
Abstract
Background:
Modeling approaches demonstrate that improvement in the accuracy of blood glucose (BG) meters may lead to cost savings. An improvement of accuracy of BG meters on the basis of a reduction in error range from 20% to 5% has been reported to be associated with substantial cost savings in Germany.
Methods:
The aim of this study is to analyze potential cost savings related to a reduction in error range from 20% to 15% and 10% of glucose meters in Germany. The health economic analysis included the number of type 1 diabetic and the number of insulin-treated patients in Germany, the costs for glucose monitoring, a model on the effects of the improvement of accuracy on the impact of severe hypoglycemic episodes, HbA1c, and subsequently myocardial infarctions and the costs of diabetes-related complications in Germany. In the model, a reduction of 1% and 3.5% reduction in severe hypoglycemic episodes, and a 0.14% and 0.28% reduction in HbA1c was included.
Results:
In type 1 diabetes the savings could be equal to a reduction in health care expenditures of more than €1.0 million (20% vs 15% error range) and €3.4 million (20% vs 10% error range). Respectively, potential savings of more than €6.0 million and €20.1 million were calculated for the group of insulin-treated patients.
Conclusions:
The model demonstrates that a reduction of error range of BG meters from 20% to 15% and 10% may translate into substantial savings for the German health care system.
Prevention of hypoglycemic episodes has been identified as an important objective in diabetes management.1-3 Self-monitoring of blood glucose (SMBG) enables the optimization of diabetes management and prevention of both acute and chronic complications of diabetes.4,5 In particular, SMBG facilitates self-regulatory prevention of significant hypoglycemic episodes.6-8
The reliability of self-monitored glucose values is a prerequisite for an efficient and safe approach to treat patients to their target. Accuracy of SMBG, therefore, is a key aspect in this regard. 9 Recently, accuracy requirements have been tightened. According to the revised ISO standard 15197:2013, 95% of the blood glucose (BG) results shall fall within ±15 mg/dl of the reference method at BG concentrations < 100 mg/dl and within ±15% at BG concentrations ≥ 100 mg/dl. 10 The less restrictive ISO standard 15197:2003 loses its validity after a transitional period of 3 years. 11
We recently introduced a model for a health economic analysis, which is based on 4 main pillars. 9 Our analysis concluded that a reduction of a meter error from 20% to 5% was identified to be associated with a 10% reduction in very severe hypoglycemic episodes and a 0.39% reduction in HbA1c, which is translated into a 0.5% reduction of myocardial infarctions (MI). 9 According to the health economic analysis, the reduction in very severe hypoglycemic episodes and MI lead to cost savings of €24.14 per patient per year. Considering 390 000 type 1 diabetic patients or 2.3 million insulin-treated patients in Germany, these savings could be equal to a reduction in health care expenditures of more than €9.4 million and €55.5 million, respectively. 9
It was now the aim of the current modeling analysis to calculate clinical and economic impact using 2 examples with an error range of 10% and 15%, respectively. We also considered results of a recently published simulation on the risk for severe hypoglycemia due to BG measurement errors 12 and the updated UKPDS Risk Engine, which was published in September 2013, for the analyses.
Methods
The current modeling included updates of the previous analysis. 9 Two publications contributed to the rational background of the analysis.13,14 One publication included in silico simulations: 13 In the model, an insulin-induced hypoglycemia was simulated and SMBG was performed at the precise time when the reference BG level reached an array of 50-70 mg/dl. For each of these reference BG levels, the probability of SMBG not to detect the hypoglycemic episode was assessed as a function of the permitted meter error. 13 Taking a reference BG level of 60 mg/dl as an example, hypoglycemia was reported to be always detected at an SMBG error of 5%. The likelihood of not detecting that hypoglycemic event was found to increase to 1%, 3.5%, and 10% for SMBG errors of 10%, 15%, and 20%, respectively. 13 In the study, the deterioration of overall glucose control (HbA1c) created by increased SMBG inaccuracy was also estimated. The increase in average BG needed to offset hypoglycemia was translated into an increase in HbA1c using the formula recommended by the American Diabetes Association (ie, “28.7 × A1C − 46.7 = estimated average glucose value”). 14 The needed increase in average BG was found to be associated with an increase in HbA1c by 0.01 at 5% error, 0.12 at 10% error, 0.26 at 15% error, and 0.40 at 20% error, respectively. 14
Another study simulated the additional risk for severe hypoglycemia due to BG measurement errors of 5 different SMBG systems for both type 1 diabetic patients and type 2 diabetic patients requiring multiple daily injections based on results of a real-world accuracy study. 12 In the study, the most accurate system had a standard deviation of 9.9 mg/dl and a mean error of −1.0 mg/dl and the least accurate system had a standard deviation of 18.2 mg/dl and a mean error of +2.5 mg/dl. 12 The differences between severe hypoglycemic episodes attributable to a meter’s specific error profile ranged from 0.44 to 0.75 per patient per year in type 1 diabetes and, respectively, from 0.11 to 0.19 in type 2 diabetes. 12
In the current analysis the previous model was applied 9 and developed further. Table 1 summarizes the results of the data incorporated into the analysis. 9
Clinical and Economic Data Incorporated Into the Analysis. 9
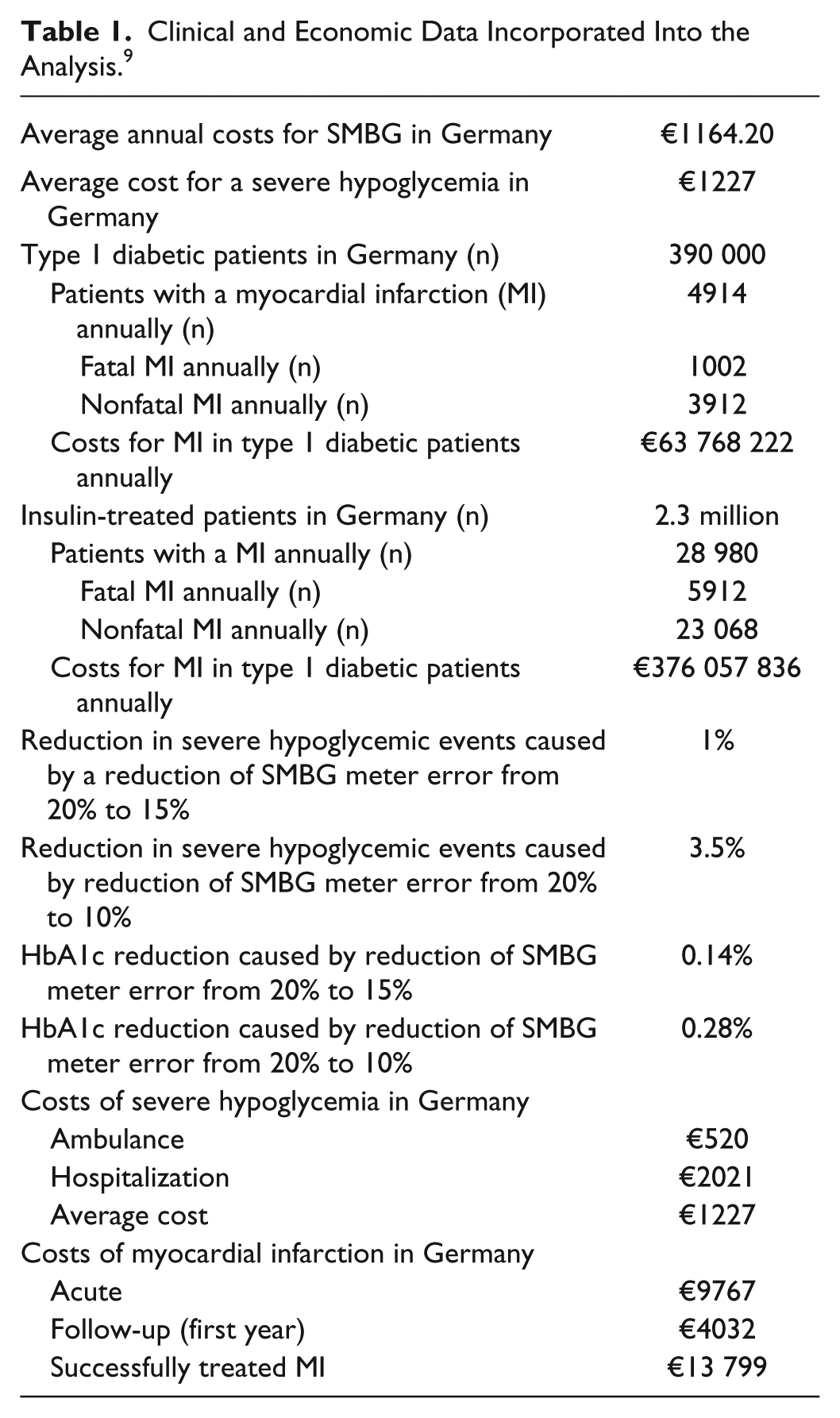
Four domains were included into the model, as previously described: 9 First is the number of insulin-treated diabetic patients in Germany. 9 Second is the cost of glucose monitoring in Germany. 9 Third is an analysis of the impact of higher accuracy on hypoglycemia, HbA1c, and subsequently cardiovascular complications. Taking the previous analysis, 9 and the data regarding hypoglycemia due to misdosing of insulin, 12 it was assumed that a reduction of error range from 20% to 15% leads to a 1% reduction of severe hypoglycemic episodes due to undetected BG levels < 60 mg/dl and misdosing of insulin. Respectively, a reduction of error range from 20% to 10% was assumed to cause a 3.5% reduction of severe hypoglycemic episodes. A rate of 0.19 times per patient and year for very severe hypoglycemic episodes (need for medical assistance or hospitalization) was included. 15 In the current analysis, the recently published UKPDS Risk Engine was applied to compute the effects of a reduction in HbA1c on cardiovascular outcome. 16 To compute the impact of a HbA1c reduction on the reduction of diabetes-related complications, we used the EDIC cohort for the analysis and defined the characteristics of a typical cohort of patients with insulin-dependent diabetes, equal to the cohort in the EDIC trial at year 11. 17 Fourth is the cost of diabetes-related complications in Germany. 9 In 2.3 million German patients with insulin-treated diabetes, 28 980 patients with an MI were calculated per year, of whom 5912 have a fatal event and 23 068 have a nonfatal event. 9 Total costs of MI in the entire group of insulin-treated patients are calculated to be as follows: 5912 cases × €9767 + 23 068 cases × €13 799 = €57 742 504 + €318 315 332 = €376 057 836. 9
Results
Cost Analysis of Improvement of Accuracy From 20% to 15%
Based on a rate of 0.19 severe hypoglycemic events per patient and year and a 1.0% reduction in severe hypoglycemic episodes, savings per patient were calculated as follows: €1227 × 1.0% × 0.19 = €2.33 (Table 2).
Results of the Cost Analysis (Reduction of Error Range From 20% to 15%).
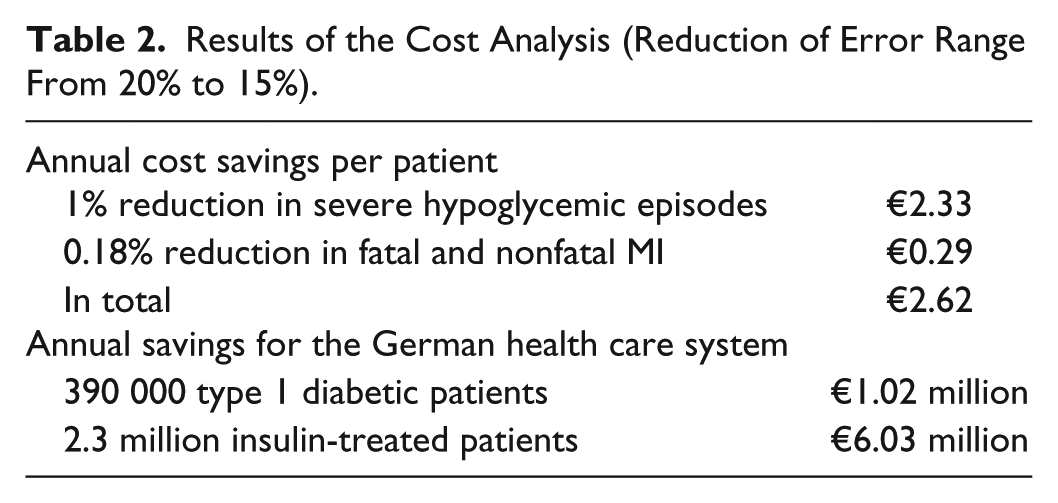
The reduction of the error range from 20% to 15% leads to a HbA1c reduction of 0.14%. 13 According to the UKPDS Risk Engine, this translates into a 0.18% reduction in CHD. 16 A 0.18% reduction in fatal and nonfatal MI translates into savings of €376 057 836 × 0.18% = €676 904 per year or €676 904 / 2.3 million patients = €0.29 per insulin-treated patient per year.
Adding annual savings due to prevented hypoglycemia (€2.33 per patient per year) and to MI (€0.29 per patient per year), total savings of €2.62 per patient and year were modeled. In the group of 390 000 type 1 diabetic patients in Germany, this will add to potential annual savings of €1.02 million. Savings in 2.3 million patients with insulin-treated diabetes will add up to €6.03 million.
Cost Analysis of Improvement of Accuracy From 20% to 10%
Based on a rate of 0.19 severe hypoglycemic events per patient and year, and a 3.5% reduction in severe hypoglycemic episodes, savings per patient were calculated as follows: €1227 × 3.5% × 0.19 = €8.16 (Table 3).
Results of the Cost Analysis (Reduction of Error Range From 20% to 10%).
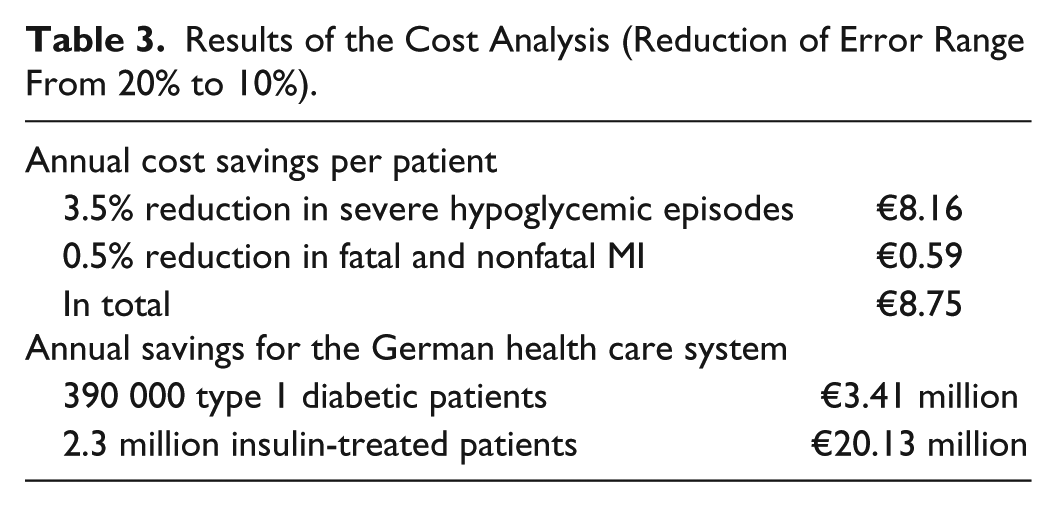
The reduction of the error range from 20% to 10% leads to a HbA1c reduction of 0.28%. 13 According to the UKPDS Risk Engine, this translates into a 0.36% reduction in CHD. 16 A 0.36% reduction in fatal and nonfatal MI translates into savings of €376 057 836 × 0.36% = €676 904 per year or €676 904 / 2.3 million patients = €0.59 per insulin-treated patient per year.
Adding annual savings due to prevented hypoglycemia (€8.16 per patient per year) and MI (€0.59 per patient per year), total savings of €8.75 per patient per year were calculated. Considering the number of 390 000 type 1 diabetic patients in Germany, this will add to potential annual savings of €3.41 million. Analyzing the savings for 2.3 million patients with insulin-treated diabetes the sum will add up to €20.13 million.
Discussion
In the current analysis, we modeled savings for the health care system due to a higher accuracy of SMBG devices in Germany on the basis of a reduction in SMBG error range from 20% to 15% and 10%, respectively.
For the German health care system, the clinical effects translate into potential cost savings of €2.62 and €8.75 (15% and 10% error range) per patient and year. The annual savings due to an improvement from 20% to 15% error range add up to €1.02 million in type 1 diabetic patients and to €6.03 million in the entire group of insulin-treated patients. The annual savings related to an improvement to 10% error range add up to €3.41 million in type 1 diabetic patients and to €20.13 million in the entire group of insulin-treated patients, respectively.
In addition, indirect costs related to reductions of severe hypoglycemic episodes may also need to be considered. In Sweden, indirect costs related to a hospitalization of 6.6 days due to severe hypoglycemia have been calculated as €1110.6 for patients with type 2 diabetes. 18 In the United Kingdom, a mean loss of 3 productive days following a severe hypoglycemic episode has been reported. 19
Recently the clinical and economic implications of accuracy differences among glucose meters have been model for the US health care system. The model predicted an annual difference of approximately 296 000 severe hypoglycemic episodes from BG measurement errors for T1DM (105 000 for T2DM with multiple daily injections) patients for the estimated US population of 958 800 T1DM and 1 353 600 T2DM MDI patients, using the least accurate BGM system versus patients using the most accurate system in a US health care system. This resulted in additional direct costs of approximately $339 million for T1DM and approximately $121 million for T2DM MDI patients per year. 12 Taking a glucose meter with higher accuracy (SD 9.9 mg/dl, mean error −1.0 mg/dl) and a system with lower accuracy (SD 18.2 mg/dl, mean error +2.5 mg/dl) as an example, a difference of 0.31 severe hypoglycemic episodes per patient and year has been modeled. 12
A limitation of the analysis is, that the UKPDS Risk Engine provides an equation for estimating the risk of new coronary heart disease in people with type 2 diabetes, based on data from 4540 UK Prospective Diabetes Study. 16 We decided to apply the risk engine, since an engine for assessing the risk of cardiovascular outcome in type 1 diabetes is currently not available. Also 1 previous in silico analysis 13 focused on type 1 diabetic patients with little or no endogenous insulin production. The application of these patient’s data to type 2 diabetic patients using insulin may also have an impact on the results. Another limitation is that other factors such as errors in carbohydrate counting and varying insulin absorption were not included in the model.
Conclusion
Our model demonstrates that an improvement of accuracy of BG meters from 20% to 15% and 10% may lead to substantial savings for the German health care system by both reducing MI and severe hypoglycemic episodes. Both the current findings and the publication of the new ISO Standard by health care authorities will enforce the development of BG meters with improved accuracy.
Footnotes
Abbreviations
BG, blood glucose; CHD, coronary heart disease; HbA1c, glycosylated hemoglobin; ISO, International Organization for Standardization; MI, myocardial infarction; SMBG, self-monitoring of blood glucose; UKPDS, UK Prospective Diabetes Study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: An unrestricted educational grant of Bayer Health Care was provided to support the editorial needs of this publication. Bayer did not provide statistical support and is not responsible for content.