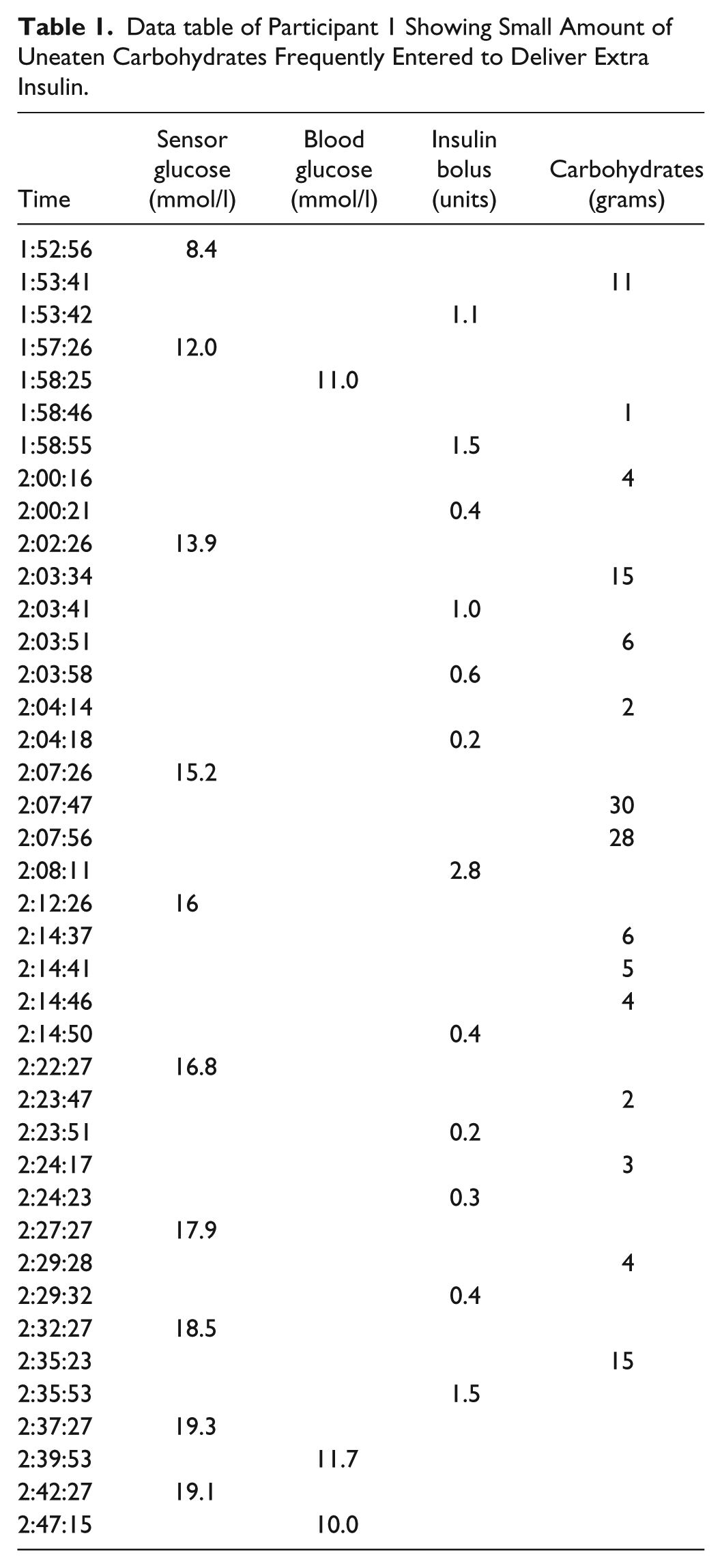
CGM use in the participant caused anxiety and discomfort as he became aware of low and high sensor glucose (SG) levels. He exhibited perfectionistic behavior and was overtly focused on his diabetes management. He acknowledged his discomfort when SG was > 10 mmol/l and resorted to frequent correction boluses by using manual boluses entering uneaten carbohydrates as shown in Table 1. Boluses were administered every one to two minutes with the intention to deliver extra insulin to reach the desired target range sooner as he was concerned of the relatively slow action of insulin. Following review of the CareLink data, the HCP discussed the action of insulin and discouraged insulin stacking and the subsequent potential to recurrent hypoglycemia.
Data table of Participant 1 Showing Small Amount of Uneaten Carbohydrates Frequently Entered to Deliver Extra Insulin.
Participant 2
HCP concern
The concern was excessive amount of insulin used for cannula and tubing fills.
Background
A 14.3-year-old with diabetes for 2.7 years and on pump therapy for 1.9 years had good glycemic control with HbA1c of 48 mmol/mol (6.5%). However, he had impaired hypoglycemia awareness and had experienced four severe hypoglycemic events, and two episodes of unexplained hypoglycemia requiring hospital emergency visits.
Behavior
The CareLink report (Figure 1) demonstrated an excess amount of insulin for cannula and tubing fills (tubing fill of 70.6 units and cannula fill of 1.52 units; the prescribed being 0.3 units for cannula fill). Pump rewind, cannula and tubing fills were done daily with excessive finger prick testing. The participant behavior was driven by expectations, both personal and from parents, to maintain perfect glycemic control. The assumption was that the cannula and tubing fills were used to administer insulin without the behavior identified on bolus history. The findings were addressed at a clinical level with the adolescent and the family.
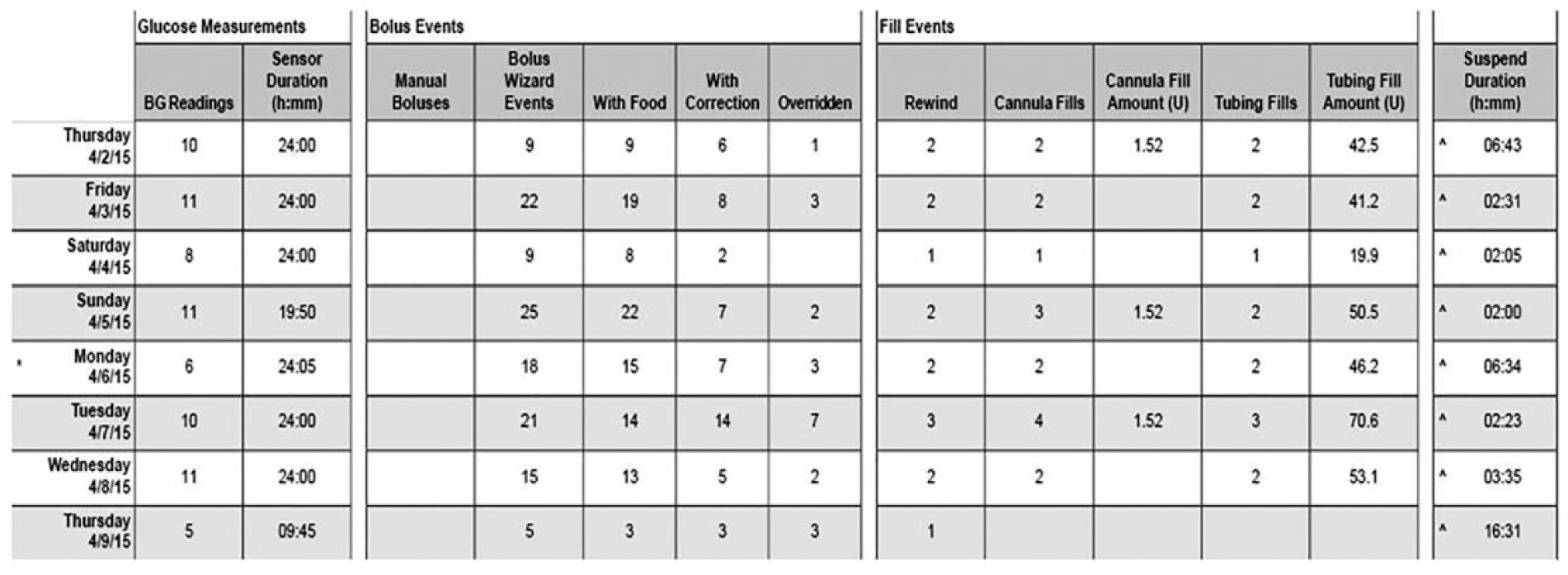
CareLink pro of participant 2 with large amounts of insulin used for cannula and tubing fill.
Participant 3
HCP concern
The concern was insulin boluses administered into disconnected pump during daytime.
Background
A 14.8-year-old adolescent with diabetes for 8 years and on insulin pump for 6 years was dedicated to his athletic pursuits with a desire to remain lean although he was unable to engage in resistance weight-training due to his young age. His glycemic control was suboptimal with HbA1c of 78 mmol/mol (9.3%). He admitted to prolonged periods of interval training. He had also experienced two severe hypoglycemic episodes. Both the participant and parents were keen to use sensors as a safeguard for upcoming sporting events. The participant had also received dietetic input with regard to the amount of carbohydrates required to support his current activity although he was not keen on increasing carbohydrate intake to avoid weight gain.
Behavior
There was a mismatch between SG readings and pump upload with insulin delivery (Figure 2a). The SG levels were persistently elevated across the day although the total daily insulin was 1.24 u/kg with 69% delivered as bolus. The sensor overlay is demonstrated in Figure 2b. The SG profile fell overnight, however; increased and remained elevated across the entire day in spite of multiple insulin doses, with no evidence of expected drop in glucose due to delivered boluses. It was suggested that during daytime, blood glucose, and carbohydrate amounts were entered into the pump while being disconnected. Behavior was speculated to avoid weight gain. The participant however denied disconnecting the pump, although he did acknowledge a concern of remaining continuously attached to the device and attributed the constantly elevated SG levels to set issues.
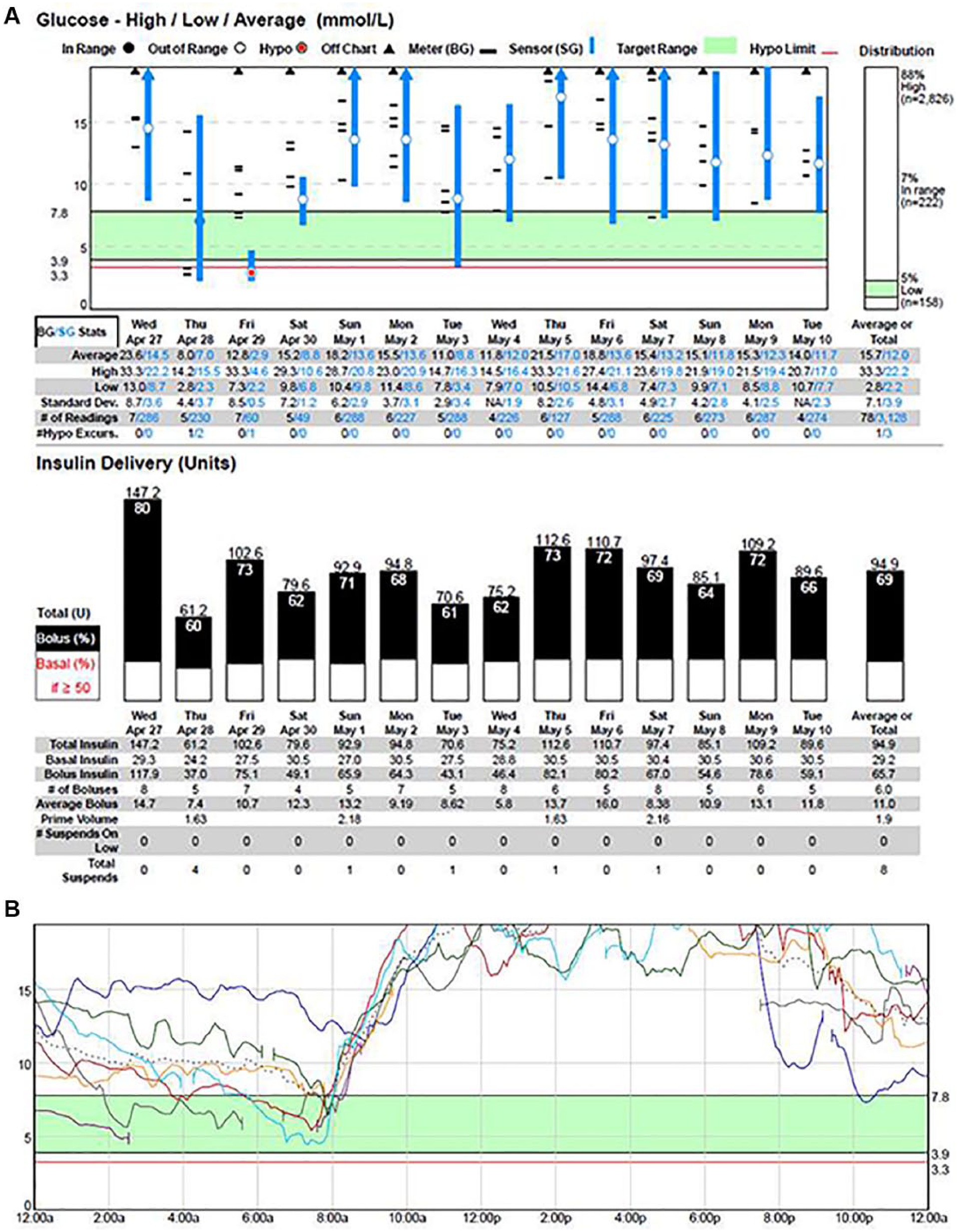
(a) A quick-view summary of participant 3 from CareLink Trial. The sensor glucose is persistently elevated in spite of adequate testing and insulin boluses. (b) Sensor daily overlay for participant 3 with persistently high sensor glucose readings.
Participant 4
HCP concern
The concern was sensor glucose readings used for calibrations and to replace SMBG.
Background
A 15.7-year-old adolescent with diabetes for 4.4 years and on pump therapy for 2.4 years had HbA1c of 51 mmol/mol (6.8%) at recruitment. Suspend before low was activated for the duration of the study.
Behavior
HbA1c increased from 51 mmol/mol (6.8%) at study entry to 67 mmol/mol (8.3%) after four months and 79 mmol/mol (9.4%) after seven months. The sensor daily overlay report was not consistent with poor glycemic control with an average SG of 7.1 ± 2.5 mmol/l as shown in Figure 3a, while Figures 3b and 3c demonstrate the data table. The participant acknowledged the entry of SG readings into the pump for calibration and bolus. The use of SG for calibration and bolus was reportedly seen as an easier way to manage his glucose readings without resorting to the need for finger pricks. The need to perform SMBG to bolus for meals and to calibrate sensor was reiterated by HCP.
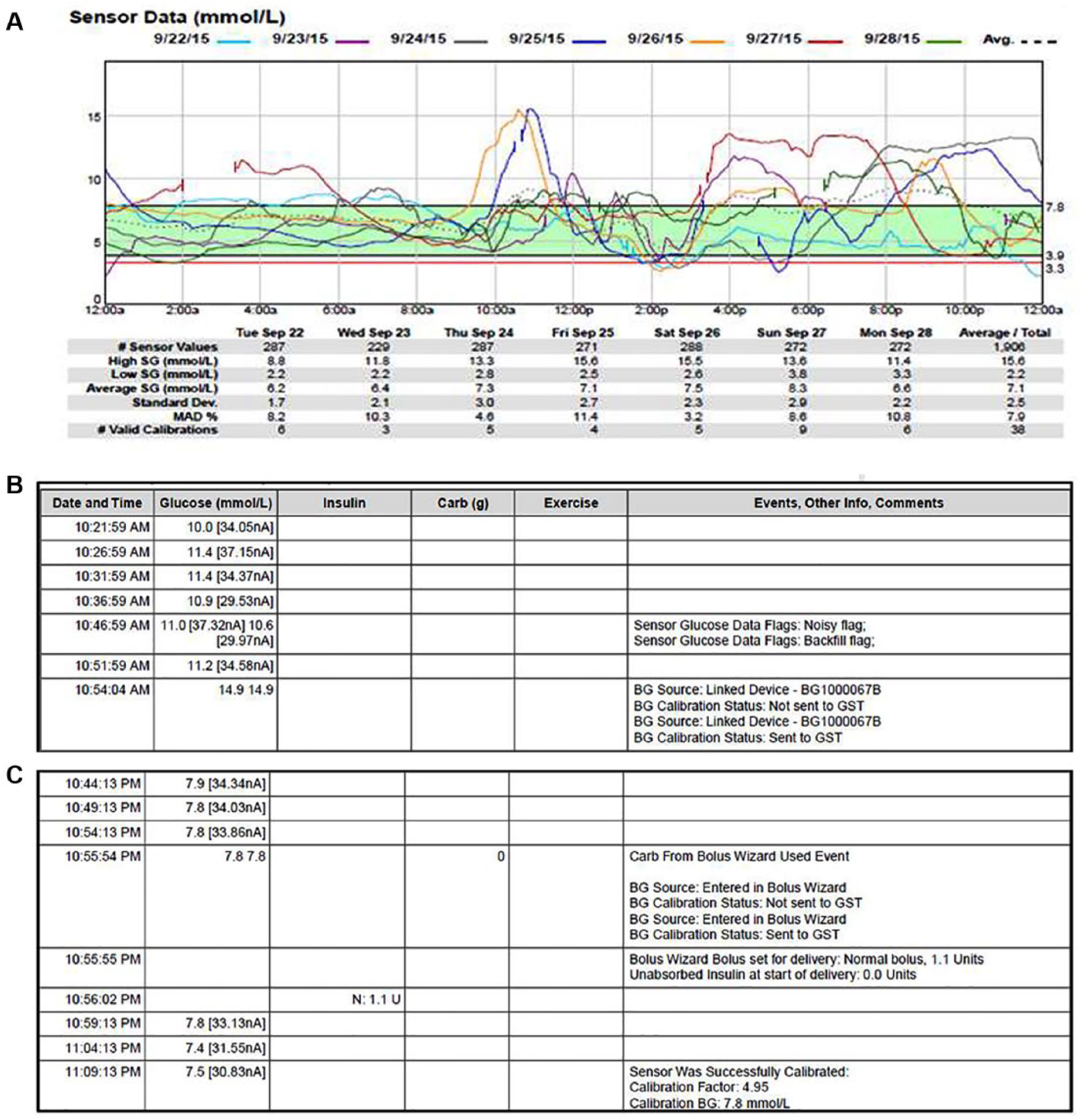
(a) Sensor daily overlay for participant 4. (b) The right calibration technique. Blood glucose (14.9 mmol/l) was used for calibration with a corresponding sensor glucose of 11.2 mmol/l .The blood glucose meter is linked to the pump and hence sent to the pump for calibration. (c) Data table of participant 4. The sensor glucose (7.8 mmol/l) is entered into the bolus wizard and used for calibration.
Participant 5
HCP concern
The concern was carbohydrate consumption with a downward trend in SG.
Background
A 14.3-year-old with diabetes for 10.5 years and on pump therapy for 4.9 years was commenced on SAPT with Suspend before low enabled. Participant’s glycemic control was optimal with HbA1c of 56 mmol/mol (7.3%). However, a subsequent increase in HbA1c to 61 mmol/mol (7.7%) was noted.
Behavior
Fear of hypoglycemia caused the participant to ingest excessive carbohydrates if SG was <5 mmol/l or downward arrow trends were observed. Foods with high glycemic index were ingested following pump suspension with resultant high SG. Although the sensor was regarded to be useful for the participant and the parents to review the alerts and arrows, hypoglycemia was prevented with food rather than permitting insulin suspension. Behavior was due to mistrust in the Suspend before low function. HCP advice was to allow the pump to suspend and resume based on SG readings. The family was also further informed regarding the use of appropriate carbohydrates if the Suspend before low function was overridden.
Discussion
This case series demonstrates the need for clinicians to be vigilant of patient interaction with CGM information as exposure to CGM systems can sometimes lead to unexpected behaviors in adolescents with type 1 diabetes. Adolescence is a time of physical and emotional growth associated with risk taking, and vulnerability. The risk taking behaviors along with the new found autonomy often leads to poor self-management, which impacts glycemic control. 9 As sensor readings are real-time, the constant exposure to glucose levels, at least in some patients, could drive them to erratic behaviors that can negatively impact their management.
Anecdotally, studies have highlighted the prohibitive cost, variable accuracy and information overload to users11,12 as some of the detriments of CGM uptake in the real world. 12 However, an adolescent could possibly respond in different ways to the glucose levels, given the extra information available to them. They could be overwhelmed and choose to ignore it (participant 3) or be obsessively driven to achieve perfect readings (participants 1 and 2). Before commencing CGM, it is important to identify with the patient their individual goals, the perceived benefits and barriers to the use of these systems. Although it may be difficult to predict an individual’s response to CGM levels, awareness of maladaptive patient responses to low and high glucose values should guide the HCP to address these issues in their clinical review. These erratic behaviors displayed with CGM use bring to light the need for open dialogues with patients and families to facilitate discussions to explore the potential disadvantages and on-going hindrances with the use of the system. Incorporating education and direct open conversations about high-risk behaviors as part of the routine assessment at regular clinic visits is vital to prevention.
Evaluation of the pump and sensor data to review the SG profile and the patient interaction with the system is paramount during the clinic visits and should complement a thorough clinical review. The review of these data can at times unveil aberrant and unsafe practices as demonstrated in our case series. The time taken for review should be taken into consideration when planning the set-up of pump and/or sensor clinics. The need for ongoing discussion and adequate CGM education should be factored in with the clinical visits. This will be crucial for staffing and resources with the increase in patients using CGM systems.
This case series also explores the issue of trust in technology by relinquishing control to an automated system and highlights the dichotomized behavior seen between “no-trust” (participant 5) vs “blind trust” (participant 4). Trust of the individual in the system determines reliance on the system. 13 These issues of trust and mistrust of technology are also widely seen in automation with autonomous cars and autopilots in aircrafts. Trust is not a static thing but dynamic with humans learning to predict what systems will do and vice versa (Bayesian analysis and prediction) in what has been termed interfacing mutual “mental” models. 14 User trust will depend on the early experience of the individual with the system and this further accentuates the importance of adequate and graded training of the individual to effectively use technology. This is also significant with the further evolution of partial closed-loop to hybrid and fully automated closed-loop systems.
To summarize, clinicians should be aware of the possibility of unsafe behaviors by the adolescents with type 1 diabetes to address glycemic excursions. These behaviors can be unveiled following review of the pump and/or sensor data. Families should be adequately informed and empowered with problem-solving strategies for safe clinical management and open discussions should be facilitated to encourage and maintain a good clinician and patient collaboration to achieve the best outcomes. The issues of trust and mistrust with technology will guide individual’s reliance on the automated systems.
Footnotes
Acknowledgements
PLGM study group: (1) Institute of Endocrinology and Diabetes, The Children’s Hospital at Westmead, NSW, Australia: Julie Klimek, Kristine Heels, Tracey Jopling, Dr Geoffrey Ambler; (2) Department of Endocrinology and Diabetes, Royal Children’s Hospital, Melbourne, Australia: Rebecca Gebert, Miles Clarkson Fletcher, Prof Fergus Cameron; (3) Department of Endocrinology and Diabetes, John Hunter Children’s Hospital, Newcastle, Australia: Tenele Smith, Amy Crawford, Jordan Rafferty, Dr Bruce King; (4) Department of Endocrinology and Diabetes, Women’s and Children’s Hospital, Adelaide, Australia: Tania Kelly, Stephanie Oates, Dr Janice Fairchild; (5) Department of Endocrinology and Diabetes, Princess Margaret Hospital, Perth, WA, Australia: Dr Mary B. Abraham, Dr Charles Czank, Jennifer Nicholas, Carol Cole, Leah Laurenson, Heather Roby, Grant Smith, Prof Elizabeth Davis, Prof Timothy W. Jones.
Abbreviations
CGM, continuous glucose monitoring; HCP, health care practitioner; PLGM, Predictive Low Glucose Management; SAPT, sensor-augmented pump therapy; SG, sensor glucose; SMBG, self-monitoring of blood glucose.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JDRF Australia, the recipient of the Australian Research Council Special Research Initiative in Type 1 Juvenile Diabetes, through the JDRF mentored fellowship awarded to MBA.