
Abstract
Background:
Mobile health and patient-generated health data are promising health IT tools for delivering self-management support in diabetes, but little is known about provider perspectives on how best to integrate these programs into routine care. We explored provider perceptions of a patient-generated health data report from a text-message-based diabetes self-management program. The report was designed to relay clinically relevant data obtained from participants’ responses to self-assessment questions delivered over text message.
Methods:
Likert-type scale response surveys and in-depth interviews were conducted with primary care physicians and endocrinologists who pilot tested the patient-generated health data report in an actual clinical encounter. Interview guides were designed to assess providers’ perceptions of the feasibility and utility of patient-generated health data in routine clinical practice. Interviews were audiotaped, transcribed, and analyzed using the constant comparative method.
Results:
Twelve providers successfully piloted the summary report in clinic. Although only a minority of providers felt the report changed the care they provided (3 of 12 or 25%), most were willing to use the summary report in a future clinical encounter (9 of 12 or 75%). Perceived benefits of patient-generated health data included agenda setting, assessment of self-care, and identification of patient barriers. Major themes discussed included patient selection, reliability of patient-generated health information, and integration into clinical workflow.
Conclusion:
Providers perceived multiple benefits of patient-generated health data in overcoming common barriers to self-management support in clinical practice and found the summary report feasible and usable in a clinical context.
Keywords
Self-management support is a cornerstone of diabetes care: guidelines recommend individualizing education based on periodic assessment of an individual’s diabetes knowledge, self-management skills and behaviors, and health beliefs and attitudes. 1 However, physicians face numerous barriers to providing ongoing and comprehensive self-management support, including lack of time, inadequate training, and scarce resources.2-4
Health information technology (HIT) is a promising tool to offset challenges physicians face in delivering self-management support,5,6 particularly in diabetes. 7 Through HIT, including patient portals, mobile applications, and automated phone technologies, providers and patients can communicate beyond the 15-minute office visit. Health care providers, through automated technology, can send patients reminders and education to support self-management, and can also collect information from patients on self-care activities and other self-assessments.
Such “patient-generated health data” are taking on greater importance in the context of the recent 2009 Health Information Technology for Economic and Clinical Health Act (HITECH), which requires providers to integrate electronic health records (EHRs) into the care environment and demonstrate meaningful use. 8 Although not yet finalized, current proposed recommendations for stage 3 meaningful use, set to take effect in 2016, require participating hospitals and physicians to electronically accept patient-generated health information. 9 While the potential benefits of patient-generated health data are widely appreciated, little is known about how best to integrate them into routine clinical care. Key research questions remain about what patient-generated data would be useful to providers, how and when the data should be captured, and how best to integrate them into clinical workflow.
Critical to any successful implementation of health IT is provider buy-in. 10 Despite national interest in patient-generated health data, little is known about health care professionals’ opinions on use of this data in a clinical context. Such information would inform policy makers and implementers not only about patient-generated health data and EHRs but also the integration of mobile health into clinical care.
At the University of Chicago Medicine (UCM), we have implemented a mobile phone-based diabetes self-management program in which patients receive tailored health information via text message and reply to questions about self-management. 11 In addition, we created a summary report of the data to share with individual participants’ physicians. In this study, we used quantitative (ie, surveys) and qualitative methods (ie, in-depth interviews) to evaluate the feasibility and utility of using patient-generated health data within clinical practice, with a specific focus on the utilization of patient data created from interactive mobile technologies designed to enhance diabetes self-management support.
Methods
Study Setting
This study took place as part of a mobile phone-based diabetes self-management support program called CareSmarts. CareSmarts is a demonstration project supported by the University of Chicago Health Plan (UCHP) and offered free of charge to member-patients with type 1 or type 2 diabetes whose physicians at UCM provide consent. Through CareSmarts, patients receive automated text messages on their personal mobile phones consisting of reminders and educational messages and text back responses to self-assessment questions. These questions include self-care activity assessments (eg, “Did you take your medications today? yes/no”) and self-reflection questions (“What is your biggest barrier to controlling diabetes? text back a short reply”). Self-assessments are monitored by nurse-care managers at UCHP. For example, if a patient reports low medication adherence, CareSmarts alerts a nurse–case manager to contact the patient.
Summary Report Development
The CareSmarts summary report was designed by a team of researchers to relay clinically relevant patient-reported health data from participants’ text message responses. The report was developed to fit on a single page and to be read and interpreted by a clinician in less than 1 minute. Based on the principles on usability testing, 12 iterative feedback was obtained from 3 physician end users to improve relevance, ease of use, and comprehension. The final summary report included the following sections (see Figure 1): (1) progress in CareSmarts (eg, modules completed), (2) patient-reported medication adherence, (3) patient-reported self-glucose monitoring, (4) nurse-care manager alerts, and (5) barriers to diabetes self-care.
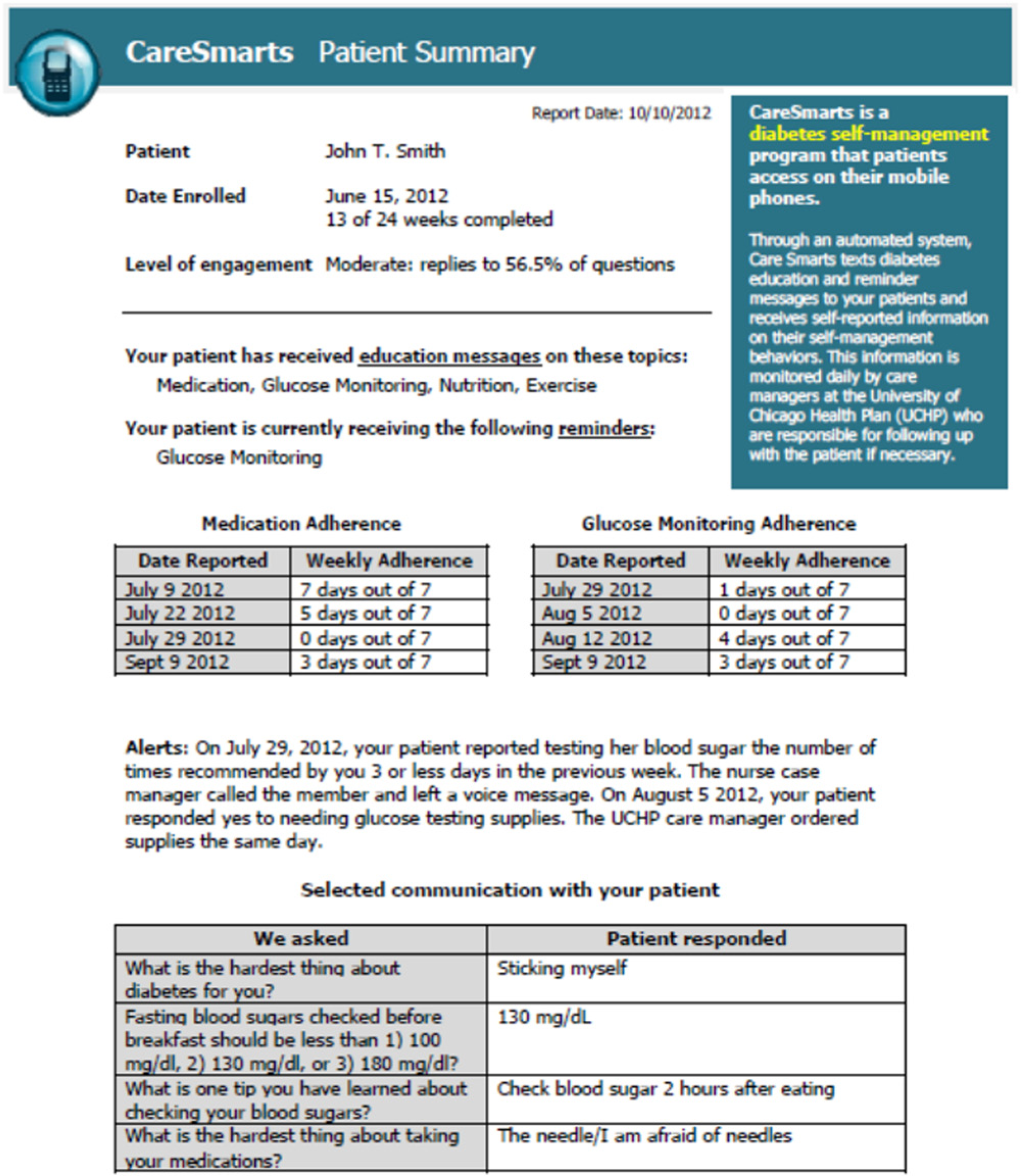
Sample CareSmarts summary report.
Study Participants and Methods
After study approval from the Institutional Review Board, primary care physicians and endocrinologists who had at least 1 patient enrolled in CareSmarts were recruited. Only faculty (vs medical residents or fellows) were included in the study; both full-time and part-time clinicians were included. Of the 31 providers contacted for recruitment, 14 agreed to participate and 12 successfully piloted the summary report. No providers declined to participate, but several did not respond within the recruitment timeframe. Two providers did not complete the study because their patients did not attend their appointment. Twelve postsurveys and 11 interviews were conducted. One provider declined the interview because he was involved with study design.
Providers were via email contacted within a week of their next clinic visit inviting them to participate. Consenting providers were provided a summary report prior to the visit with no specific instructions about when and how to use the report. Following the visit, providers completed an experience survey consisting of questions with multiple choice and 5-point Likert-type scale responses. Providers also participated in a 30-minute individual interview with a physician–member of the research team (SN) in the provider’s office. A topic guide was created to discuss the provider’s approach to diabetes self-management support, experience piloting the summary report in clinic, and perspectives on patient-generated health data.
Data Analysis
Descriptive statistics were performed on Likert-type scale response and multiple choice survey questions. Consistent with established qualitative methods, data collection and analysis were conducted simultaneously. 13 We continued to recruit physicians until theme saturation was met (ie, no new themes emerged from the data). Individual interviews were audiotaped, transcribed verbatim, and imported into ATLAS.ti 6.0 software. All deidentified, anonymous transcripts were coded using the constant comparative method, with no a priori hypotheses, by a team of 5 investigators with experience in medicine, diabetes education, and public health. 14 A codebook was developed using an iterative process. All 5 coders independently coded the first transcript. That is, individual names or “codes” were given to thought units within the transcripts that described the content (eg, “perceived reliability of patient data”). The group then met as a team to discuss the transcript, come to consensus regarding the coding nomenclature, and create uniform coding guidelines. Subsequently, each transcript was independently coded by 2 randomly assigned reviewers, who then met to resolve coding discordance. Outstanding issues were resolved by the group. The group met regularly to discuss new codes and emerging themes; the themes were discussed iteratively until consensus was reached and no new themes arose from the transcripts.
Results
Provider Characteristics
Ten of the 12 providers (83%) surveyed identified themselves as primary care physicians with the remainder identifying themselves as endocrinologists or diabetes specialists. Nine of the providers (75%) were female, and their median duration in practice was 7 years (range 1-36 years). Nine providers (75%) identified themselves as full-time clinicians or clinician–educators and 3 (25%) as clinician–researchers with part-time clinical responsibilities.
Providers’ Experience Piloting the Report
Table 1 summarizes the providers’ experience piloting the patient-generated data summary report. All but 1 “agreed” or “strongly agreed” that the summary report was easy to use and understandable. A minority of providers “agreed” or “strongly agreed” that the report influenced their understanding of their patients (3 of 12 or 25%) or changed the care they provided (4 of 12 or 33%). No large differences were observed in providers’ perceptions of the usefulness of different data elements—medication adherence, glucose monitoring adherence, and open-ended responses. Most providers (9 of 12 or 75%) “agreed” or “strongly agreed” that they would be willing to use the summary report in the future.
Provider Experience Piloting the CareSmarts Summary Report (n = 12).

Table 2 presents representative quotes of each of the themes regarding patient-generated health information. Each theme is discussed in the sections below.
Themes and Representative Quotes From Physicians About Patient-Generated Health Information.

Patient Selection
Providers had different perspectives on which patients were most appropriate for patient-generated health information. Some providers favored receiving these data from all patients with diabetes, but many wanted to target only specific subpopulations such as those with poorly controlled diabetes. Other providers wanted the ability to select individual patients on a case-by-case basis, for example, only on patients who were poor historians or had limited insight into their disease.
Content of Information
Providers generally found the types of patient-generated health data included in the summary report valuable and often suggested new content domains. These included additional self-care activity assessments such as blood sugar readings, exercise, and nutrition; assessments of barriers such as costs; and behavioral assessments such as self-efficacy and diabetes knowledge. Providers generally agreed that a combination of quantitative and qualitative data was helpful, and many were particularly influenced by the qualitative data.
Reliability of Information
Providers expressed few concerns about the reliability of patient-generated health data. Rather most providers felt that patient data collected via mobile phones may be more accurate than information collected during a clinic visit. They reported this in part because data collected at more frequent intervals and not just during clinic visits may have less recall bias and in part because of patients’ tendency to want to “please the doctor.” However, most providers saw this information as a complement to, not a replacement for, provider-directed history taking. They saw the patient-generated health report as a screening tool.
Usefulness of Information
Providers widely agreed that patient-generated health information could be useful to their practice but for varying reasons. However, most providers did not feel the information directly influenced the care they provided or their clinical decision-making. Five subthemes were identified within the theme of information usefulness as described below.
Setting an agenda
Providers reported that patient-generated health information could be useful for agenda setting. For example, if a patient reported low adherence to blood sugar monitoring but high adherence to medication taking, the provider could focus the visit on blood sugar monitoring.
Assessing self-care activities
Providers found the self-reported adherence data collected through the texting program helpful for assessing self-care activities. Although providers routinely collected this information during the clinic visit, they found it useful to have another source of data.
Identifying patient barriers
The report was also useful for identifying patient barriers to diabetes self-management. Providers particularly found patient responses to self-reflection questions such as “What’s the hardest thing about your diabetes?” helpful.
Understanding the patient’s perspective
Providers found the subjective information patients provided useful in understanding the patient perspective. This was particularly true for new patients (where patient perspectives were not yet known) and for patients with whom providers had previously experienced communication difficulties (and thus patient perspectives were not well understood).
Increasing patient activation
A few providers felt that the very act of patients reporting health information might encourage patients to take greater ownership over their health. For example, asking patients to report their weekly adherence (“How many days in the past week did you take all of your diabetes medications?”) may itself increase patient activation.
Accessing Information and Integrating Into Clinic Workflow
Nearly all providers agreed that the best time to receive the patient-generated health report was immediately before a scheduled clinic visit. While some providers saw the potential benefits of receiving reports between clinic visits (eg, monthly) or when urgent issues arose, none felt this was practical or feasible. Providers agreed that the report should be sent directly to them rather than to a nurse or care manager and be accessible through the electronic medical record.
Willingness to Use
Providers reported a high willingness to use the patient-generated health information report in clinic. Because the report was generated automatically and took less than a minute to review, they felt it would not burdensome to use. At the same time, some providers felt it may actually improve clinic efficiency.
Other Concerns
Some providers raised concerns about patient-generated health information. The most common was access to information technology in low-income and minority populations, which would limit the availability of patient-generated health data in patients who often needed it most and risk increasing health disparities.
Discussion
In this study, we explored provider perceptions of a patient-generated health data report pilot tested in a clinical encounter. The data were obtained from a mobile health diabetes self-management program in which patients received tailored health information via text message and texted back responses to automated self-assessment questions. Providers perceived multiple benefits of patient-generated health data in overcoming common barriers to providing self-management support in clinical practice and found our summary report feasible and usable in the clinic setting.
While mobile technologies have shown promise in supporting diabetes self-management,15,16 they are unlikely to be widely adopted or effective unless they are clinically linked. 7 The challenge then becomes in integrating technology-enabled self-management support interventions into clinical care. Despite the importance of physician buy-in, 17 few studies have examined provider perceptions of health IT-enabled interventions or explore how best to integrate them into clinical practice. This study helps address this important research gap.
Our study suggests that patient-generated health data constitute a feasible tool for linking mobile health programs to clinical care and may play a role in diabetes self-management support. Practice guidelines suggest that self-management support be tailored to the individual based on an assessment of a patient’s diabetes knowledge, self-management skills and behaviors, and health beliefs and attitudes, 1 yet this is seldom achieved in clinical practice. In our study, by standardizing and automating patient self-assessment, patient-generated health data addressed common provider barriers such as lack of time and reliable information. The data were also useful in agenda setting. By reviewing self-assessment data prior to the clinic visit, providers were able to organize the visit around addressing specific barriers and patient needs. Thus, we found that patient-generated health data can help prepare clinics to have “proactive, prepared clinical teams,” a key component of the chronic care model.18,19
Our results temper some of the enthusiasm for the potential of patient-generated health data to improve quality of care. Providers were divided on the usefulness of the summary report when piloted in an actual clinic encounter. Only some providers felt the data changed their understanding of the patient, and fewer found that it changed the health care decisions they made. A key result was that the usefulness of the data was not uniform across all patients with diabetes, suggesting that providers may need to individually select patients for whom patient-generated health data is most appropriate. This finding should be explored in future research and may have important implications for how health systems choose to implement the proposed stage 3 meaningful use requirement on patient-generated health data. 9 In addition, although nearly every provider reported a willingness to use the summary report in a future clinic encounter, providers wanted to receive the report only in the context of a scheduled clinic visit when they could reliably act on the information. Many proponents of patient-generated health data believe that it will facilitate between-visit care, but our findings suggest that without significant clinic redesign this may be not feasible.
To our surprise, providers had few concerns about the reliability of patient-generated health data. Many, in fact, reported that the anonymity of electronic self-assessments may increase the accuracy of the self-reported data compared to physician interview, which has been reported elsewhere. 20 Moreover, providers placed greater confidence in adherence data collected weekly than less frequently at clinic visits because of the lower risk of recall bias. In fact, the capture of patient data in real time, and in their natural environment, has been used in the social sciences as a strategy to reduce recall bias. 21 This ecological momentary assessment (EMA) method is an advantage not only for scientific studies, but also for the clinical utilization of such data.
Physicians valued both quantitative and qualitative patient-generated health data, a finding that was also observed in a study of provider perceptions of personal health records. 22 As much of the current discussion on patient-generated health data is on objective data such as ambulatory blood pressure readings, policy makers should make note of this observation in setting standards for meaningful use.
While this study focuses on the use of patient-generated health data within the clinical setting, it is important to note that such data has potential for use outside of the clinical encounter, particularly as a means of reengaging patients not routinely interfacing with the health system for care and for continuing communication with patients between clinic visits. However, providers in this study reported a willingness to use the summary report immediately prior to clinic visits, and were less willing to use it between episodes of care. Thus, creating greater financial incentives for population-based health promotion and prevention would likely increase the utilization of such patient-generated health data outside of fee-for-service-based clinical encounters.
Providers’ major concern was the availability of patient-generated health data among racial/ethnic minorities and elderly patients who may not have access to digital technologies. The digital divide in these groups has been well documented, particularly with computers and access to broadband.23,24 A major advantage of our intervention is that mobile phones enjoy high rates of usage by racial and ethnic minorities and low-income groups.25,26 Nevertheless, making these technologies affordable and accessible across socioeconomic groups is an important priority for addressing health disparities.
This study has several limitations. First, our findings are from 1 academic medical center in an urban, underserved African American community and therefore may not generalize to other primary care settings. Second, while a wide range of physicians participated in the study, almost half of those contacted did not agree to participate. This may have skewed our sample toward physicians with an interest in mobile technology or patient-generated health data. Third, our sample size was relatively small.
Nonetheless, our study has several strengths. First, we used EMA techniques to capture patient data, thus limiting the recall bias among patient participants in the CareSmarts program. Second, we utilized both quantitative and qualitative methods, which better enable us to triangulate the data. Third, we included both primary care physicians and subspecialists (ie, endocrinologists), which enhances the generalizability of our findings to a broader range of physicians.
Conclusions
In summary, patient-generated health data collected through a mobile phone-based diabetes self-management program were translated into a summary report and pilot tested in a clinical encounter by primary care physicians and endocrinologists. Although providers perceived many potential benefits of patient-generated health data in self-care assessment and identification of patient barriers, only a minority of providers found that they directly affected their treatment decisions. Patient-generated health data may be more of a tool for improving self-management support than clinical decision making, a finding that should be explored in future studies.
Footnotes
Abbreviations
EHR, electronic health record; HIT, health information technology; IT, information technology; UCHP, University of Chicago Health Plan; UCM, University of Chicago Medicine.
Authors’ Note
Dr Nundy is currently employed by Evolent Health.
Declaration of Conflicting Interests
Dr Nundy previously cofounded and was part owner of mHealth Solutions, LLC, a mobile health software company, but currently has no financial relationship or affiliation with the company.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Nundy was supported by the Agency for Healthcare Research and Quality Health Services Research Training Program (T32 HS00084). This research was also supported by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) (R18DK083946), Diabetes Research and Training Center (P60 DK20595), the Chicago Center for Diabetes Translation Research (P30 DK092949), and the Alliance to Reduce Disparities in Diabetes of the Merck Foundation.