
Abstract
Background:
Continuous glucose monitoring (CGM) may improve the management of patients with type 2 diabetes hospitalized in the general ward by facilitating the detection of hyper- and hypoglycemic episodes. However, the lack of data on the accuracy and safety of CGM have limited its application.
Methods:
A prospective pilot study was conducted including 38 patients hospitalized in the general ward with a known diagnosis of type 2 diabetes mellitus (DM) and hyperglycemic individuals without a history of DM with a blood sugar of 140-400 mg on admission treated with a basal bolus insulin regimen. Inpatient glycemic control and the incidence of hypoglycemic episodes were compared between detection by CGM of interstitial fluid for up to 6 days and point-of-care (POC) capillary blood glucose monitoring performed pre- and postprandially, before bedtime and at 3
Results:
No differences in average daily glucose levels were observed between CGM and POC (176.2 ± 33.9 vs 176.6 ± 33.7 mg/dl, P = .828). However, CGM detected a higher number of hypoglycemic episodes than POC (55 vs 12, P < .01). Glucose measurements were clinically valid, with 91.9% of patients falling within the Clarke error grid A and B zones.
Conclusions:
Our preliminary results indicate that the use of CGM in type 2 patients hospitalized in the general ward provides accurate estimation of blood sugar levels and is more effective than POC for the detection of hypoglycemic episodes and asymptomatic hypoglycemia.
Background
Inpatient dysglycemia, including hyperglycemia, hypoglycemia, and increased glycemic variability, is associated with an increase in hospital-related complications and mortality. 1
Hyperglycemia in diabetic patients hospitalized in the general ward, surgical units,2-5 or the intensive care unit 6 is associated with poor clinical outcomes, including longer hospital stay and higher deconditioning, sepsis, and mortality rates. Therefore, optimization of glycemic control in hospitalized patients has been proposed as a necessary and cost-effective strategy. 6 However, implementation of an intensive glucose management program increases the risk of hypoglycemia.
Hypoglycemia is a risk factor for inpatient mortality among patients in intensive care6-10 and in those admitted to the general ward, 11 and it increases the risk of prolonged hospitalization. 12 Furthermore, undetected or untreated hypoglycemic events may lead to neurological damage, cognitive decline, seizures, and coma.13,14
Continuous glucose monitoring (CGM), which provides information on changes in interstitial glucose levels, including the direction and rate of change, was proposed as the method of choice to minimize the risk of hypoglycemia among hospitalized patients. Measurement of blood glucose levels every 5 to 10 minutes has advantages over the traditional bedside capillary point-of-care (POC) testing, which is performed before meals and at bedtime. 1
Despite these advantages, recent clinical guidelines do not currently recommend the use of CGM because of insufficient data on its accuracy and safety. 15 The aim of the present study was to evaluate the accuracy and safety of CGM in adult type 2 diabetic patients hospitalized in the general ward, and to assess its potential advantages over POC for the detection of symptomatic or asymptomatic hypoglycemic episodes.
Methods
Patients and Insulinization Strategy
The present study was a prospective pilot study that included 38 medical management patients hospitalized in the general ward of the University Hospital San Ignacio in Bogota, Colombia, between March 2011 and February 2012, with a known history of diabetes mellitus (DM) or without a previous diagnosis of DM but with a blood sugar level on admission of 140-400 mg/dl. Patients excluded from the study were as follows: younger than 18 years or older than 80 years, undergoing surgery during the course of hospitalization, those treated with systemic steroids, requirement for enteral or parenteral nutrition, requiring intensive care management during hospital stay, chronic liver disease or cirrhosis, creatinine clearance < 30 cc/min, pregnant, mental conditions limiting an understanding of the study, and patients with diabetic ketoacidosis or hyperosmolar nonketotic state.
Patients enrolled in the study provided blood samples for HbA1c (measured by high performance liquid chromatography), creatinine, glycemia, and capillary blood glucose measurement. Treatment with oral antidiabetic agents and crystalline insulin and NPH (Neutral Protamine Hagedorn) was discontinued, and patients were placed on a basal insulin bolus regimen with glargine and glulisine (Lantus and Apidra, Sanofi-Aventis, Bridgewater, NJ) according to the protocol described in the RABBIT study. 11 Briefly, patients were started on an initial total daily insulin dose (TDD) of 0.3-0.5 U/kg according to the basal glucose levels, age, and creatinine values. One half of the TDD was administered as a basal glargine dose, and the remaining 50% was administered with glulisine in 3 equal doses at mealtimes. In patients with a fasting glucose of 140-180 mg/dl (7.7-10 mmol/l), the basal insulin dose was increased by 10%, whereas in those with a fasting glucose >180 mg/dl (10 mmol/l), it was increased by 20%. The objective of the treatment was to achieve a fasting glucose level of 100-140 mg/dl (5.5-7.7 mmol/l) and preprandial glucose of 140-180 mg/dl (7.7-10 mmol/l).
Continuous Glucose Monitoring and Point-of-Care Capillary Blood Glucose Monitoring
POC glucose monitoring was performed before meals and at 2 h after meals, at bedtime, and at 3
CGM was initiated on the second day of hospitalization with a CGMS iPro-2 (Medtronic, Northridge, CA ) following the insertion of a subcutaneous sensor in the anterior region of the abdomen of each patient, and monitoring was performed for a maximum of 6 days. Calibration of the CGM was done following the iPro-2 producer recommendations, using capillary blood glucose measures in range between 40 and 400 mg/dl, 1 and 3 hours after the insertion of a subcutaneous sensor, and then previous to each meal until the end of the study. At the end of this period, the equipment was removed and data were downloaded using the iPro CareLink software. Patients and hospital personnel were blinded to the results of CGM. Hypoglycemic episodes were defined as a blood glucose level < 70 mg/dl (< 3.8 mmol/l) as detected by conventional capillary blood glucose monitoring regardless of the presence of symptoms. Additional evaluation was done defining hypoglycemia as a glucose level < 60 mg/dl (< 3.3 mmol/l).
Statistical Analysis
Statistical analyses were performed using SPSS v18 (SPSS Inc, Chicago, IL). Descriptive data analysis was performed. The rates of incidence of hypoglycemia were calculated based on the data obtained by CGM and POC, and the incidence rate ratio (IRR) between them was determined. Student’s t test was used to compare systems, global, pre- and postprandial average glucose levels. Values of P < .05 were considered statistically significant.
Results
Characteristics of the Study Participants
The study included 38 patients, of which most were men. Two patients were excluded for missing data on CGM. The average age on admission was 66.1 ± 8.6 years, the duration of diabetes was 14.8 ± 9 years, glucose level on admission was 251 ± 9 mg/dl, BMI was 26.5 ± 4.9 kg/m2, and glycosylated hemoglobin was 9.26 ± 2.62% (78 ± 17 mmol/mol). At least 1 comorbidity was detected in 84.2% of patients (Table 1). The average number of days under CGM was 4.3 ± 1.0 days.
Characteristics of the Study Participants (N = 38).
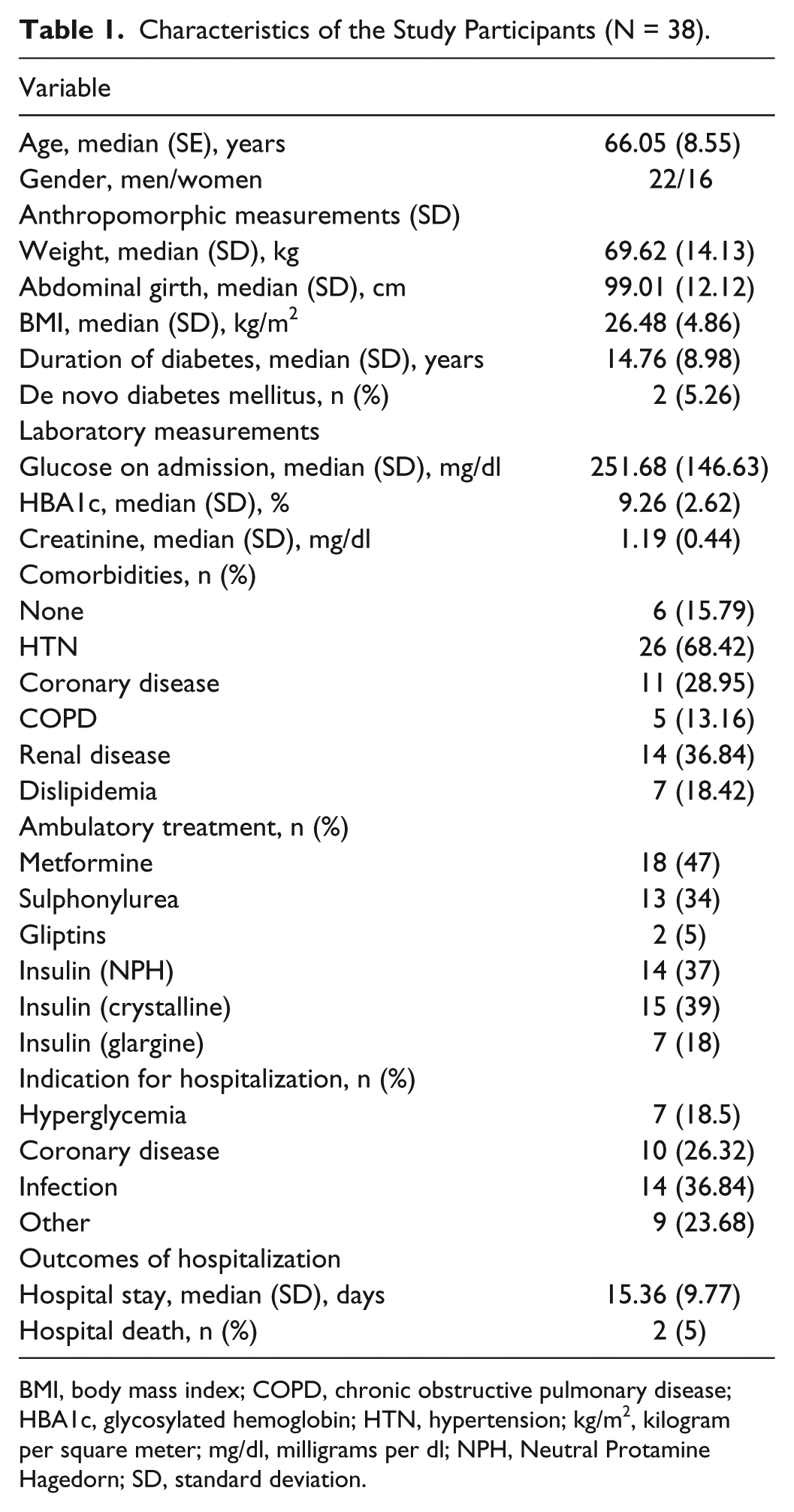
BMI, body mass index; COPD, chronic obstructive pulmonary disease; HBA1c, glycosylated hemoglobin; HTN, hypertension; kg/m2, kilogram per square meter; mg/dl, milligrams per dl; NPH, Neutral Protamine Hagedorn; SD, standard deviation.
Glucose Concentration
No significant differences in the average daily glucose levels measured by CGM and POC were observed after the first day of treatment (176.2 ± 33.9 vs 176.6 ± 33.7 mg/dl, P = .828) (Figure 1). Ten patients (26.3%) had at least 1 episode of hypoglycemia defined as glucose level < 70 mg /dl (< 3.8 mmol/l) during follow-up. Overall, 55 episodes of hypoglycemia were detected by CGM (1.45 episodes per patient) compared to 12 episodes detected by POC (0.32 episodes per patient), indicating that CGM was more effective than POC for the detection of hypoglycemia (IRR = 4.58, 95% confidence interval: 2.42-9.40, P < .0001).
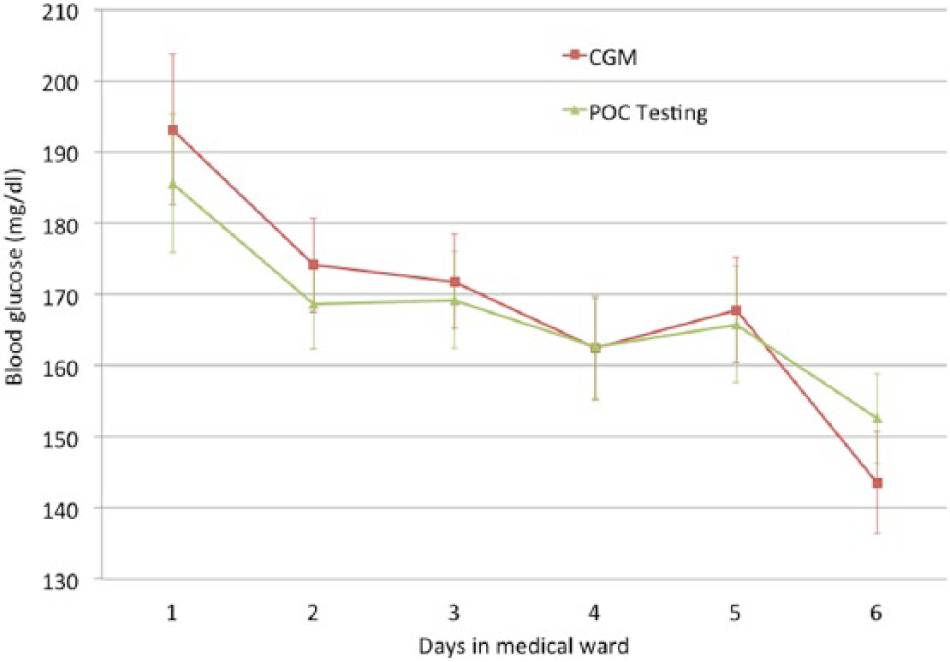
Average daily glucose measured by CGM and POC. Average glucose measured by CGM or POC glucose monitoring at bedside during the first 6 days of hospitalization. The red line represents CGM measurements and the green line represents POC measurements.
Of the total hypoglycemic episodes, 60% occurred between dinner and 6
Hypoglycemia (<70 mg/dl) Detected by POC Glucose Monitoring and CGM.
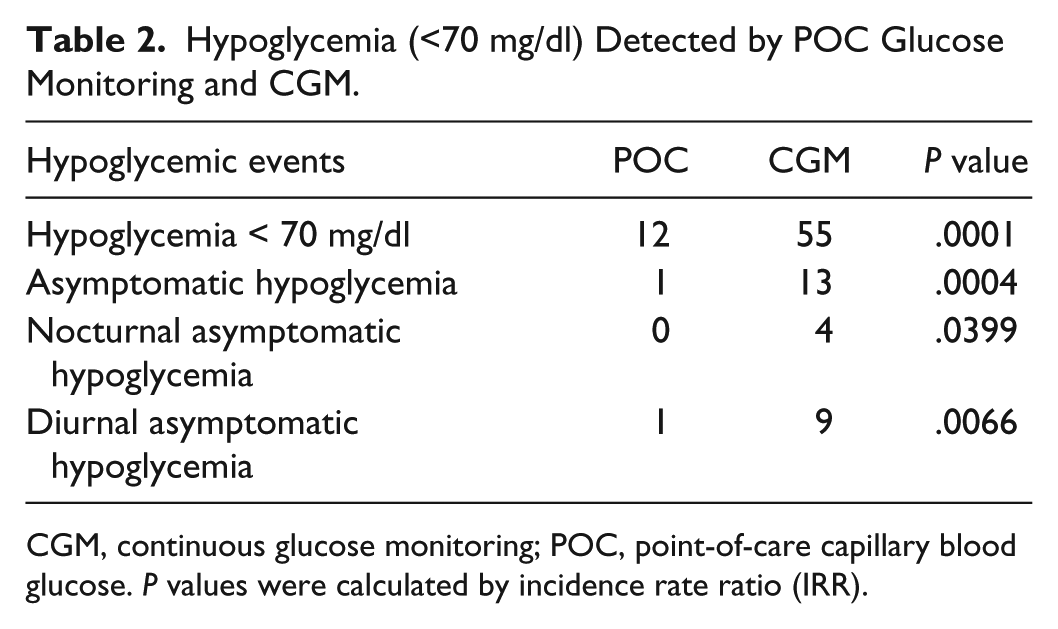
CGM, continuous glucose monitoring; POC, point-of-care capillary blood glucose. P values were calculated by incidence rate ratio (IRR).
Defining hypoglycemia as glucose level below 60 mg /dl (<3.3 mmol/l), we found 30 episodes detected by CGM compared to 6 episodes detected by POC (IRR = 5, 95% confidence interval: 2.5-14.28, P < .0001). No episodes of hypoglycemia < 40 mg/dl were detected by either of the 2 methods.
Accuracy of Measurements
The numerical accuracy of the measurements obtained by CGM was determined according to the ISO criteria (16). Measurements were found to be accurate for both, glucose values > 75 mg/dl (4.33 mmol/l), with an absolute difference of means of 12.9%, and for measurements < 75 mg/dl, with only 0.6% of the values showing a difference greater than 15 mg/dl (0.83 mmol/l) compared to POC. Pearson correlation analysis revealed a positive correlation between interstitial glucose values by CGM and corresponding capillary blood glucose (r = .79). In addition, the clinical accuracy was determined using the Clarke error grid, which showed that 91.9% of the data were within the A and B zones (Figure 2).
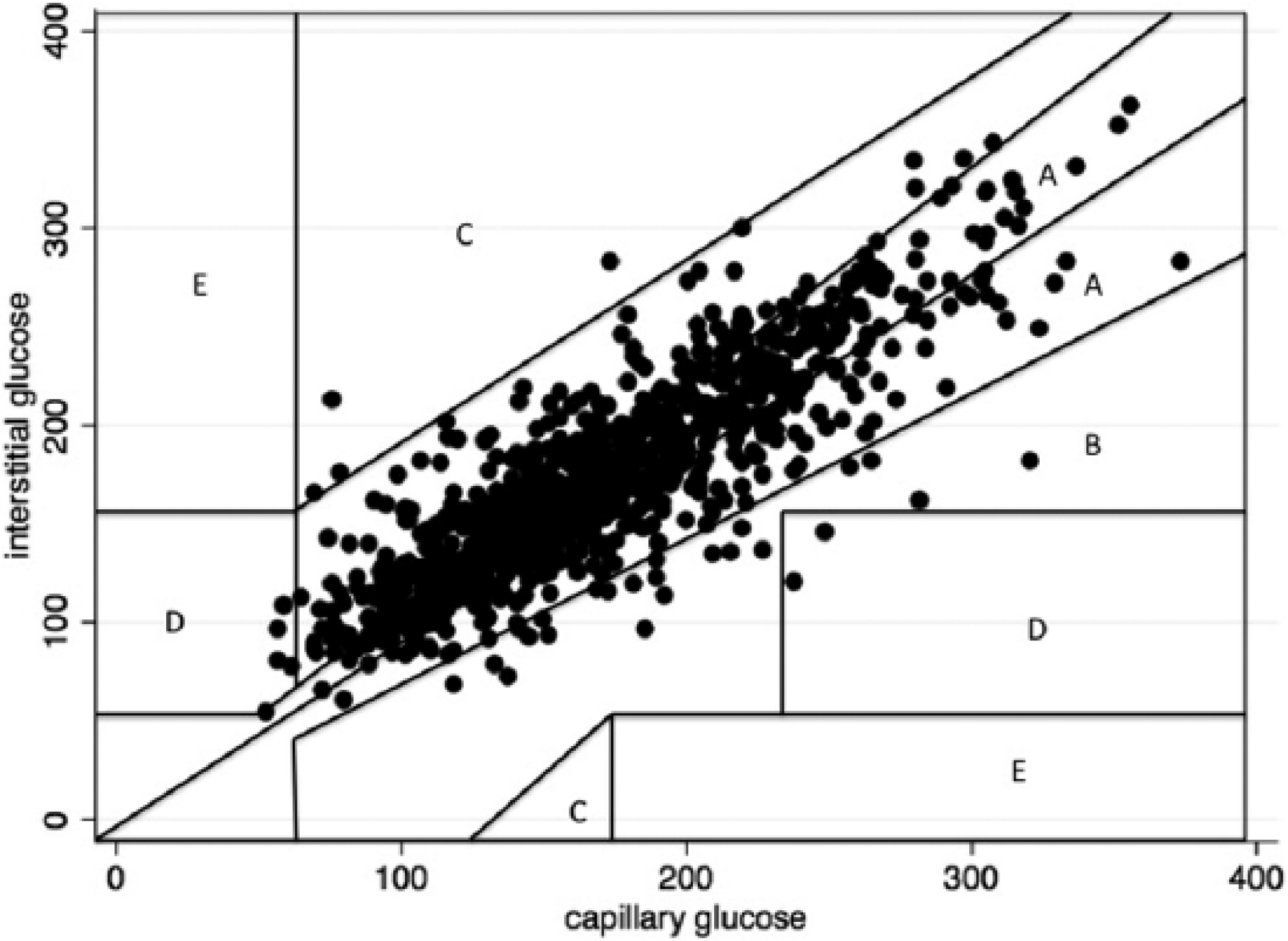
Clinical accuracy of blood glucose levels measured by continuous glucose monitoring. Clarke error grid comparing blood glucose levels measured by CGM and POC. The grid predicts the type of clinical error that can be committed when there is a difference between the 2 assessment methods. Differences that fall within the A and B zones indicate the lack of clinical consequences.
Discussion
Adequate glycemic control is an important objective in the management of hospitalized type 2 diabetic patients, and a basal bolus insulin regimen is the method of choice to achieve this goal.15,16 The primary objective of the present pilot study was to perform a systematic comparison of CGM and POC for the detection of episodes of hypoglycemia, and our results showed that CGM is the superior method. In addition, we evaluated the accuracy of measurements obtained by CGM and POC, both to determine average glucose levels and for the detection of hypoglycemic episodes. The present study is the first evaluation limited to type 2 general medicine diabetic patients, among which the average BMI was found to be in the overweight range (BMI: 26.7), which is lower than that reported in previous studies, in which the majority of patients were obese. Similar to previous reports,17,18 our study showed that the average daytime glucose level measurements are comparable between CGM and POC. However, the main difference between the 2 methods was the ability to detect episodes of hypoglycemia. In the present cohort, 55 episodes of hypoglycemia were detected by CGM, of which 86.7% were detected exclusively with this method. The fact that more than 50% of these hypoglycemic episodes occurred between dinner and 6
The present study also provides important information regarding the accuracy of glucose measurements obtained by CGM. We independently evaluated the accuracy of the results obtained based on glucose values above and below 75 mg/dl (4.33 mmol/l) according to the ISO guidelines. 19 Our results showed that the measurements were accurate in both instances, demonstrating the usefulness of CGM for the detection of both hyper- and hypoglycemia. Similarly, assessment of the clinical accuracy of the results using Clarke’s error grid showed that the clinical decisions potentially made on the basis of these results should be accurate in 92% of the cases. Furthermore, the safety of this technology was demonstrated by the fact that no severe symptoms associated with subcutaneous catheter insertion or infectious complications were detected among our patients.
The main limitation of our study was the relatively low number of episodes of hypoglycemia among our patients, which limits the assessment of the accuracy of the results in the glucose range below 75 mg/dl (4.33 mmol/l). Future studies should evaluate this issue in further detail.
CGM could potentially improve our ability to detect episodes of hyper- and hypoglycemia among hospitalized patients over that of POC. However, the use of this technology has generated concern because of its high cost and because data on its accuracy and safety in inpatients are limited; therefore, its use is not currently recommended by international guidelines. 15
The present results provide a basis for further investigation aimed at determining whether real-time CGM, when combined with a predefined and specific therapeutic regimen, can reduce the incidence of hypo- and hyperglycemia episodes in the context of type 2 diabetes patients hospitalized in the general ward, as previously demonstrated in type 1 ambulatory patients, in which CGM was shown to reduce the duration of hypoglycemic episodes, 20 and in critical care patients, in which studies have shown a lower incidence of severe hypoglycemia.18,21 However, because this information is not currently available, the recommended method for the monitoring of glucose levels is POC glucose monitoring before meals and at bedtime, as proposed by international guidelines.
Conclusions
Our preliminary results indicate that the use of CGM in type 2 patients hospitalized in the general ward provides accurate estimation of blood sugar levels and is more effective than POC for the detection of hypoglycemic episodes and asymptomatic hypoglycemia.
Footnotes
Acknowledgements
The publication of this article was possible thanks to the support of the Pontificia Universidad Javeriana (ID PPTA 5938).
Abbreviations
BMI, body mass index; CGM, continuous glucose monitoring; DM, diabetes mellitus; IRR, incidence rate ratio; POC, point-of-care capillary blood glucose; TDD, total daily insulin dose.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AMG reports speaker fees from NovoNordisk, Elli Lilly, MSD, Novartis, and Medtronic and research grants from Medtronic, Novartis, and Abbott. CR receives fees for a patient education program with NovoNordisk and insulin pump patient training with Medtronic. PA has participated in advisory boards and has received speaker fees from AstraZeneca, BMS, Boehringer, GSK, Jansen, J&J, Lilly, MSD, Novartis, and Sanofi and has participated in original research involving Sitagliptin and insulin Glargine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.