
Abstract
Background:
Population health management approaches can help target diabetes resources like Diabetes Self-Management Education and Support (DSMES) to individuals at the highest risk of complications and poor outcomes. Little is known about patient characteristics associated with DSMES receipt since widespread uptake of telemedicine for diabetes care in 2020.
Methods:
In this retrospective cohort study, we used electronic medical record (EMR) data to assess patterns of DSMES delivery from May 2020 to May 2022 among adults who used telemedicine for type 2 diabetes (T2D) endocrinology care in a large integrated health system. Multilevel regression models were used to evaluate the association of key patient characteristics with DSMES receipt.
Results:
Of 3530 patients in the overall cohort, 401 patients (11%) received DSMES. In adjusted multivariable logistic regression, higher baseline HbA1c (odds ratios [OR] 3.10 [95% confidence interval 2.22-4.33] for HbA1c ≥9% vs <7%), insulin regimen complexity (OR 3.53 [2.59-4.80] for multiple daily injections vs no insulin), and number of noninsulin medications (OR 1.17 [1.05-1.30] per 1 additional medication) were significantly associated with receipt of DSMES, whereas rurality and area-level deprivation of patient residence were not.
Conclusions:
Diabetes Self-Management Education and Support remains underutilized in this cohort of adults using telemedicine to access endocrinology care for T2D. Factors contributing to clinical complexity increased the odds of receiving DSMES. These results support a potential population health management approach using EMR data, which could target DSMES resources to those at higher risk of poor outcomes. This risk-stratified approach may be even more effective now that more people can access DSMES via telemedicine in addition to in-person care.
Introduction
Type 2 diabetes (T2D) is a challenging diagnosis, requiring active daily self-management for more than 27 million Americans. 1 From managing new medications to changing one’s diet and activity levels, day-to-day care of diabetes affects nearly every dimension of life. Diabetes Self-Management Education and Support (DSMES) is an evidenced-based approach to give patients with diabetes the knowledge, skills, and confidence to troubleshoot common issues, collaborate with care providers, develop actionable goals, and manage stress. 2 Diabetes Self-Management Education and Support is linked to improved behavioral, clinical,3,4 psychosocial,5,6 and cost-effectiveness 7 outcomes for adults with T2D. As a result, national guidelines recommend DSMES as part of comprehensive diabetes care, including key points like initial diagnosis, changes in treatment or life circumstances, development of new complications, and annually when treatment goals are not being met.2,8
Despite these proven benefits, DSMES is not routinely delivered to all patients who could benefit. Prior literature demonstrates that only 5% of Medicare beneficiaries receive DSMES within the first year after diagnosis, 9 and additional studies demonstrate low rates of delivery in other populations.10,11 Barriers to utilization are multifactorial and tied to issues in the provider, participant, health system, and environmental domains. One major obstacle has been access to in-person care for patients with T2D who have geographic or transportation barriers, such as those who live in rural areas. Rural areas have fewer DSMES programs than metropolitan centers, meaning that patients with diabetes who live in these areas have been less likely to receive this critical care.12,13 With the recent shift toward telehealth during the COVID-19 pandemic, there is potential for more patients to overcome these barriers and benefit from participation in DSMES delivered virtually, a modality that has been shown to be effective.14 -16
Despite the potential for improved virtual access, systems-based factors like low referral rates by providers, inadequate numbers of diabetes care and education specialists (DCES), and poor reimbursement present additional challenges to optimal DSMES uptake.11,17,18 The population of adults with T2D in the United States is projected to triple to more than 60 million by 2060, and all patients cannot be served by the limited number of active DCES. 19 In addition, the growing popularity of advanced diabetes technology for T2D, such as continuous glucose monitors and insulin pumps, demands additional education and support for patients to realize the potential benefits of these devices.20,21 Diabetes care and education specialists are well positioned to support advanced self-management skills and enable patients to translate the increased insight and flexibility from diabetes technology into improved clinical outcomes and quality of life, thereby increasing demand for their services. 22 Given this dynamic, approaches such as population health management that link patients who are most in need with appropriate care resources are critical.
Population health management strategies leverage clinical data to identify and target care resources to patients at high risk for poor health outcomes. 23 These methods have been applied to a wide range of chronic diseases including congestive heart failure, 24 chronic kidney disease, 25 and atrial fibrillation 26 and can be used to increase diabetes care quality, prevent complications, and reduce health care costs. 27 Risk-based targeting of diabetes care resources has been applied across the diabetes spectrum, from lifestyle programs for prediabetes to inpatient glycemic management. 28 The use of electronic medical record (EMR) data to identify patients at high risk has been promoted as an approach to increase uptake of this underutilized resource and improve care coordination. 27
Despite this growing need, EMR data-driven approaches to proactively identify and deliver DSMES to high-risk patients have not yet been established. Little evidence exists to inform which patients currently receive DSMES. Furthermore, no studies have assessed updated DSMES utilization patterns since the shift toward hybrid virtual and in-person diabetes care delivery in the wake of the COVID-19 pandemic. Analysis of trends in which patients are receiving DSMES could inform a population health management approach to ensure that limited resources are deployed in an optimal manner. In this study, we aimed to assess current patterns of utilization of this high-value diabetes care resource among patients who use telemedicine to access endocrinology care in a setting where DSMES is readily available and reimbursable. In particular, we aimed to evaluate the association of patient characteristics, including medical treatment complexity (treatment regimen and comorbidities) and barriers to in-person care (residence in rural communities), with receipt of DSMES.
Methods
Study Design and Cohort
This retrospective cohort study included adults with T2D who had at least one telemedicine visit with an endocrinology provider in one of five clinics within the University of Pittsburgh Medical Center (UPMC) Division of Endocrinology and Metabolism between May 2020 and February 2022. Patients were followed up through May 2022, such that each patient had at least three months of follow-up after their endocrinology telemedicine visit. This study period was chosen to reflect a period of routine widespread telemedicine usage after significant care disruption during the COVID-19 pandemic. Data extracted from the EMR included patient baseline demographic information, laboratory results, active medication prescriptions, care utilization (including encounters with DCES and endocrinologists), as well as endocrinology visit modality (telemedicine vs in-person).
Patients had to be at least 18 years of age, have a primary care provider within the UPMC system, and have a diagnosis of T2D based on the International Classification of Diseases, Tenth Revision, code E11.X. In addition, patients had to have at least one active order for a diabetes medication to increase the likelihood that diabetes was being actively managed during the endocrinology visit, as opposed to other endocrine conditions. Given the focus on T2D, adults with diagnosis codes for type 1 or gestational diabetes were excluded. Patients with diagnosis codes for dementia or end-stage renal disease were excluded, as these conditions significantly alter diabetes treatment goals. Patients who died during the study period were excluded. Further details on cohort creation based on inclusion and exclusion criteria are provided in the Supplemental Material (Figure S1).
Clinical Setting
The Division of Endocrinology at UPMC serves patients across Western Pennsylvania, as well as neighboring areas of West Virginia, Ohio, and New York. The division covers a wide geographic area, including both rural and urban locations. Similar to many other centers, UPMC had robust uptake of telemedicine starting in March 2020 and has had persistent ongoing use, with approximately 30% of recent outpatient endocrinology visits conducted via telemedicine. Each of the five included clinics had at least one on-site DCES who received referrals from endocrinology providers and then provided individualized DSMES initial assessments and follow-up sessions (in-person or via telemedicine) based on patient needs.
Measures
The primary outcome of receipt of DSMES was defined as at least one education encounter with a DCES documented during the study period in the EMR, including in-person or telemedicine encounters. Encounters documented as patient phone calls, patient portal messages, and encounters with diabetes care team members who were not DCES were not included in this outcome. Patient characteristics of interest were assessed at the time of the first telemedicine endocrinology provider visit during the study period and included age, sex, Body Mass Index (BMI), baseline HbA1c, insulin use (categorized as no insulin, basal insulin only, or multiple daily injections (MDI) of insulin based on active medication orders), and number of noninsulin diabetes medications (tally of oral or injectable noninsulin diabetes active medications orders). Comorbidities were measured by using the Elixhauser Comorbidity Index score, 29 as this has been linked to health care utilization among adults with T2D in prior literature. 30 Demographic and social determinants of health predictors of interest included race, rurality, and Social Deprivation Index. Rurality was assessed using Rural Urban Commuting Area (RUCA) codes based on the patients’ home address five-digit ZIP code (where 1 represents urban areas, 2-6 represent suburban areas, and 7-10 represent rural areas), as rurality impacts diabetes care quality, outcomes, and access to DSMES.12,31 -33 Social Deprivation Index 34 is a composite measure of local-area-level deprivation based on the five-digit ZIP code which has been linked to health outcomes. 35 In order to accommodate patients with missing baseline HbA1c and BMI data, these variables were categorized, and patients with missing data were included in a distinct category. Encounters with DSMES were identified within the EMR based on encounter type, provider, and location and had to occur after the endocrinology provider visit, to avoid counting referrals from primary care or other providers. Receipt of DSMES was categorized as a binary variable indicating whether or not the patient received DSMES at any point during the study period. In addition, the number of encounters with an endocrinology care provider over the study period was assessed and standardized to an annual rate based on when the patient entered the cohort and the duration of follow-up.
Statistical Analysis
We assessed overall frequencies (percentages) and means (standard deviations) or medians (interquartile range; Q1, Q3) as appropriate, for baseline patient characteristics. Baseline characteristics were compared between those who did and did not receive DSMES using χ2 tests for categorical variables and two-sided Wilcoxon rank sum for continuous variables. We used multivariable logistic regression to model the relationship of key patient predictors of interest with the binary outcome or whether or not the patient received DSMES during the study period. Key predictors of interest included baseline HbA1c, insulin regimen, noninsulin medication count, Elixhauser Comorbidity Index, Social Deprivation Index, race, and rurality. In addition, we adjusted for covariates including patient age, sex, BMI, and the annual rate of visits with an endocrinology provider, as we hypothesized that this may reflect engagement in care and therefore be linked to both patient characteristics and receipt of DSMES. We report odds ratios (ORs) and corresponding 95% confidence intervals (CIs) for all variables included in the model. We assumed a type 1 error rate of 0.05 and made no adjustments for multiplicity. All analyses were performed using SAS Version 9.4 (SAS Institute Inc., Cary, NC).
This study was determined to be exempt by the University of Pittsburgh Institutional Review Board and was deemed to be exempt from informed consent. The results are reported in accordance with the Strengthening Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 36 A limited deidentified data set is available from the authors upon reasonable request.
Results
There were 3530 patients in the overall cohort as seen in Supplemental Figure 1. Characteristics of the study population are shown in Table 1. A total of 401 patients (11%) received DSMES during the study period.
Baseline Characteristics.
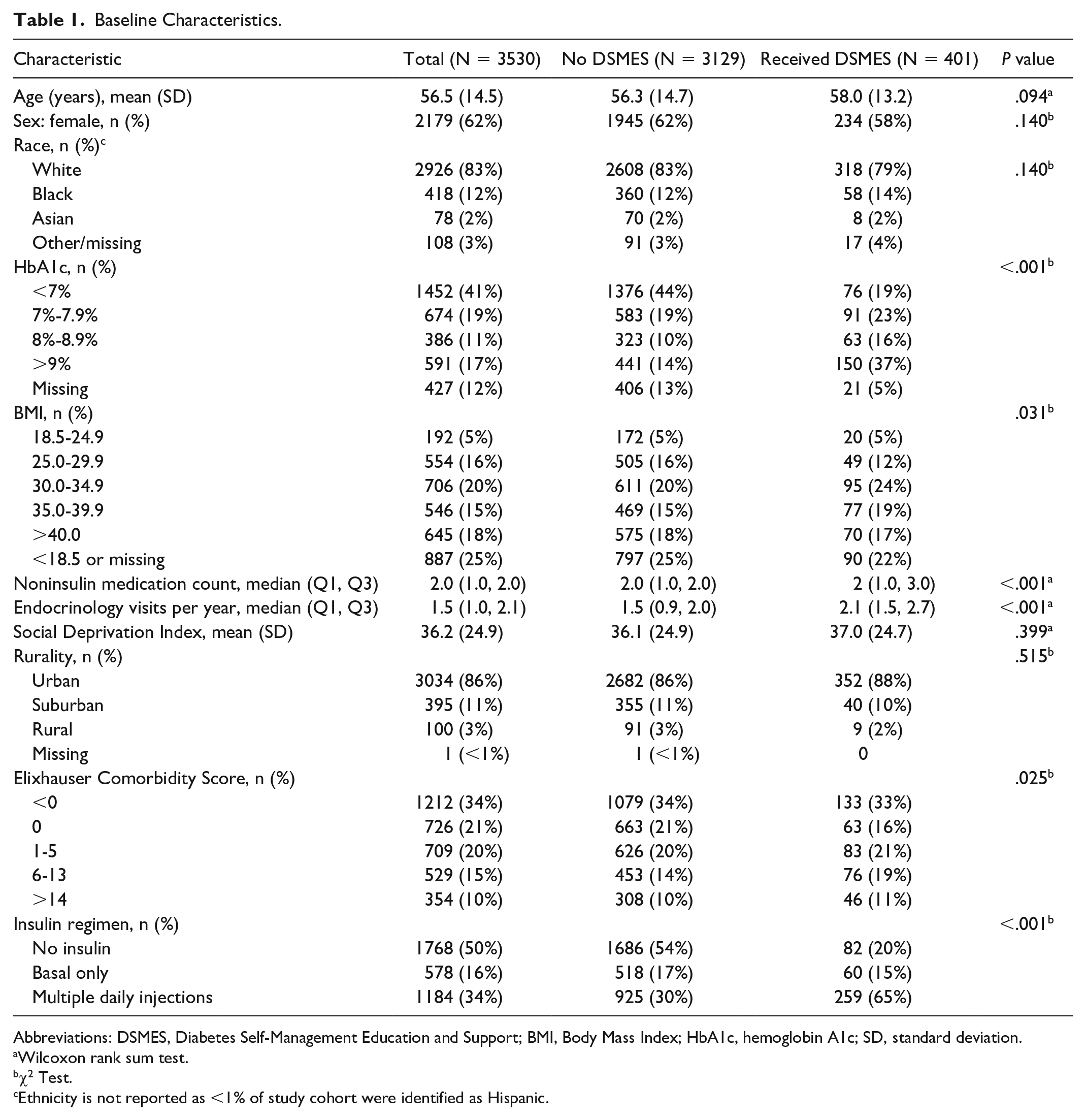
Abbreviations: DSMES, Diabetes Self-Management Education and Support; BMI, Body Mass Index; HbA1c, hemoglobin A1c; SD, standard deviation.
Wilcoxon rank sum test.
χ2 Test.
Ethnicity is not reported as <1% of study cohort were identified as Hispanic.
In unadjusted analyses, patients who received DSMES had significantly higher baseline HbA1c, BMI, noninsulin medication count, and endocrinology provider visits per year and more frequently used MDI of insulin. Patients who received DSMES also were more likely to have higher Elixhauser Comorbidity Index scores. Social Deprivation Index and rurality were not significantly different between patients who did versus did not receive DSMES in unadjusted analyses.
In adjusted multivariable regression models (Table 2), baseline HbA1c, insulin regimen complexity, and number of noninsulin medications were significantly associated with receipt of DSMES. Patients at all levels of elevated HbA1c had significantly higher odds of receiving DSMES than patients with HbA1c <7%. The addition of each noninsulin medication also significantly increased the odds of DSMES receipt (OR 1.17, 95% CI 1.05-1.30, P = .005). Patients who used MDI were more likely to receive DSMES than patients who did not use insulin (OR 3.53, 95% CI 2.59-4.80, P < .001). There was no significant impact of sex, race, Social Deprivation Index, rurality, or Elixhauser Comorbidity Index on receipt of DSMES in adjusted models. Patients with elevated BMI had significantly higher odds of receiving DSMES than those with BMI between 18.5 and 24.9. In addition, the number of annual endocrinology visits was significantly associated with increased odds of receipt of DSMES, with each additional visit over a 12-month period increasing the odds of DSMES (OR 1.77, 95% CI 1.56-2.01, P < .001).
Adjusted a Association of Patient Characteristics With DSMES Receipt.
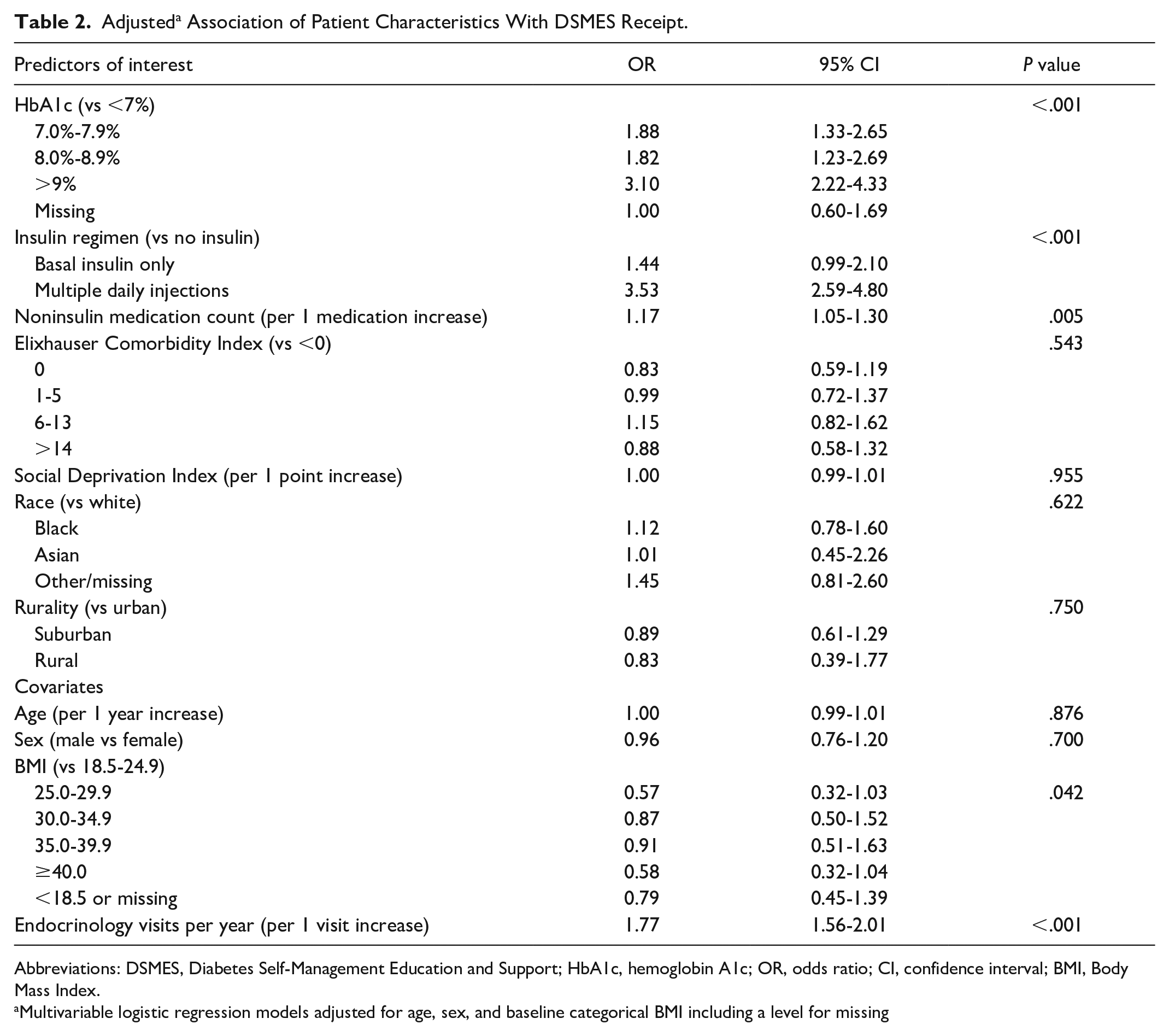
Abbreviations: DSMES, Diabetes Self-Management Education and Support; HbA1c, hemoglobin A1c; OR, odds ratio; CI, confidence interval; BMI, Body Mass Index.
Multivariable logistic regression models adjusted for age, sex, and baseline categorical BMI including a level for missing
Discussion
This study of adults with T2D who use telemedicine to access endocrinology care demonstrated that DSMES remains underutilized, with only 11% of patients receiving DSMES over the two-year study period. Although only a fraction of individuals received DSMES, this proportion is in line with rates of DSMES receipt in prior literature, which range widely from 5% 9 to more than 36%. 13 In this cohort, increased diabetes treatment complexity (e.g., use of multiple daily injections and increased number of noninsulin medications) was associated with receipt of DSMES. Individuals with intermediate HbA1c levels (7%-9%) were also more likely to receive DSMES, and those with HbA1c levels >9% had the highest odds overall. These findings suggest that individuals at the highest risk of complications from diabetes may already be prioritized to receive this important service in an unstructured referral system. However, there are likely additional opportunities to use informatics-based approaches with EMR data to target referral and receipt of DSMES to patients in greatest need. For example, comorbidity burden, which may significantly impact the complexity of diabetes self-management and need for ongoing support, was not associated with DSMES receipt. On the other hand, factors representing structural and social barriers to DSMES care delivery, including area-level deprivation and rurality, did not significantly impact the odds of receiving DSMES in this cohort. Although this analysis cannot account for all structural and sociodemographic factors that impact care, these findings suggest that increased uptake of telemedicine may enhance access for patients who face traditional barriers to in-person DSMES delivery.
These findings provide new insight into current DSMES utilization and suggest multiple avenues to apply EMR data in population health management approaches that identify those patients most in need of evidence-based diabetes care resources. Similar approaches in other chronic conditions, such as chronic kidney disease, have evaluated the potential to advance effective and efficient clinical care by using EMR data to identify high-risk individuals and link them with evidenced-based treatments via targeted electronic consultations. 37 Population health management approaches could be applied to diabetes care by using data points extrapolated from the EMR, including clinical factors (e.g., specific treatment regimens, HbA1c values, high-risk comorbid conditions) to identify patients at the highest risk of poor outcomes and deliver care prompts for DSMES referral. Because patients who require MDI are at higher risk of poor diabetes outcomes including severe hyperglycemia and hypoglycemia and mortality,38 -41 this is one potential factor which could be used in a structured approach to target DSMES to patients most likely to benefit. In addition to identifying patients with high-risk clinical factors, similar strategies could target care resources to patients with social factors associated with disparities in diabetes care quality and outcomes. For example, one recent study demonstrated that the addition of a structured form identifying key clinical points which prompt DSMES referral within the EMR workflow resulted in higher rates of DSMES referral for medically underserved adults with T2D at a federally qualified health center. 42 These approaches have the potential to enhance quality and efficiency of diabetes care delivery, improve immediate clinical outcomes, and impact downstream effects including complications, health care utilization, and cost. In implementing and evaluating similar population health management interventions, providers and health systems can find ways to leverage the power and breadth of EMR data to optimize the DSMES referral and delivery process and make this critical resource as accessible and impactful as possible.
Harnessing the power of the EMR and telemedicine to deliver DSMES to patients with T2D and higher disease complexity may also help close gaps in guideline-based care. Prior research has demonstrated differences in DSMES receipt by sociodemographic factors such as age, racial identity, 43 rurality, insurance status, and region, 13 all of which reflect known structural barriers in the US health care system. These important studies are frequently conducted in primary care settings, where the majority of care for adults with T2D is delivered. In this study, uptake of DSMES was low even in an endocrinology setting, where patients with diabetes may be more likely to use diabetes technology and complex insulin regimens than those seen in primary care settings.44 -46 In addition, the endocrinology clinics in this study had direct access to on-site DCES, which is not available in many primary care and smaller specialty clinics settings. Thus, approaches to enhance optimal uptake and evidence-based utilization of DSMES are highly applicable both to endocrinology and primary care settings. By using EMR data to highlight individuals at high risk of poor outcomes, we can leverage telemedicine to support these vulnerable patients to overcome barriers to care, increase update of DSMES, and reduce disparities.
Limitations
There are several limitations to this study. First, results from an endocrinology care setting in a single health system may not generalize to DSMES utilization trends in other settings or regions. Furthermore, there is limited representation of patients from racial and ethnic minority groups and from rural areas in this study. Although the included patient population is similar to the demographics of Allegheny County where all included clinics are located, 47 this may limit generalizability and obscure care disparities experienced by groups underrepresented in this cohort. Similarly, findings may not apply to patients who face barriers to telemedicine use, such as those without broadband internet access. In addition, although we know that all patients used telemedicine to see their endocrinology care provider, we were not able to capture whether DSMES was delivered virtually or in-person or the content of DSMES sessions in this data set. As with all analyses of EMR data, miscoded or missing information may limit capture of DSMES encounters or other patient characteristics. Finally, we were not able to definitively assess whether patients used continuous glucose monitors or insulin pumps because of limitations in device prescription data in this data set and, thus, were not able to assess the impact of diabetes technology use on receipt of DSMES.
Conclusion
In this retrospective cohort study of adults with T2D using telemedicine to access endocrinology care, patients with increased clinical complexity were more likely to receive DSMES, but overall utilization was low in this specialty care setting. Structural barriers to in-person diabetes care, including rurality, were not associated with lower odds of DSMES receipt. This study underscores the potential for EMR-based risk stratification strategies to identify and target DSMES to patients in greatest need. With the expansion of telemedicine usage, these approaches may be even more effective in delivering crucial diabetes care resources to patients who can benefit most.
Supplemental Material
sj-docx-1-dst-10.1177_19322968231176303 – Supplemental material for Factors Associated With Receipt of Diabetes Self-Management Education and Support for Type 2 Diabetes: Potential for a Population Health Management Approach
Supplemental material, sj-docx-1-dst-10.1177_19322968231176303 for Factors Associated With Receipt of Diabetes Self-Management Education and Support for Type 2 Diabetes: Potential for a Population Health Management Approach by Timothy Bober, Scott Rothenberger, Jonathan Lin, Jason M. Ng and Margaret Zupa in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
BMI, Body Mass Index; DCES, diabetes care and education specialists; DSMES, Diabetes Self-Management Education and Support; EMR, electronic medical record; HbA1c, hemoglobin A1c; multiple daily injections (of insulin), MDI; T2D, type 2 diabetes; UPMC, University of Pittsburgh Medical Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants KL2TR001856 through the University of Pittsburgh from the National Center for Advancing Translational Sciences and 5TL1TR001858-07 TL1 Training Grant Support from the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.