
Abstract
We write this letter as a brief report of our personal observation on optimal frequency of blood glucose reporting by patients on insulin pumps to treatment teams. There are multiple studies showing efficacy of frequent home blood glucose monitoring for patients with diabetes in maintaining glycemic control.1,2 However, there are limited data regarding how frequently blood glucoses should be reported by patients with diabetes to their treatment teams, and how this frequency affects glycemic control. We focused on patients on insulin pumps in our study due to several factors, including the availability of downloading blood glucoses remotely with high volumes and statistical analyses with pump software such as Medtronic’s Carelink®, Omnipod’s CoPilot®, and Animas’s Diasend®, the increased reliability and volume of glucose reporting through pump software compared to written logbooks, and the presence of a dedicated insulin pump clinic with diabetes educators to help gather insulin pump reports. We hypothesized that patients on insulin pumps who reported glucoses at least once monthly would have less glycemic variability with less frequent hypoglycemic and hyperglycemic events than those who report infrequently.
We performed a prospective, observational study of all our veterans with diabetes on insulin pumps via analyses of their submitted glucose downloads over 4 months. This study protocol was approved by the Veterans Administration Nebraska–Western Iowa Health Care System Institutional Review Board. We grouped patients into frequent reporters if they submitted glucoses at least 4 times during the study period, and infrequent reporters if they submitted glucoses 1-3 times. We defined hyperglycemia as any blood glucose >180 mg/dL, 3 hypoglycemia as blood glucose <70 mg/dL, 4 and severe hypoglycemia as <50 mg/dL. 5 Univariate analysis was done with t test and chi-square tests. Poisson regression was used to compare hypoglycemia and hyperglycemia rates. P < .05 was considered significant.
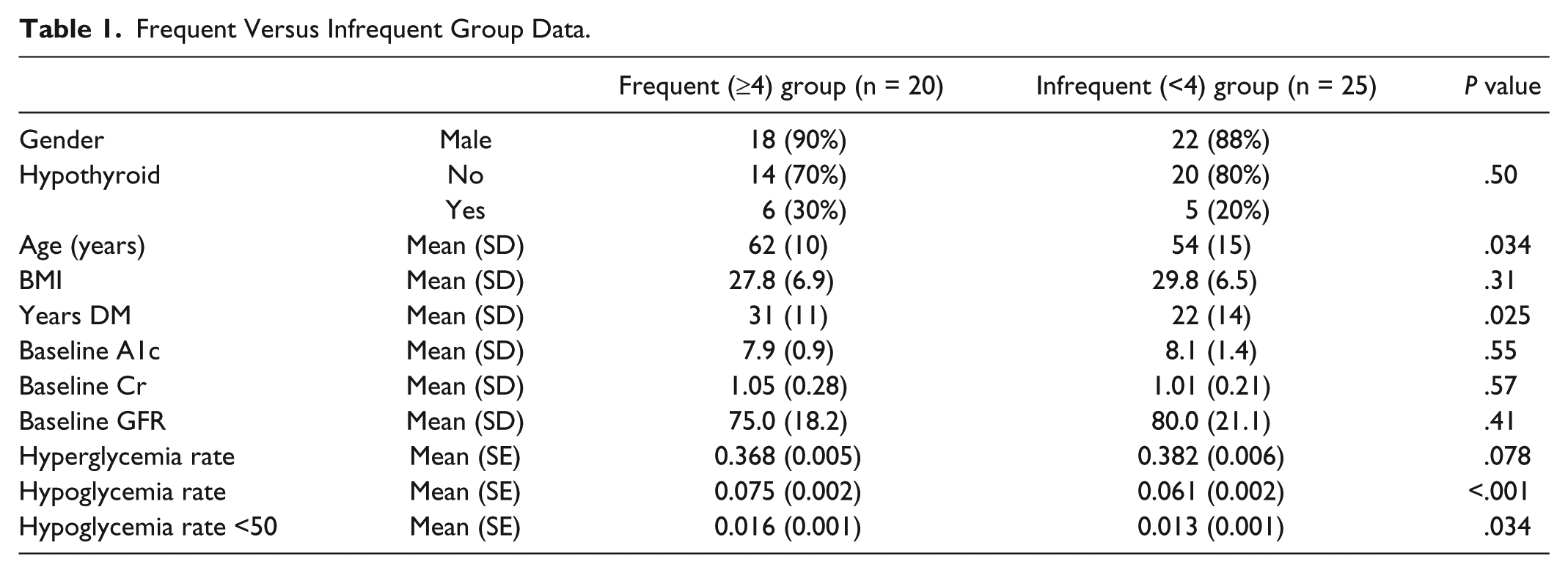
Forty-eight patients agreed to be included in the study; 3 of the 48 were later excluded from the study as they did not submit any blood glucoses over the 4-month study window. Frequent reporters (20 patients) showed a trend toward less hyperglycemia compared to infrequent reporters (25 patients) (36.8% vs 38.2%), though not statistically significant (P = .078) (Table 1). However, frequent reporters showed a higher rate of hypoglycemia (7.5% vs 6.2%) (P < .001) and severe hypoglycemia (1.6% vs 1.3%) (P = .034), compared to infrequent reporters. In addition, frequent reporters were older and had a longer duration of diabetes. When using the multivariate analysis for hyperglycemia, we discovered that younger patients, female patients, and patients with a higher baseline A1c all had statistically significant increased rates of hyperglycemia. Multivariate analysis also revealed significantly higher rates of hypoglycemia in females, patients with fewer years with diabetes, those with a lower BMI, and those with a higher baseline A1c.
Frequent Versus Infrequent Group Data.
In conclusion, the optimal frequency of blood glucose reporting by patients on insulin pumps to treatment teams may be individualized. Patients with increased glycemic variability may benefit from closer follow-up and more frequent glucose reporting, whereas patients with stable glycemic control with lower rates of hypoglycemia and hyperglycemia may require less frequent glucose reporting.
Footnotes
Abbreviations
BMI, body mass index; GFR,Glomerular Filtration Rate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was done through the VA Nebraska–Western Iowa Health Care System and is based upon work supported with resources and use of facilities at the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development and Biomedical Laboratory Research and Development. The contents do not represent the views of the Department of Veterans Affairs or the US government.