
Abstract
How do governments address complex, cross-sectoral problems, like the COVID-19 pandemic? Why were some Latin American countries more successful at containing the pandemic's most devastating health outcomes? We argue that national governments that were more collaborative in their response to COVID-19 were more successful in reducing death rates. Our original dataset offers a novel attempt to operationalise collaborative governance (CG). We undertake simple statistical tests to measure the relationship between CG and COVID-19-related mortality rates in Latin America. We then choose three case studies to assess whether collaboration was meaningful in practice. Initial evidence suggests governments that pursued CG were more effective at containing mortality rates early on in the pandemic. The collaboration helped to foster cooperation over resources; buy time to prepare for a potential case surge; and produce a unified message regarding what citizens should do to prevent viral spread.
Introduction
COVID-19 has spread like wildfire across the globe, impacting national health systems, the economy, a country's fiscal solvency, and its social safety nets. Responses to the pandemic vary greatly (Azerrat et al., 2021), as has government capacity to contain its spread. Epidemiological, demographic, and socioeconomic factors cannot fully account for these differences. Political factors, for example, seem to better explain the stringency of government-mandated responses to the pandemic (Bennouna et al., 2020). Policy and politics matter as well for explaining different COVID-19-related outcomes (Greer et al., 2020). Nevertheless, we have yet to understand fully how political factors mitigate the most catastrophic consequences of the pandemic, including widespread death.
In this paper, we argue that how governments choose to address the pandemic matters in terms of staving off the worst health outcomes. We hypothesize that national governments that pursue collaboration when designing containment policies will be more successful in reducing COVID-19-related deaths. A pandemic represents a “wicked” problem. It is “dynamic and complex”; it “ignore[s] the boundaries that shape our public sphere”; and it transcends “governmental, sectoral, jurisdictional, geographic, and even conceptual demarcations” (Emerson and Nabatchi, 2015, p. 7).
Wicked problems are not easily resolved by agents from one level of government, one issue area, or one organisation. Collaboration allows governments to pool resources, knowledge, and experiences from across levels, areas, and organisations. Consequently, policy effectiveness grows. We, therefore, suspect that when collaborative governance (CG) underpins government responses to COVID-19, the worst health impacts of the pandemic will be mitigated.
To test this claim, we build an original dataset that offers a novel attempt to operationalise CG at the country level for large-scale analysis. We then measure the impact of CG on COVID-19-related mortality rates in Latin America. Finally, we examine the cases of Argentina, Brazil, and Uruguay in more detail to identify the potential mechanisms that connect more collaboration to lower COVID-19-related mortality rates.
We find that certain types of collaboration matter. Specifically, collaboration across levels of government and with social organisations yielded policy choices that helped contain COVID-19-related deaths. In the following pages, we develop the theoretical underpinnings of our hypothesis. Next, we describe the research design and provide a first, quantitative examination of the relationship between CG and COVID-19 mortality rates. Finally, we examine three case studies before briefly concluding.
The Role of Collaborative Governance in Pandemic Times
What political factors help explain the widespread differences in COVID-19-related contagion and death rates across countries? Existing research is inconclusive. For example, the relationship between regime type and COVID-19-related mortality rates is unclear. Some found that authoritarian regimes were more successful in reducing death tolls (Cepaluni et al., 2020; Cheibub et al., 2020). Democracies, to quote one study, “experienced deaths sooner and on a larger scale” (Cepaluni et al., 2020, p. 24), likely because their more delegative nature constrained the capacity to respond rapidly (Malesky and London, 2014). Others found no clear relationship. Similar regimes have very different success rates with the virus (González, 2020). Only some authoritarian regimes assert the control necessary to successfully traverse major crises (Shih, 2020).
Democratic quality also has a variable impact. Some institutions and norms associated with democracy, such as greater transparency or less corruption, have a negative relationship with death reduction (Cepaluni et al., 2020). Other institutions, including rule of law, horizontal accountability, or institutionalised party systems, exhibit no clear relationship (González, 2020). Additionally, neither federal nor unitary systems have a clear advantage when it comes to reducing COVID-19 mortality rates (González, 2020; Kincaid and Leckrone, 2020).
The nature of political leadership also does not systematically explain COVID-19 responses. Populists, for example, have a mixed record when it comes to the pandemic. Some populists, like Jair Bolsonaro in Brazil and Donald Trump in the United States, sowed uncertainty and minimised the seriousness of COVID-19 (Lasco, 2020; Smith, 2020). Others, like Andrej Babiš of the Czech Republic and Igor Matovič of Slovakia, preferred to embrace scientific expertise for political gain. Their response was on balance effective, unlike that of Bolsonaro or Trump, even as they further weakened checks and balances (Buštiková and Baboš, 2020).
The negative effects of populism on COVID-19-related outcomes may be tempered by democratic institutions that constrain populist leaders. The most adverse effects of populism during the pandemic have been felt in “the world's less democratic countries” (Cepaluni et al., 2021, p. 4), where checks and balances are inherently weaker or non-existent. Additionally, older democracies are more immune to the negative policy effects of populist leaders than younger ones (Ruth-Lovell et al., 2019). Populist leaders may politicise the pandemic (Lasco, 2020), upending good policy and wreaking havoc on state institutions. 1 Nevertheless, populism alone cannot explain COVID-19-related health outcomes.
Ideology and partisanship do provide explanatory value (González, 2020; Kettl, 2020). Right-wing governments have a higher incidence of COVID-related-deaths per capita than left-wing governments. The former may be reluctant to mandate policies that reduce contagion but hurt the economy. Indeed, left-wing governing parties have better health outcomes than right-wing parties in general (Falkenbach et al., 2020). Nevertheless, the role of ideology is not sufficient for explaining variation in COVID-19 outcomes. For example, some countries experienced dramatic shifts in viral contagion during the same administration. Argentina was a world leader in terms of COVID-19 containment during the first months of the pandemic. By early 2021, however, those numbers had skyrocketed (Bianchi, forthcoming). Yet, the centre-left government of Alberto Fernández remained unchanged.
Additionally, not all right- or left-wing governments are the same. Brazil's right-wing leader, Jair Bolsonaro, has done little to contain viral spread (Melo, 2020). Other right-wing leaders, including Luis Lacalle of Uruguay, have been more successful. 2 Overall, ideology may constrain the range of policy options available to a particular administration. It cannot, however, fully explain the over-time change in one country, or across countries where leaders espouse similar ideological positions.
One potent source of variation with respect to COVID-19-related health outcomes is related to how leaders and governments choose to craft policy. Actors and interests regularly impinge on a government's capacity to deliver goods and guarantee rights to its citizens (Mainwaring and Scully, 2010, p. 1). This is especially true for a pandemic, whose consequences transcend policy areas and impact different sectors of the population in distinct ways.
COVID-19 is a “wicked” problem. It is “dynamic and complex, with no clear definition and no clear solution,” and it “ignore[s] the boundaries that shape our public sphere” (Emerson and Nabatchi, 2015, p. 7). COVID-19 may be “one of the most complex problems that modern governments anywhere have faced” (Kettl, 2020, p. 600). Complex problems defy any single policy response. Nevertheless, they put governance at the forefront of any analysis trying to assess their consequences (Azerrat et al., 2021, p. 147).
Wicked problems, such as COVID-19, demand complex responses that include the input and expertise of multiple actors across different sectors. CG allows for this. CG includes the “processes and structures of public policy decision making and management that engage people across the boundaries of public agencies, levels of government, and/or the public, private, and civic spheres to carry out a public purpose that could not otherwise be accomplished” (Emerson and Nabatchi, 2015, p. 18). CG acknowledges the added value that other actors bring to policymaking. A CG approach deliberately reaches across organisational, sectoral, and jurisdictional boundaries. It privileges multi-actor deliberation and consensus-building (see, e.g. Ansell and Gash, 2008). CG works to “pool” the knowledge base and experiences of different actors, leading to more responsive policies (Bryson et al., 2006, p. 44). 3
CG may be particularly useful in countries, such as many in Latin America, where governments have fewer resources to leverage in the face of an immediate crisis. Where limits on public resources exist, governments often turn to the private and non-profit sectors (Bingham, 2011). CG can promote cooperation, rather than competition, over resources.
Finally, CG may be effective against a pandemic, because it can compel a government to buck the institutional inertia associated with its conventional approach to policy problems. Largely speaking, COVID-19 responses by governments have been “on-path”; they largely reflect how governments typically respond to crises (Bambra et al., 2021). When governments seek out expertise, knowledge, and/or resources through collaboration with others, it can have the (unintended) impact of shifting the Overton Window, or the spectrum of ideas on policy issues considered acceptable by the general public (Lynch, 2020). CG may be a more effective approach at addressing COVID-19-related health outcomes because the policies it produces are more palatable.
CG has potential downsides. The inclusion of more actors can complicate policymaking. More actors mean more veto players, making consensus more difficult. Policies designed collaboratively often take more time (Ansell and Gash, 2008). Yet, a pandemic requires a rapid response. Pandemics are characterised by uncertainty, time pressure, a lack of experience, and “potentially devastating consequences” (Liu et al., 2021, p. 205). Centralised decision-making, therefore, may seem easiest when it comes to crafting responses, especially in the first year (Cepaluni et al., 2020; Schwartz, 2012).
Additionally, the multi-dimensional nature of wicked problems means that policies designed to address one issue may have unexpected negative consequences on another issue (Luke, 1997). Policies create complex feedback effects from which new problems emerge (Senge, 2006). This is true of all policies. Nevertheless, the question of how to effectively collaborate when it comes to interconnected, “wicked” problems remains unanswered (Bryson et al., 2006).
The complexity of a collaborative approach, as well as the time needed to orchestrate the collaboration and then design the policy, may make collaboration prohibitively costly for a government facing a pandemic. A desire to collaborate, and a belief in its results, may not be enough for collaboration to occur. Consequently, in addition to evaluating the impact of collaboration, a worthy empirical question following the COVID-19 outbreak is whether collaboration occurred at all. 4
How do more collaborative governments fare vis-a-vis their less collaborative counterparts when it comes to addressing the COVID-19 pandemic? Early research suggests that collaboration produces better policy outcomes. In Mexico and the United States, governors that worked with each other tended to forge social distancing policies that were more coordinated. Collaboration, in this case, led to greater policy alignment across subnational territories (Bennouna et al., 2020), mitigating contagion across a greater geographic space.
Collaboration with social movements also yields qualitatively distinct outcomes. Where social movements were involved in policymaking, as in Argentina, responses to COVID-19 were designed to think beyond, while also addressing, the short-term needs produced by the pandemic. By contrast, where social movements were excluded, as in Brazil, social movements focused on short-term emergency responses (Abers et al., 2021). The nature and quality of the policies varied as a result of whether the government worked with social movements when crafting its pandemic response.
Overall, there is suggestive evidence that collaboration matters when it comes to shaping policy responses to COVID-19. Nevertheless, this relationship has not been tested systematically. In what follows, we test the following hypothesis:
Research Design
Measuring Collaborative Governance
CG is a concept that has typically been measured qualitatively (Douglas et al., 2020). There are few guideposts regarding how to operationalise the measure. We view CG to be an “umbrella term for myriad cross-boundary, multi-institutional arrangements” (Emerson and Nabatchi, 2015, p. 8), where different stakeholders work toward a common goal, like reducing the spread of COVID-19. Collaboration, consequently, must include at least two actors or stakeholders.
We focus on collaboration that occurs between national government and other actors. In a pandemic, most initial policy responses will emanate from the national government, and especially the executive branch. The executive has the authority and the capacity to quickly design and coordinate policy. Consequently, collaboration early on in the pandemic almost certainly included national government.
Collaboration entails the exploitation of different skillsets and knowledge bases (Ansell and Gash, 2008). Collaborative actors may also have different interests when it comes to the problem at hand. This diversity in terms of skills, knowledge, and interests is what allows for creativity in policy design. Without it, the unique capacity of collaboration is diminished.
Our operationalisation of CG includes the interaction of the national executive with five different stakeholders. Each offers a unique skillset, as well as diverse interests, for addressing a pandemic. For example, inter-governmental CG involves interactions between the national and subnational (local or regional) governments on COVID-19-based policy responses. Subnational governments understand the infrastructural weaknesses and resource challenges of pandemic responses in their constituencies.
Institutional CG includes collaboration among national ministries and/or across national and subnational bureaucracies. These ministries and bureaucracies include technocrats and bureaucrats who have specialised knowledge in policy areas while being attuned to political challenges that public policymaking entails. CG in science and technology occurs between national government and independent experts and scientists. The latter are autonomous from politics and can objectively discuss, for example, the epidemiological, psychological, and economic consequences of particular policy choices. Social CG occurs between national government and social movements and unions – actors who advocate for marginalised groups and can speak to and represent their challenges and demands when considering policy options. Corporate CG occurs between national government and private companies. The private sector has the resources and the connections to offer infrastructural support and fund the research and development for innovative policy solutions.
Given the diversity of knowledge, interests, and skills of these five stakeholders, interactions between the government and each are likely to involve deliberation and debate over which policies should be prioritised and how they should be implemented. To return to Emerson and Nabatchi's definition of CG, interactions with each actor are likely to produce policy responses that “could not otherwise be accomplished” (p. 18). We count these interactions between the national executive and each stakeholder as instances of CG.
For each type of collaboration, we sought to answer a series of questions (see Appendix 1) corresponding to a set of implications that should be observed if collaboration took place. These questions examine whether the national government consulted with each stakeholder on different economic, social, and health policies associated with the pandemic. For example, for inter-governmental CG, we measured whether policy planning and implementation involved meetings between national and subnational governments. We assessed the temporal regularity of those meetings and the representativeness of each level of government. For institutional CG, we coded whether there were formalised instances of policy planning and cooperation among national government ministries (administrative CG) and/or among officials of national and subnational bureaucracies (inter-bureaucratic CG). We also coded whether the meetings included only representatives from the ruling party or also from the opposition.
For CG in science and technology, we explored whether there was policy planning and cooperation with independent health specialists and scientists. For social CG, we evaluated whether there were instances of policy planning and cooperation with representatives of social movements and unions. Finally, for corporate CG, we surveyed whether there were instances of policy planning and/or public–private cooperation mechanisms with private companies.
We coded most questions dichotomously. This means that we cannot get at the degree to which collaboration occurred in any one instance, although a country does score higher if collaboration was regular (vs. infrequent). 5 Nevertheless, we asked multiple questions for each dimension of collaboration. More positive responses across the battery of questions reflect a greater level of collaboration between the national government and a stakeholder. Each country received a separate score for all five types of collaboration. For example, Argentina scored 14 (93 per cent) and Brazil scored 6 (40 per cent) for inter-governmental CG (out of a total of 15, see Table 1).
Cross-Country Levels of Collaborative Governance (CG) Across Different Dimensions.
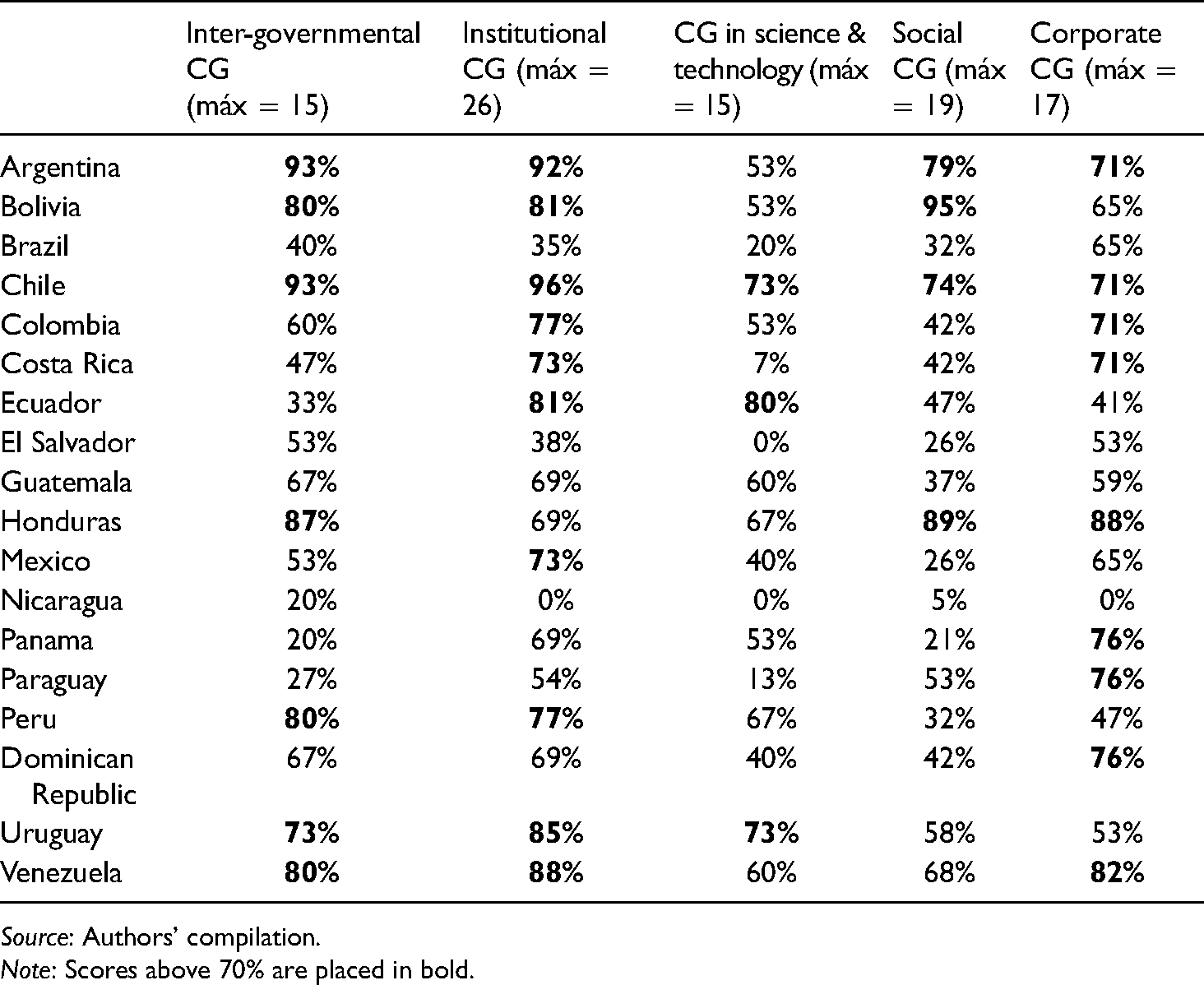
Source: Authors’ compilation.
Note: Scores above 70% are placed in bold.
Newspapers were our primary data-coding source. We selected a minimum of three in each country (see Appendix 1), although when reports were contradictory we included more. We chose newspapers with the highest number of readers but that also varied in terms of their editorial and ideological positions. We triangulated the newspaper data, when necessary, with information from official government sites, academic articles, and experts on each country.
Overall, we collected data on the national executive's collaboration with five different stakeholders during the first year of the pandemic (March 2020–end of January 2021) in eighteen Latin American countries, including Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Dominican Republic, Ecuador, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama, Paraguay, Peru, Uruguay, and Venezuela. Latin America exhibits some of the highest rates of inequality and economic informality in the world. National governments, therefore, faced multiple, daunting tasks when reacting to the pandemic, including accessing and eventually assisting individuals who fall outside of existing social security schemes and government assistance programs (Blofield et al., 2020, pp. 7–8). It is also a region where the government response to COVID-19 has been varied in nature and mixed in terms of effectiveness (Abers et al., 2021; Blofield et al., 2020).
Measuring the Dependent Variable: The Negative Health Impact of COVID
Our dependent variable is the number of COVID-19-based deaths (per million inhabitants) in a country. Specifically, we use per capita mortality data from the end of the first year of the pandemic (January 27, 2021) to ensure that the instances of collaboration, where they occurred, took place before the identified mortality rate.
Our data for the dependent variable are imperfect. Underreporting has likely occurred in many countries. If COVID-19 cases are underreported, then COVID-19-related deaths are likely to be as well. The WHO recommends using excess mortality as an alternative, 6 but these estimates are not available for all cases in our study – a point that restricts their usability in this kind of analysis (Greer et al., 2020).
Our reasons for preferring mortality rates are multiple. For one, containing COVID-19 death rates was a primary goal during the first year of the pandemic and therefore a measure of policy effectiveness. Government authorities used mortality rates early on to plan additional health services and define future policy priorities (Muñoz, 2020). Additionally, COVID-19-based mortality rates vary dramatically across the region. Countries that are quite similar in socio-economic terms exhibit very different rates per one million inhabitants. For example, in December 2020, the cumulative number of COVID-19-based deaths in Argentina and Brazil was 956.8/million and 917.2/million, respectively – roughly eighteen times the rate in Uruguay, at 52.1/million.
Finally, while not perfectly reliable, the total number of deaths per million inhabitants attributed to COVID-19 is one of the best indicators of government performance in addressing the disease (Lau et al., 2021). 7 Overall patterns for this indicator are relatively clear. We see collapsed healthcare systems and mass burials in some countries but not in others (Beech et al., 2020). Even with underestimation, some countries (e.g. the United States, Brazil, and India) experienced far more deaths than others (e.g. Argentina, Canada, or Australia). Finally, underreporting by some countries likely truncates the variation on our dependent variable. Our results may be biased, but they are likely to be biased away from a relationship between CG and mortality rates.
Our approach to measuring CG is also not without limitations. Our data are limited in terms of capturing variation across time. We coded for instances of collaboration at three different times during the first year of the pandemic: at the beginning, during the peak of infections, and in early December 2020. Nevertheless, to maximise variation, we aggregated all of these into a single score per country. Our case studies provide more insight into over-time fluctuation in collaboration, especially in the case of Argentina. Future research should include more information on the dynamics of CG over time.
Second, our data do not capture shifts in collaboration produced by a change in government. In Bolivia, for example, a centre-left government with ties to social movements (Anria, 2018) replaced a conservative, right-wing government. Given these ties, it is possible that the second administration was collaborative in ways that differed from the first. Nevertheless, we coded the case using an average for the period. Finally, we identified at least one clear outlier, Nicaragua, for which obtaining reliable information was a challenge. We excluded it from the statistical analyses, although we maintain it in the descriptive statistics.
Methods
In the following pages, we undertake a novel approach to the study of CG. We rely on data from an original database to undertake pairwise correlations between the different dimensions of CG and COVID-19-based deaths. We also run a Student's t-test between each (dichotomous) question and the number of deaths from COVID-19 per million inhabitants. We compare the average number of deaths in cases where the attribute in question is present with cases in which it is absent.
These statistical tests provide a first cut at assessing the relationship between collaboration and COVID-19-based mortality rates. We have a limited number of cases (18). Therefore, to accompany the quantitative analysis, we undertake three case studies. These help assess the extent to which collaboration, as coded in our dataset, was meaningful in practice. As we show below, the cases of Brazil and Uruguay confirm theoretical expectations. They are good testing grounds for the extent to which the observed correlation actually translates into meaningful collaboration (Lieberman, 2005). A third case, Argentina, appears to contradict theoretical expectations. It scores high on collaboration and also high on per capita mortality rates by the end of the year. A deeper dive into the case demonstrates that changes in collaboration over time bolster, rather than weaken, our quantitative findings. This final case strengthens our results, as it is an apparent deviant case that, upon closer look, ultimately aligns with our hypothesis (Seawright and Gerring, 2008).
To What Extent Does Collaboration Matter? A Quantitative First Look
To analyse the impact of collaboration on COVID-19-based mortality rates, we must first have a sense of how much collaboration there was in Latin America during the first year of the pandemic. We created an overall score of collaboration for each country – what we call a collaborative governance index (CGI). The CGI is the sum total of the dichotomous coding of a battery of questions asked across all five dimensions of collaboration. 8 The maximum possible value of the index (summing up all positive responses) is fifty-five; the minimum is zero. We calculated the Cronbach's alpha statistic to analyse whether the dimensions of the index are related to a single latent theoretical construct. The correlation between all dimensions is 0.86, indicating that these dimensions are related.
Preliminary results suggest that there is quite a bit of variation with respect to the CGI across all cases (Table 2). Several countries show higher values of CG. Chile (46) and Argentina (45), followed by Honduras (43) and Uruguay (43), were the most collaborative in their policy responses to COVID-19. El Salvador, Brazil, and Nicaragua, on the other hand, have the lowest scores. Nicaragua, which represents an outlier in our dataset, received a total score of 1. 9 Overall, Latin American countries varied in terms of how much collaboration they sought with different sorts of actors during the first year of the pandemic.
Collaborative Governance Index.

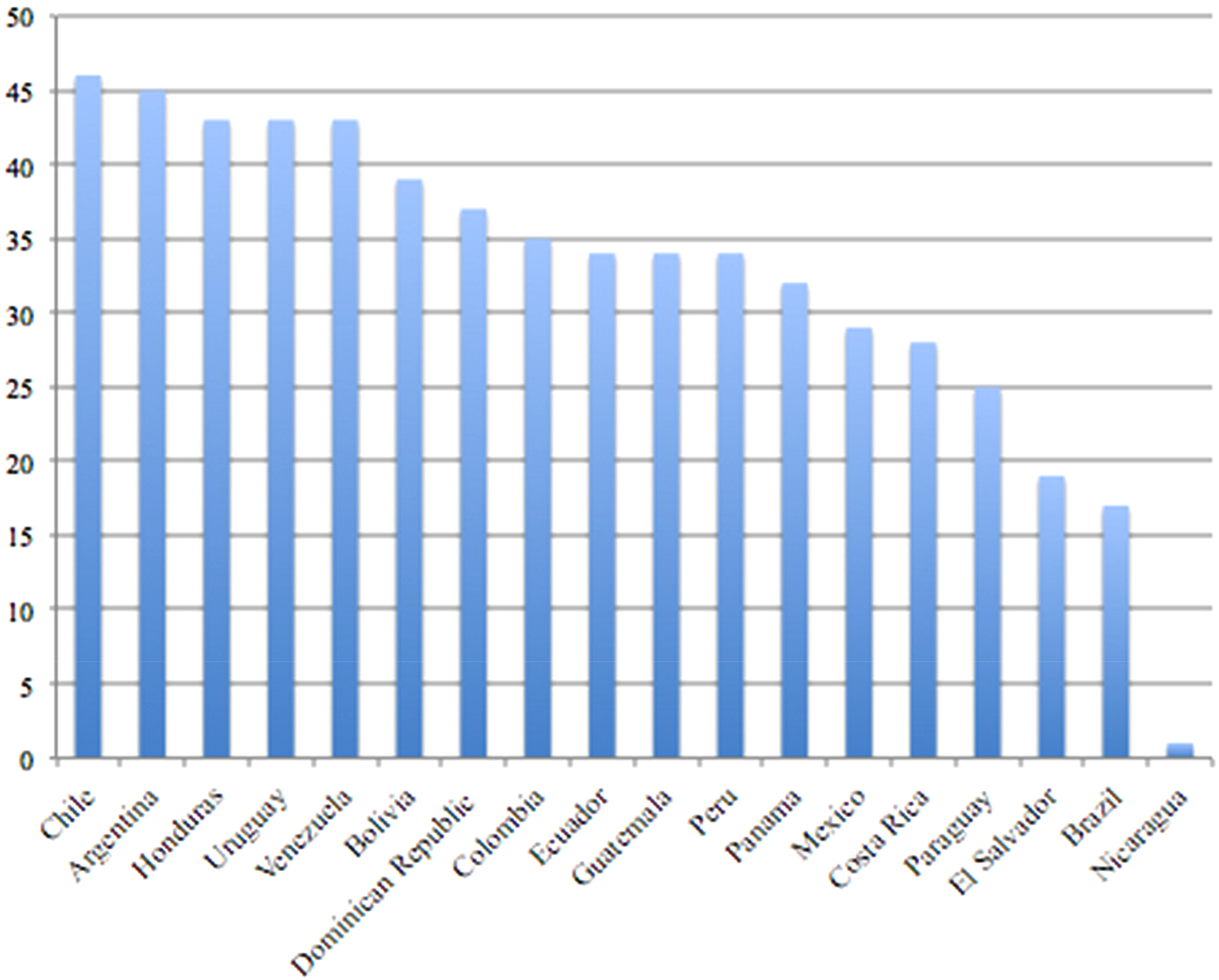
Source: Authors’ compilation.
Note: Maximum possible score is 55.
Table 1 demonstrates how each country fared with respect to each of the five dimensions of collaboration. Here, the maximum score possible for each dimension is based on the number of questions asked about each type of collaboration. 10
Interesting patterns emerge regarding variation across collaboration types. For example, at the most general level, countries tended to score high or low across all dimensions. Many countries scored at 70% or higher (e.g. Argentina, Bolivia, Chile, Honduras, Uruguay), while others never attained that percentage (Brazil, El Salvador, Guatemala, Nicaragua). Corporate CG is an exception to this rule. Countries exhibit relatively high levels of collaboration with the private sector. Ecuador, alternatively, collaborated most with independent scientists and experts. It scored towards the middle or bottom on other dimensions.
There is no clear relationship between different types of governments and collaboration. For example, some federal countries, like Argentina, scored high (14/15, or 93 per cent) in terms of inter-governmental CG – a “natural” choice for collaboration in such a political system. In Mexico and Brazil, by contrast, collaboration with subnational governments was much lower (53 per cent and 40 per cent, respectively). Left-wing and right-wing governments also vary in terms of collaboration. Chile and Argentina pursued the most collaboration (46 and 45, respectively, on the CGI scale). Chile's president, Sebastián Piñera, sits on the centre-right; Argentina's, Alberto Fernández, sits on the centre-left.
The extent of collaboration across these countries is somewhat surprising given the near-universal need, early on in the pandemic, to respond quickly. Collaboration takes time (Ansell and Gash, 2008). These findings also challenge the conclusion that Latin America is a region where, generally speaking, “governance is not sufficiently collaborative and innovative in designing democratically responsible solutions to complex twenty-first-century problems” (Rodriguez, 2019, p. 5). Collaboration is a choice that at least some countries made.
To what extent has collaboration mattered? We hypothesise that, in countries where national governments collaborate more, the negative health impact of COVID-19 should be reduced. As an initial test of this hypothesis, and due to a limited number of cases (18), we produce a scatterplot of cases based on the two key variables (see Figure 1).
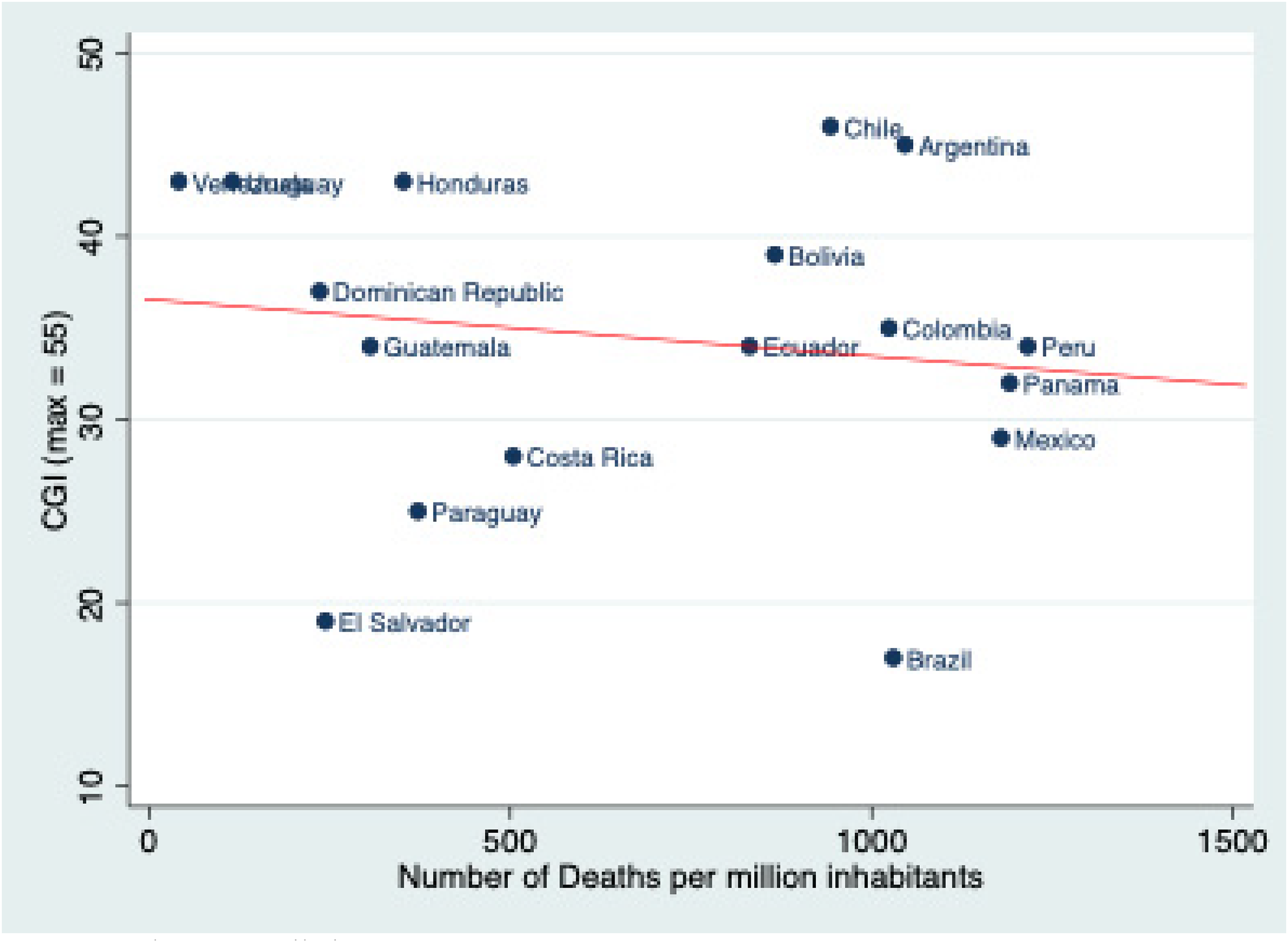
CGI and deaths from COVID-19 (per million inhabitants), eighteen countries. Source: Author's compilation.
Figure 1 presents mixed results. Some countries, such as Uruguay, Honduras, and the Dominican Republic, conform to expectations: They have high values on the CGI with lower COVID-19-related deaths. So, too, does Brazil in the opposite quadrant, with a low CGI score and high death rates. By contrast, Argentina and Chile scored high on the CGI but also experienced high death rates. El Salvador has a low CGI score and also a comparatively low death rate. These results suggest that there is only a weak relationship between the CGI and the number of deaths attributed to COVID-19. 11 The correlation between the variables is low and statistically insignificant, but it is negative (r = −0.10).
Next, we broke down this correlation into the different dimensions of CG. There is no correlation between institutional CG and per capita COVID-based deaths. 12 Nevertheless, t-test results associated with specific policy areas are suggestive. For example, where inter-governmental bureaucracies collaborated on quarantine policy, average death rates were lower than in the absence of collaboration (653/million vs. 1123/million, p = 0.01).
There is no correlation between CG of science and technology and deaths rates either. We do find a negative (r = −0.25) relationship between corporate CG and per capita deaths and between inter-governmental CG and per capita deaths (r = −0.22), but they are not statistically significant (see Figure 2). Nevertheless, the t-test indicates that the number of COVID-19-related deaths/million tends to be lower in countries where there was inter-governmental CG. In these cases, the average number of deaths was 578/million, compared to 857/million where there was no collaboration (p = 0.1). The average number of deaths was also lower when there were regular meetings between officials of the national and sub-national bureaucracies (366/million) versus when there were no meetings (759/million) (p = 0.07).
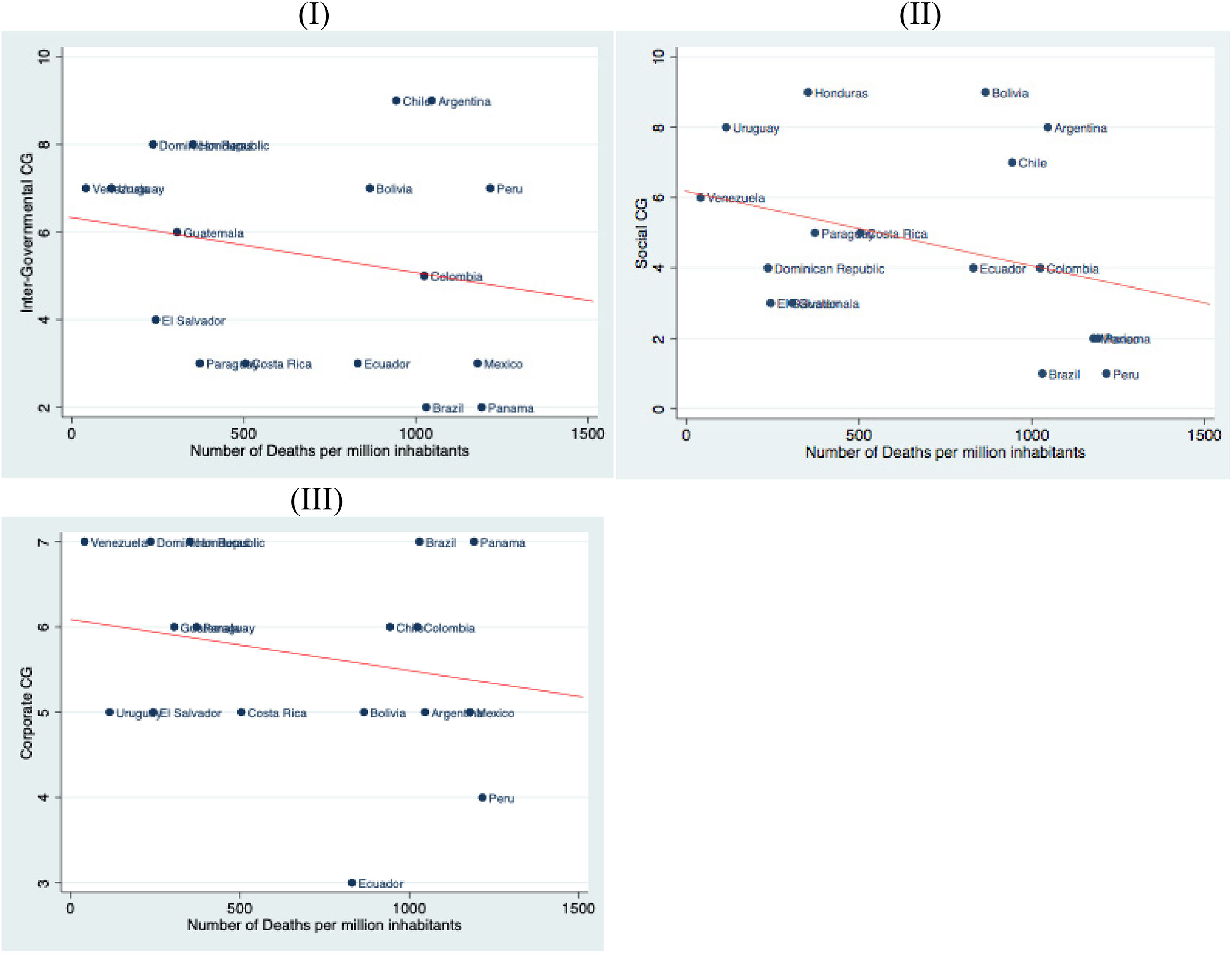
Relationship between COVID-related deaths per million inhabitants and inter-governmental CG (I), social CG (II), and corporate CG (III). Source: Authors’ compilation.
The correlation is stronger and within the upper limits of statistical significance with social CG (r = −0.35; p = 0.1). The t-test appears to confirm that deaths tended to decrease when there was social CG. This was true in the case of collaboration with social organisations (577/million in the presence of collaboration; 788/million in its absence; p = 0.1) and also with unions (575/million with collaboration vs. 1142/million without; p = 0.02). This finding is consistent with existing literature, which finds that social organisations can positively influence government policymaking (Keck and Sikkink, 1998; Andrews, 2001; Soule and Olzak, 2004), including with respect to COVID-19 responses (Abers et al., 2021).
More specifically, when social organisations collaborated on detection, the number of deaths tended to decrease more substantially compared to where there was no collaboration: 336/million on average versus 864/million (p = 0.01). This kind of collaboration occurred in Bolivia, Guatemala, Honduras, Uruguay, and Venezuela. Where social organisations collaborated with vaccine distribution and vaccination, the number of deaths tended to decrease as well: 493/million with collaboration versus 839/million without (p = 0.02). This kind of collaboration occurred in Argentina, Bolivia, Costa Rica, Dominican Republic, Ecuador, Guatemala, Uruguay, and Venezuela. The number of deaths also tended to decrease when there was social collaboration at the beginning (647 vs. 1111; p = 0.08) and at the peak of the pandemic (506 vs. 951; p = 0.02).
Overall, our dataset represents the first attempt to measure collaboration and explore its incidence across a set of countries. We have data on a quite limited number of cases. Gathering information on collaboration is time-consuming and information about it is elusive. Despite these limitations, our measures of CG suggest that there was considerable variation in the countries of the sample. This is an important finding and contributes to our understanding of how governments decide to address a complex problem like the COVID-19 pandemic.
Our initial analyses and their preliminary results also indicate that, where there was more collaboration, the number of deaths attributed to COVID-19 tended to be lower. This was the case, for example, where there were regular meetings between national and subnational government officials. This trend is clearest where there was inter-governmental and social CG. The t-tests confirm that when social organisations collaborated on detection, vaccine distribution, and vaccination, the number of deaths tended to decrease more substantially compared to where there was no collaboration. In all, the data suggest that collaboration can help address the enormous challenges that the pandemic generates. Case studies allow us to examine these findings in more detail.
To What Extent Does Collaboration (Really) Matter? An Examination of Three Cases
Above we found initial evidence of a relationship between collaboration, and especially social and inter-governmental collaboration, and a reduction of COVID-19-related deaths. However, the small number of cases prevented us from controlling for other factors. Additionally, some countries experienced high levels of deaths despite high levels of collaboration.
We carry out brief case studies of Uruguay, Brazil, and Argentina to dig a little deeper into the hypothesised relationship between collaboration and COVID-19-related deaths. In the first year of the pandemic, Uruguay had high levels of collaboration and low death rates (Figure 1). Brazil scored low in terms of collaboration and had much higher death rates. Argentina, by contrast, had one of the highest levels of collaboration but also very high death rates. It is a potentially confounding case that merits further investigation.
High on Collaboration, Low on COVID-19-Related Deaths: The Case of Uruguay
After the first case of COVID-19 was detected in Uruguay, President Luis Lacalle Pou, a conservative president and “fervent believer in personal freedom” (Parks, 2021), instituted a rather severe lockdown (Moreno et al., 2020). The government made confinement voluntary. Nevertheless, 90 per cent of the population complied with the rules and stayed home (BBC News Mundo, 2020).
The lockdown gave the government time to develop a series of technological measures to monitor and control contagion. The resulting system, called Coronavirus.uy, made the country's health services available to citizens via a mobile app. The app helped with tracking, allowed for self-monitoring, and also provided a channel for telemedicine. Uruguay was the first country in Latin America to incorporate exposure notifications (Milano et al., 2020, p. 53).
Collaboration almost certainly had a hand to play in the containment of COVID-19-related deaths in Uruguay. For one, the government worked with the scientific community (Moreno et al., 2020, p. 4) and more than thirty public and private companies to design and implement the software (Milano et al., 2020, p. 54). These stakeholders worked quickly. In the two months following the first detected case, the system was accessed more than 2.6 million times in a country with a total population of 3.5 million people (Milano et al., 2020, p. 54).
The government also developed its own testing kit, allowing Uruguay to outperform other countries on COVID-19 testing. At one point, it had “tested 233.7 people for every confirmed case of COVID-19, compared with 1.7 in Argentina, 1.9 in Mexico, and 3 in Colombia” (Taylor, 2020, p. 1). The kits were created within a COVID-19 diagnostic lab network created in a matter of weeks with the help of research institutes, hospitals, and academic laboratories throughout the country (Taylor, 2020, pp. 1–2).
Overall, CG in science and technology and institutional CG were important to the Uruguayan response early on. This conforms with Table 1, where Uruguay scores high on both dimensions (73 per cent and 85 per cent, respectively). 13 These stakeholders provided expertise, infrastructure, and resources to respond quickly to the pandemic. Indeed, they came together within days of the first identified case. The agreement they forged early on was nearly “perfect” (Taylor, 2020, p. 1), setting the stage for a coordinated response.
Uruguay's early steps in tracking, monitoring, and notification were largely successful. By the end of the year, thanks to the “unprecedented alignment” of decision makers, scientists, and academics, the country had succeeded in reducing the virus’ spread (Anarte, 2020). The total number of COVID-19-related deaths was 52/million. By way of comparison, Argentina had 956 and Brazil had 917 deaths per million (ourworldindata.org). Uruguay's relatively low death rate is especially impressive given that the country has one of the oldest populations in the region – a group that is particularly susceptible to the worst effects of COVID-19 (Saldías, 2020). Overall, many hailed Uruguay as an exceptional success story in Latin America.
Despite this success, a catastrophic surge in COVID-19 cases and deaths emerged in the second year. Why, in April 2021, did Uruguay face a “world-record COVID-19 infection rate” ( Medical Express, 2021 )? Several different factors likely led to the dramatic reversal. First, Uruguay borders Brazil, where one of the more contagious variants of the virus emerged. Second, citizen fatigue with the restrictions of pandemic life undoubtedly set in. Finally, President Lacalle refused to further restrict mobility in light of the growing number of cases, calling instead on personal responsibility. He ignored calls from experts – including some with whom he had collaborated to develop the online health portal (Lissardy, 2021). Rather than continue to collaborate with experts on policy, he deliberately excluded them.
Low on Collaboration, High on COVID-19-Related Deaths: The Case of Brazil
Generally speaking, Brazil's constitutional design is oriented toward promoting federal coordination. This institutional feature should facilitate inter-governmental collaboration. Rather than work with regional and municipal governments, however, President Jair Bolsonaro centralised power (Abrucio et al., 2020). Consequently, when the pandemic hit, the administration's relationship with other governmental stakeholders was “increasingly tense” (Abers et al., 2021, p. 5; Rodrigues and Azevedo, 2020).
The differences between pandemic policymaking in Uruguay and Brazil were stark. In Uruguay, the president worked collaboratively with different stakeholders from the onset of the pandemic. Bolsonaro, by contrast, refused to work with other actors. 14 Inter-institutional conflict, for example, between the national government and other key ministries made addressing the pandemic very difficult. In April 2020, Bolsonaro fired his Health Minister, Luiz Henrique Mandetta. The Minister had recommended that citizens voluntarily quarantine – a measure that specifically contradicted Bolsonaro's message to the public (Rodrigues et al., 2020, p. 628; Kamlot and Santos Vieira de Jesus, 2020). The new minister, Nelson Teich, initially stated that he was aligned with the president (Kamlot and Santos Vieira de Jesus, 2020). Nevertheless, he quit just one month later, in May 2020, after refusing to endorse the use of hydroxychloroquine ( Gazeta do Povo, 2020 ). In line with these events, Brazil has the second-lowest score in Table 1 for institutional CG (35 per cent).
Additionally, rather than collaborate with subnational governments on a coordinated response to COVID-19, Bolsonaro sowed conflict. He called on Brazilians to ignore shutdown mandates emanating from subnational governments and go back to work (Lopes, 2020; Phillips, 2020). In one case, he issued a statement against the self-isolation and business closure measures that governors in Rio de Janeiro and elsewhere mandated. In support of Bolsonaro, the mayor of Rio de Janeiro, Marcelo Crivella, re-opened local business. Immediately following this move, the governor, Wilson Witzel, intervened and reversed Crivella's decision. In the absence of inter-governmental collaboration, mixed messages over the shutdown measures prevailed, sowing confusion amongst the population, who were unsure about whose authority to follow (Rodrigues and Azevedo, 2020, p. 3).
Bolsonaro was adamantly against the more stringent measures of social distancing, the closing of non-essential businesses and schools, and the cancellation of large public gatherings. Nevertheless, Brazil's federal structure gave regional and local governments the authority to issue such measures (Kamlot and Santos Vieira de Jesus, 2020). These were taken by Bolsonaro “as an insurrection against the federal government” (Cheatham, 2020). Eventually, twenty-six out of the twenty-seven Brazilian governors met without the president and agreed on a joint strategy for combating the virus (Kamlot and Santos Vieira de Jesus, 2020).
Ultimately, the national executive chose not to heed the states’ call for stronger actions against COVID-19. Consequently, the states struggled to coordinate their own efforts. For example, without national coordination over the distribution of medical equipment and other resources, states ended up competing over the limited pool of supplies (Abrucio et al., 2020, p. 672). Rather than address inequalities across states, the pandemic exacerbated them.
A “broad-based anti-Bolsonaro coalition from centre-right to left” was formed to protest the president's inaction and also press for change (Abers et al., 2021, p. 8). Unlike in Argentina, as we will see below, these movements were excluded from talks over pandemic policy. Indeed, Bolsonaro's success in sowing doubt over the virus meant that, rather than press for longer-term pandemic solutions, social movements spent their energy convincing citizens that the pandemic actually constituted a threat. Their capacity to demand change, consequently, was limited (Abers et al., 2021).
Overall, Bolsonaro's administration chose not to collaborate with potentially powerful state and non-state actors. Its strategy was one of denial and minimisation in the name of preserving economic growth, and its model of confrontation was strengthened (Abrucio et al., 2020, p. 670). These findings reflect Brazil's performance in Table 1, where it has the fifth-lowest score out of eighteen for inter-governmental CG and social CG, and the second-lowest score on institutional CG and CG in science and technology.
Ultimately, despite a rising number of cases and deaths, state and local governments felt enormous pressure to re-open the economy. In June 2020, most subnational governments began to lift restrictions (Abers et al., 2021, p. 5). By August, the Public Policy Adoption Index of the COVID-19 Observatory at the University of Miami found that Brazil only fared better than Haiti and Nicaragua when it came to fighting the pandemic (Abers et al., 2021, p. 5). Case counts and deaths per million rose exponentially. On June 1, 2020, the number of confirmed cases in Brazil was 2,476 per million. By August 1, it was more than five times higher, at 12,739. Its confirmed number of deaths was 140.8/million on June 1, and nearly three times as great, at 440.7/million, in August. 15
Differences between Uruguay and Brazil in their COVID-19 response were stark in the first year. Uruguay sought out and leveraged the expertise and knowledge of different stakeholders to implement a system to inform citizens about disease testing, tracking, and monitoring. The collaborative effort produced a single (online) site where any Uruguayan could receive information. Bolsonaro's refusal to work with other actors to address the pandemic made enacting successful containment strategies more difficult. States competed, rather than cooperated, over resources. Mixed messages sowed confusion amongst the population. Debates “raged” on social media over whether people should stay home (Kamlot and Santos de Vieira de Jesus, 2020, p. 40). Without the federal government's acknowledgement of the seriousness of the virus, social movements struggled to mobilise support for their demands. Overall, efforts were divided. Containment, as a consequence, was more difficult to achieve.
High on Collaboration, High on COVID-19-Related Deaths: The Case of Argentina
At first glance, Argentina's experience with collaboration directly contradicts our expectations. It is one of the highest performers in terms of CGI, but it has one of the highest death rates in the dataset (Figure 1). Here, we examine Argentina's over-time experience with COVID-19. We show that the government was in fact highly collaborative early on in the first year, when the country's case and death rates were among the lowest in the world. Yet, collaboration – and especially inter-governmental collaboration – broke down several months into the pandemic. By the end of the first year, when we coded mortality rates, deaths had skyrocketed.
Alberto Fernández assumed power just months before the first COVID-19 case was detected. His administration faced debilitating debt, high inflation, and an increasingly polarised political system (Abers et al., 2021, p. 8). Collaboration, and especially inter-governmental collaboration, was not a given. Nevertheless, Fernández chose to work with multiple actors – including scientists, social organisations, and governors – from early on to develop a pandemic response. Part of this response involved utilising existing collaborative institutions and relationships. For example, the executive relied heavily on the Federal Council for Healthcare (COFESA in Spanish), a public agency created in 1981 to: help coordinate public health in the country, design a system for acquiring and distributing medicine and devices, create an online program for identifying and tracing cases, called DetactAr, and coordinate an integrated health database. The most important health measures were decided in collaboration with this institution (Bianchi, forthcoming, p. 7). In line with this finding, Argentina was the second-highest scorer in terms of institutional CG (92 per cent, see Table 1).
The government also turned to scientists and social movements to craft policy. Indeed, these stakeholders had already been incorporated into key government Ministries. Fernández's governing coalition was collaborative in nature. Nevertheless, key social movement leaders, including from the Confederation of Popular Economic Workers (CTEP) and the Mothers of the Plaza de Mayo, gained leverage and influence as the pandemic advanced. They sought to ensure that vulnerable populations could access pandemic-based relief. In harnessing the support of social leaders, the government also mobilised the support of their broader movements, especially for the strict lockdown that was imposed in March 2020 (Abers et al., 2021, pp. 9–10). Social collaboration was integral to the government's initial pandemic response; it is the third-highest performer (79 per cent) on this dimension in Table 1.
Fernández also collaborated with governors and other actors outside of the COFESA framework. For example, his administration, together with the provincial government of Córdoba, negotiated with a company to distribute ventilators domestically rather than export them. The government also worked with the provinces to craft a ventilator distribution plan, so as to “avoid competition among provinces over equipment” (Bianchi, forthcoming, p. 7). Additionally, emergency responses to distribute food, supplies, and protective equipment to the poor were crafted in conjunction with municipal and provincial governments and social movements and organisations (Díaz Langou et al., 2020, p. 19). Collaboration with governors was also important for the country; its score is the highest on this dimension (93 per cent, see Table 1).
Overall, the federal government sought out and collaborated with multiple different actors to address the pandemic early on. The country's collaborative response during the first months of the pandemic gave it time to build hospitals, double the number of beds, and utilise the growing knowledge about the disease to prepare for a potential future spike in cases (Bianchi, forthcoming, p. 2). Collaboration with subnational government was paramount since the country's federal structure gives provinces autonomy over delivering healthcare. As mentioned above, Argentina's case numbers and death rates remained among the lowest in the world during the first months.
The country's federal structure eventually worked against Fernández as the strict lockdown he imposed – with the support of the opposition 16 – neared its fourth month. Given the nature of its federal system, the power of the Argentine presidency is defined in great part by subnational coalitional support (Ardanaz et al., 2014). When that support is lost, a president's capacity to coordinate national policy falters.
This happened towards the end of June when part of the opposition began to openly resist the federal government. Multiple factors likely produced the breakdown in collaboration. For one, early containment may have created a false sense of security amongst the population. 17 A relatively low case count, together with growing citizen fatigue and an economic crisis exacerbated by the lockdown, made consensus over the lockdown increasingly costly for the opposition. Additionally, the government moved to expropriate Vicentín, one of the country's leading agricultural companies that had filed for bankruptcy in late 2019. The stated goal was to rescue the company and protect employees and associated farmers. Opponents publicly condemned the move, drawing parallels with Hugo Chávez in Venezuela (Dube, 2020).
On June 20, 2020, the opposition organised the first of many national protests against the administration. Argentines came out in droves holding signs that said, “Save the Republic,” “Save democracy,” and “No to Argenzuela.” Prominent opposition leaders lambasted the president. By September 2020, the president's support – which had reached 90 per cent in the first month of the pandemic – dropped to just over 50 per cent (Bianchi, forthcoming).
With the breakdown of inter-governmental collaboration and mounting pressure to act, Fernández ended up loosening lockdown restrictions and re-opening the economy. 18 The impact was nearly immediate. Confirmed cases peaked at a weekly average of 333/million in October (on June 1, the weekly average was 15.13 cases/million). Confirmed deaths grew from 12.3/million on June 1 to 958/million by the end of the year (Our World in Data). Nevertheless, the healthcare system was able to absorb the growing caseload. At least through the end of January 2021, and despite having the eleventh highest death rate in the world, Argentine's healthcare system did not collapse (Bianchi, forthcoming).
Overall, the collaboration between the federal government and other stakeholders, and especially governors, shifted quite dramatically roughly four months into the pandemic. Collaboration was high early on. As a result, governors cooperated, rather than competed, over existing resources. Collaboration bought time for the federal government to procure more resources, especially in terms of hospitals and hospital beds. When the surge occurred in the second half of the year, the country was prepared. Nevertheless, cases and deaths surged in the months after collaboration broke down. Rather than confound our hypothesis, Argentina's yearlong battle with the pandemic provides further evidence of the importance of collaboration.
Conclusions
In this paper, we sought to examine the impact collaboration has on COVID-19-related deaths. The quantitative data provided initial, suggestive evidence that collaboration matters for preventing the worst health outcomes. Inter-governmental and social collaboration, in particular, were salient dimensions of collaboration.
The case studies reinforced these findings. Brazil was a negative case of collaboration. The Bolsonaro government excluded social movements and conflicted openly with governors. Consequently, Brazilian states competed for resources; citizens received mixed messages regarding the seriousness of the virus; and social movements struggled to mobilise citizens. The Uruguayan and Argentine governments sought collaboration from the outset. The former leveraged the knowledge and experience of independent scientists and public and private institutions. The latter worked with governors and other state institutions to forge consensus over the imposed lockdown, and it directly incorporated social movements and scientists into its governing coalition. Uruguay and Argentina were successful in containing deaths early on; Brazil, by contrast, struggled. In Argentina, after inter-governmental collaboration broke down, the country's caseload and deaths per capita surged.
We also uncovered mechanisms through which collaboration helped reduce the negative health impacts of COVID-19. Non-state actors in Uruguay and Argentina provided national executives with access to unique expertise and experience. The collaboration allowed governments to pool from other stakeholders the resources they lacked. Collaboration may also have made policies easier to understand. Citizens received mixed messages in Brazil about how to prevent the spread of COVID-19, sowing uncertainty about the proper course of action. Finally, collaboration helped produce policies for sharing, rather than competing, over resources, especially among subnational governments.
Collaboration can be dynamic, as Uruguay and Argentina demonstrate, and there is no reason it must endure. Indeed, Uruguay's president sought collaboration early on in response to the pandemic. When, however, independent experts recommended a stricter lockdown policy, Lacalle chose not to listen. Collaboration may only last to the extent that collaborative mechanisms are institutionalised, so that the whims of any one individual do not supersede broader goals. This point is especially salient in Latin America, where state institutions have historically been politicised.
Finally, we measured the collaborative efforts of national governments in addressing COVID-19. Yet, collaboration need not emanate from the national executive, nor must it necessarily include it. Local government leaders, in collaboration with other local stakeholders, may craft policies that, while more limited in extension, can be effective (Bennouna et al., 2020).
The pandemic rages on in Latin America. Government responses will evolve. Our research suggests that collaboration shaped early responses to COVID-19. But questions about CG remain. Defining the scope, nature, and limitations of collaboration, both for the pandemic as well as for other “wicked” problems in the region, remain fruitful avenues for future research.
Supplemental Material
sj-docx-1-pla-10.1177_1866802X211049250 - Supplemental material for Governing a Pandemic: Assessing the Role of Collaboration on Latin American Responses to the COVID-19 Crisis
Supplemental material, sj-docx-1-pla-10.1177_1866802X211049250 for Governing a Pandemic: Assessing the Role of Collaboration on Latin American Responses to the COVID-19 Crisis by Jennifer Cyr, Matías Bianchi, Lucas González and Antonella Perini in Journal of Politics in Latin America
Footnotes
Acknowledgements
This work emerged from a larger project, Colabora.lat, and the authors thank their fellow collaborators within the project's consortium. The work was carried out with the aid of a grant from the International Development Research Centre, Ottawa, Canada. The views expressed herein do not necessarily represent those of IDRC or its Board of Governors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the International Development Research Centre (Grant no. 109500).
Supplemental Material
Supplemental material for this article is available in online appendices.
Notes
Author Biographies
Appendix 1: Questionnaire Used for Measuring Collaboration across Different Dimensions,as well as Newspaper Sources Used for Coding
In the following pages, we provide a series of tables. Tables 3 and 4 list the questions we used to code levels of collaboration across the five dimensions. Table 5 provides the breakdown of the CGI, and Table 6 provides the score per country. Finally, Table 7 provides a list of all of the newspaper sources utilised to code across the questions in the first tables.
Below is the questionnaire used to measure the extent to which there was collaboration across the five different dimensions of CG. In brief, each dimension refers to the following:
Inter-governmental CG, or collaboration with regional governments and especially the executive office at the regional (i.e. state, province, region) level. Institutional CG, which includes two variants: (a) administrative, or collaboration amongst different national ministries, and (b) inter-bureaucratic, or collaboration across national and subnational bureaucracies. CG in science and technology, or collaboration with independent scientists and health experts. Social CG, or collaboration with social organisations and/or unions. Corporate CG, or collaboration with private enterprise.
The questions in bold were the questions used to create the CGI.
Appendix 2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.