
Abstract
Purpose:
Management of ankle deformity and instability remains a challenge in patients with severe fibular hemimelia (FH). This study aims to evaluate the long-term effectiveness of lateral malleus reconstruction using the fibular anlage in correcting ankle malalignment and preventing the recurrence of deformity following leg lengthening.
Methods:
Ten patients (age: 3.3 years, 0.8–7.7) with a severe FH, equino-valgus foot deformity, ankle instability, and tibial bowing underwent tibia and ankle realignment and lateral malleolus reconstruction. Afterward, all patients underwent tibial lengthening, and the mean lengthening was 9.9 cm (5.0–16.5). Foot and ankle alignment was evaluated clinically and radiographically before surgery, postoperatively, and at a follow-up (10.0 years, 9.2–11.7). Recurrences, additional procedures, and complications were analyzed. Quality of life was assessed using the Limb Deformity-Scoliosis Research Society (LD-SRS) questionnaire.
Results:
At the last follow-up, all patients present neutral heel position or slight valgus (three patients 5° and one patient 10°). No additional procedures were performed except medial malleus temporary epiphysiodesis in two patients. The foot was plantigrade in six patients, presented equinus 10° in two and 20° in two, due to equinus, supra-malleolar osteotomy was performed in three patients. Significant improvement of radiological alignment was found and maintained in all parameters. The mean LD-SRS score was 3.78 at follow-up.
Conclusion:
Lateral malleolus reconstruction provided good clinical, radiological, and functional outcomes. Due to the tendency for recurrence, additional procedures may be necessary.
Level of Evidence:
IV
Introduction
Fibular hemimelia (FH) is the most common longitudinal lower limb deficiency characterized by a spectrum of severity, ranging from mild fibular hypoplasia to complete fibular aplasia.1,2 This condition is associated with progressive leg shortening, hypoplasia of the lateral femoral condyle with valgus knee, and tibial anteromedial bowing (valgus and procurvatum), often accompanied by a skin dimple. 2 The fibula may be partially or absent or present as a distal vestigial fragment, classified as a fibular anlage, which may consist of fibrocartilaginous tissue. 1 The foot deformity observed in severe FH manifests as equinovalgus, though equinovarus may occur less frequently. The etiology of equinovalgus foot deformity includes tibial diaphyseal valgus-procurvatum, maloriented tibial joint surface, lateral wedging of the distal tibial epiphysis, lateral tilt of the talus at the ankle mortise, and malunited subtalar coalition, coupled with the tethering effect of fibular anlage. This condition may also be associated with variable deficits in the foot rays and tarsal coalition, which can lead to restricted hindfoot mobility or, in milder cases, a ball-and-socket ankle joint. The ankle joint may present as horizontal, spherical, or valgus in configuration, but is invariably accompanied by decreased dorsiflexion, with overall joint mobility considerably limited compared to the healthy joint. The presence of a fibular anlage induces lateral tethering. In addition, contracted posterolateral soft tissues and a shortened Achilles tendon contribute to the ongoing progression of valgus deformity and lateral subluxation of the ankle joint.1,3,4
The treatment guidelines emphasize the importance of a comprehensive assessment of foot and ankle morphology to achieve the main goal, which is a plantigrade and functional foot. Subsequently, equal limb length through multiple lengthening procedures that secure normal axis alignment by maturity. In the proposed management of fibular hemimelia, the correction of foot and ankle deformities plays a critical role in the overall treatment outcome.4,5
Different treatment options ranging from the amputation to ankle reconstruction and restoration of a plantigrade foot with various techniques were described for FH treatment. Proposed reconstruction methods included various surgical interventions, including bending tibial osteotomy, 6 fibular remnant excision and buttressing,3,7 free graft buttressing, 8 vascularized fibular head graft, supra-malleolar varus osteotomy, 9 and the SUPERankle procedure. 4 However, middle- or long-term results demonstrating an advantage of one method over another are still lacking.
Objective
This study aims to evaluate the effectiveness of lateral malleus reconstruction using the distal fragment of the fibular anlage in providing ankle alignment and preventing deformity recurrence following leg lengthening in a cohort of patients with severe FH.
Materials and methods
The consecutive 10 patients (five females and five males) diagnosed with severe fibular hemimelia underwent surgical intervention between October 2012 and March 2015. Inclusion criteria were as follows: (1) Severe FH defined as Paley type III—fixed equinovalgus deformity (unable to correct), 4 (2) presence of bony or cartilaginous anlage, (3) procedure of lateral malleus reconstruction using the anlage, and (4) tibial lengthening.
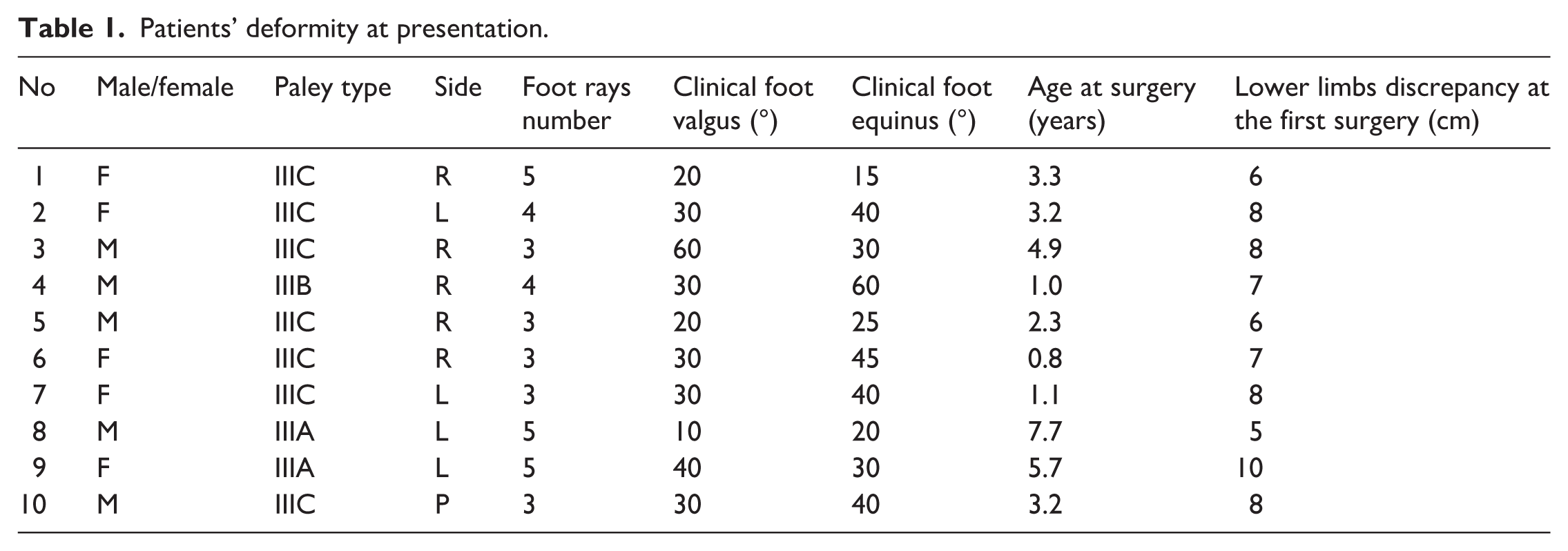
The mean age was 3.3 years (ranging from 0.8 to 7.7 years) at the time of surgery. According to Paley classification, seven patients were type IIIC, one type IIIB, and two type IIIA. Patients’ ankle and foot deformity at presentation are listed in Table 1. Institutional Review Board approval was obtained for this study (No KB—635/23).
Patients’ deformity at presentation.
Surgical technique
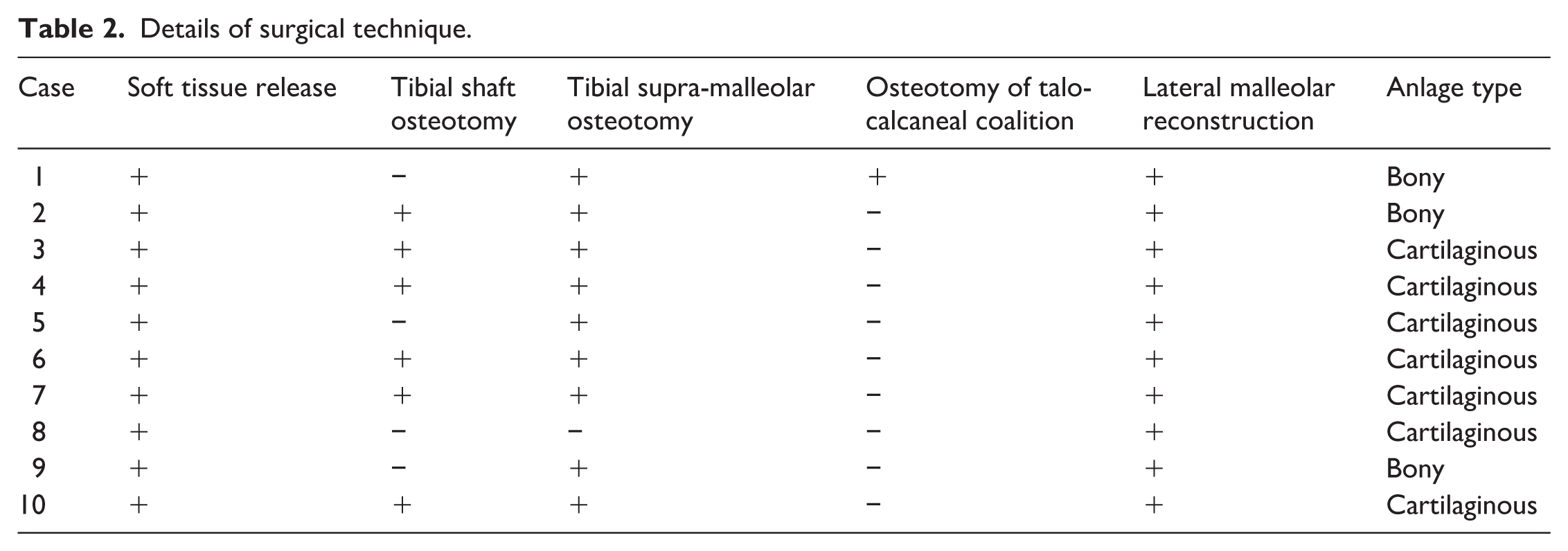
A curved incision was made along the posterolateral aspect of the distal two-thirds of the leg, extending to the sinus tarsi, followed by the elevation of anterior and posterior skin and subcutaneous tissue flaps. Lateral soft tissue release of the ankle joint was performed, and the Achilles and peroneal tendons were lengthened using “Z” plasty. The fibular anlage, including its periosteum or perichondrium, was carefully mobilized from both proximal and distal attachments before excision. Excision of nearly the entire fibular anlage, with preservation of the distal 4–5 cm fibular remnant for lateral malleolus reconstruction. A posterolateral ankle release was performed to achieve proper ankle alignment. In cases of pathological talocalcaneal coalition with abnormal interosseous relationships, an osteotomy of the talocalcaneal coalition was carried out to modify the talocalcaneal orientation. The talus was pinned to the tibia, and the calcaneus was transposed medially and positioned in inversion to realign the calcaneus in line with the talus and the tibia. The foot and ankle were stabilized with one or two transcalcaneal Kirschner wires inserted from the plantar surface of the calcaneus. A supra-malleolar osteotomy was performed to correct a malaligned tibial joint surface, if present, and an additional tibial osteotomy was carried out to address the diaphyseal deformity. Tibial shortening was performed during diaphyseal osteotomy if soft tissue tension did not allow achievement of adequate axial correction. The distal tibial periosteum was dissected from the metaphysis to the level of the distal growth plate, and a space was created for reimplantation of the bony or cartilaginous anlage as a free graft (completely detached with the fibrous part excised). The graft provided lateral support to the ankle joint by fixation to the distal tibia and talus using two transverse smooth K-wires (one K-wire to the epiphysis and one K-wire to the talus; Figures 1 and 2). In addition, the periosteum was sutured between the distal tibia and the fibular anlage, which served as a reconstructed “lateral malleolus” to buttress the talus. The wound was closed in layers, and a posterior above-knee cast was applied for 2 weeks. It was then replaced by an above-knee circular cast for an additional 4 weeks. At 6 weeks after removal of the K-wires, a below-knee walking cast was applied for a further 4 weeks, allowing weight bearing. Physiotherapy, including both passive and active range-of-motion exercises, was initiated immediately after cast removal. An ankle-foot orthosis was subsequently applied to maintain correction (Figure 3). The surgical technique details are described in Table 2.

Surgical dissection of the anlage.
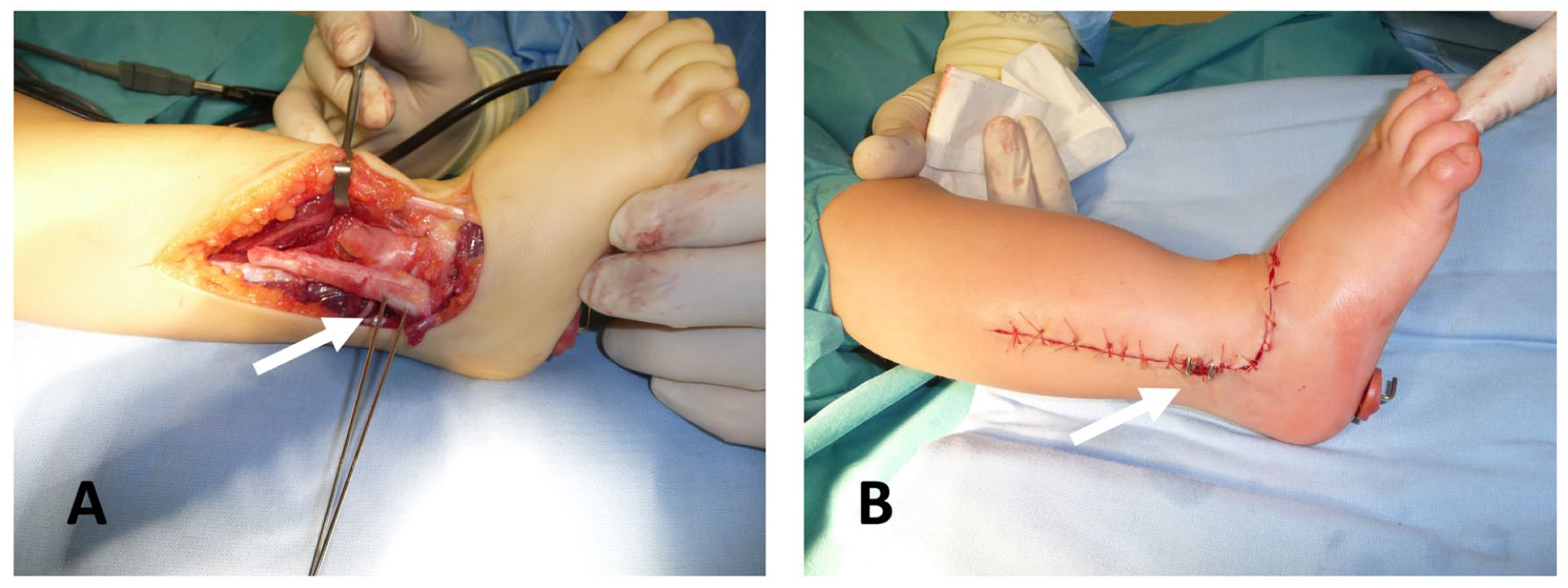
Fixation of the cartilaginous anlage fragment.
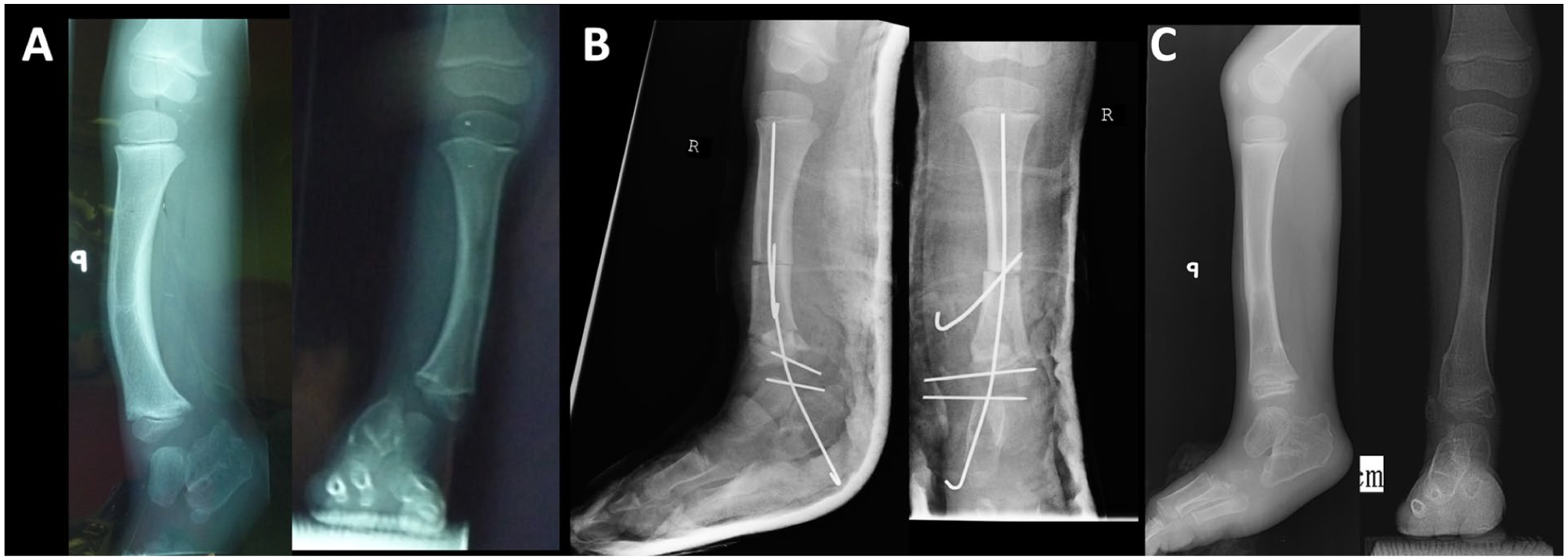
Radiological images of a representative patient.
Details of surgical technique.
Lengthening
Lengthening procedures utilizing circular frame distractors were conducted at least 1 year later and repeated when needed. In each case, the heel stabilization to the frame with two K-wires was performed.
Clinical evaluation
The clinical assessment was performed at follow-up and comprised evaluation of the plantigrade foot position or measurement of the equinus angle, and assessment of the heel valgus angle in a standing position using a goniometer. The ankle joint was defined as mobile when both the dorsal and plantar ranges of motion were greater than 10°.
Recurrence was defined as a clinical equinus or valgus deformity exceeding 10°. Patients who required additional surgery at the level of the distal tibia, ankle joint, or foot due to recurrence during treatment were also included, even if no deformity was present at the final follow-up.
Radiological evaluation
Preoperative and follow-up radiological evaluations were conducted using long-standing, full-length, weight-bearing anteroposterior and lateral radiographs of the entire limb. Early postoperative assessment was performed in a plaster cast using non-weight-bearing radiographs (Figure 3).
The following radiological measurements were performed on anteroposterior radiographs (Figure 4):

Radiological measurements.
Ankle joint position (valgus)—assessed using the mechanical Lateral Distal Tibial Angle (mLDTA), measured between the distal tibial articular surface and the mechanical axis of the tibia. The normal range is 86°–92°, with a mean value of 89°.10,11
Calcaneal position (valgus)—assessed by the mechanical tibiocalcaneal distance, defined as the distance (in millimeters) between the mechanical axis of the tibia and the most distal point of the heel in contact with the ground. 11
Tibial shaft curvature—Coronal Tibial Angle—defined as the angle of deviation of the anatomical axis of the tibia in the coronal plane.11,12
Evaluation of the distal tip of the fibula (anlage) in relation to the tibiotalar joint line in millimeters. Positive value is defined when the tip of the anlage is distal to the joint line, and negative value is defined when the tip of the anlage is proximal to the joint line. 13
The following radiological measurements were performed on the lateral radiographs (Figure 4):
Ankle equinus—measured as the mechanical Anterior Distal Tibial Angle (mADTA), defined as the angle between the mechanical axis of the tibia and the joint orientation line of the ankle in the sagittal plane. The normal range is 78°–82°, with a mean value of 80°.10 –12
Foot equinus—assessed using the mechanical Sagittal Tibio-Calcaneal Angle, defined as the angle between the distal cortical surface of the calcaneus and the mechanical axis of the distal tibial epiphysis. The normal range is 70°–90°, with a mean value of 80°. 11
Tibial shaft curvature—sagittal Tibial Angle, defined as the angle of deviation of the anatomical axis of the tibia in the sagittal plane.11,12
Quality of life evaluation
Patients’ quality of life was assessed during follow-up using the Limb Deformity-Scoliosis Research Society (LD-SRS) questionnaire. This validated instrument comprises 30 items categorized into five domains: function, pain, self-image, mental health, and treatment satisfaction. Answers are scored from 5 to 0. Higher scores indicate a better quality of life. 14
The questionnaires were filled out by patients.
Statistical analysis
Descriptive statistics, including means and standard deviations, were calculated. The normality of data distribution was evaluated using the Kolmogorov–Smirnov test. For variables with a normal distribution, statistical comparisons were performed using repeated-measures ANOVA, with post hoc paired t-test and Bonferroni adjustment applied for multiple comparisons.
In cases of non-normal distribution, medians and interquartile ranges (Q1, Q3) were presented, the Friedman test was employed, followed by post hoc, and the Wilcoxon signed-rank test was used with a Holm correction. A p-value below 0.05 was considered indicative of statistical significance. All analyses were conducted with MedCalc software (version 12.7.8.0).
Results
Lateral malleolus reconstruction was performed in 10 legs of 10 patients with severe FH.
No postoperative infection, bone malunion, or wound healing complications were observed. No patients were lost to follow-up. The follow-up was 10.0 years (9.2–11.7). The age at the last follow-up was 13.3 (10.4–15.0) years.
Patients’ treatment history
All patients underwent subsequent limb lengthening, distributed as follows: three patients underwent a single lengthening procedure, six patients underwent two lengthening procedures (including one patient who required an additional femoral lengthening due to congenital femoral deficiency), and one patient underwent three lengthening procedures. The mean tibial lengthening was 10.0 cm (5.0–16.5 cm), with an average of 5.5 cm (5.0–6.5 cm) per procedure (Table 3). In one patient, tibial and femoral fractures occurred during the lengthening phase after a minor injury.
Number of lengthening and treatment history.
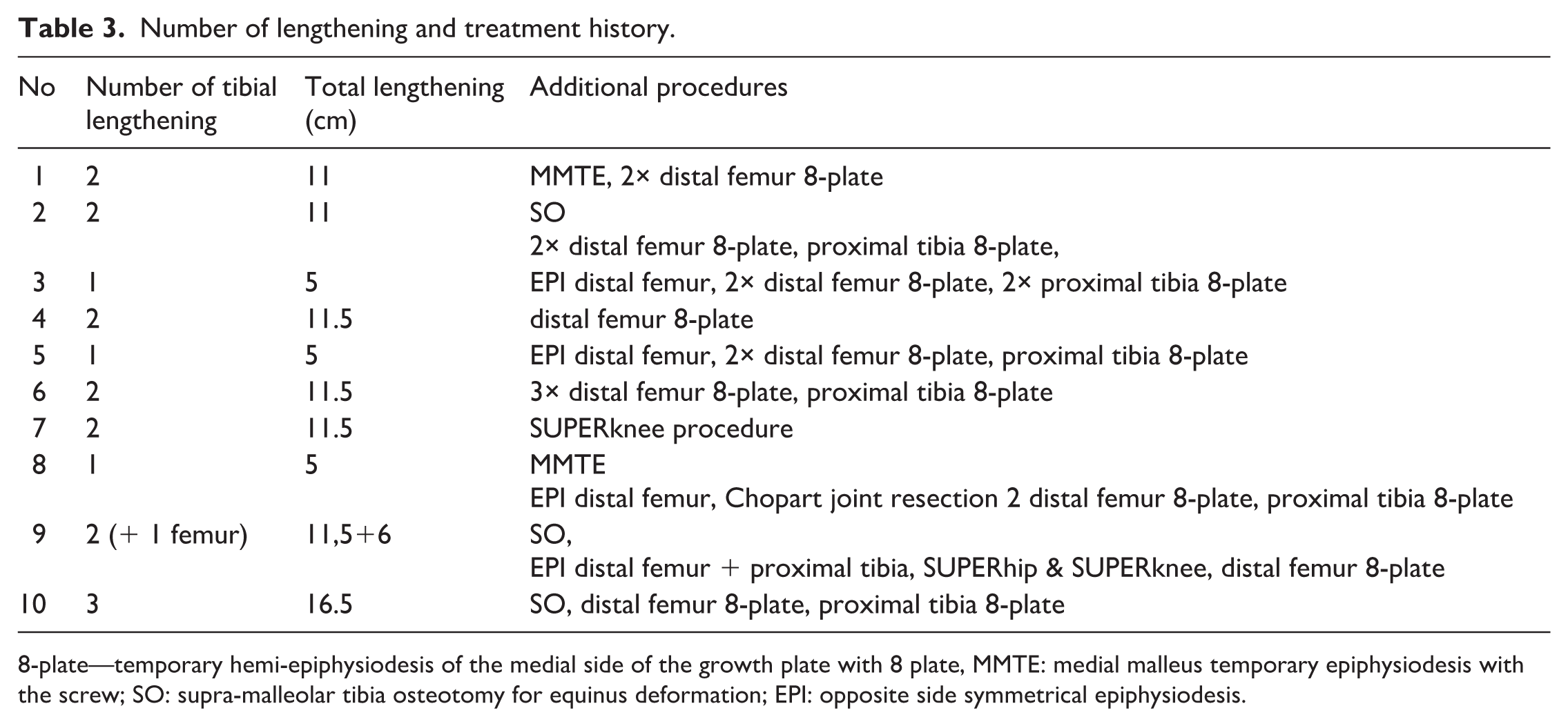
8-plate—temporary hemi-epiphysiodesis of the medial side of the growth plate with 8 plate, MMTE: medial malleus temporary epiphysiodesis with the screw; SO: supra-malleolar tibia osteotomy for equinus deformation; EPI: opposite side symmetrical epiphysiodesis.
Additional procedures concerning the ankle joint during follow-up included the following: (1) correction of recurrent equinus deformity using supra-malleolar tibial osteotomy in three patients. (2) Medial malleus temporary epiphysiodesis with the screw in two patients (Table 3).
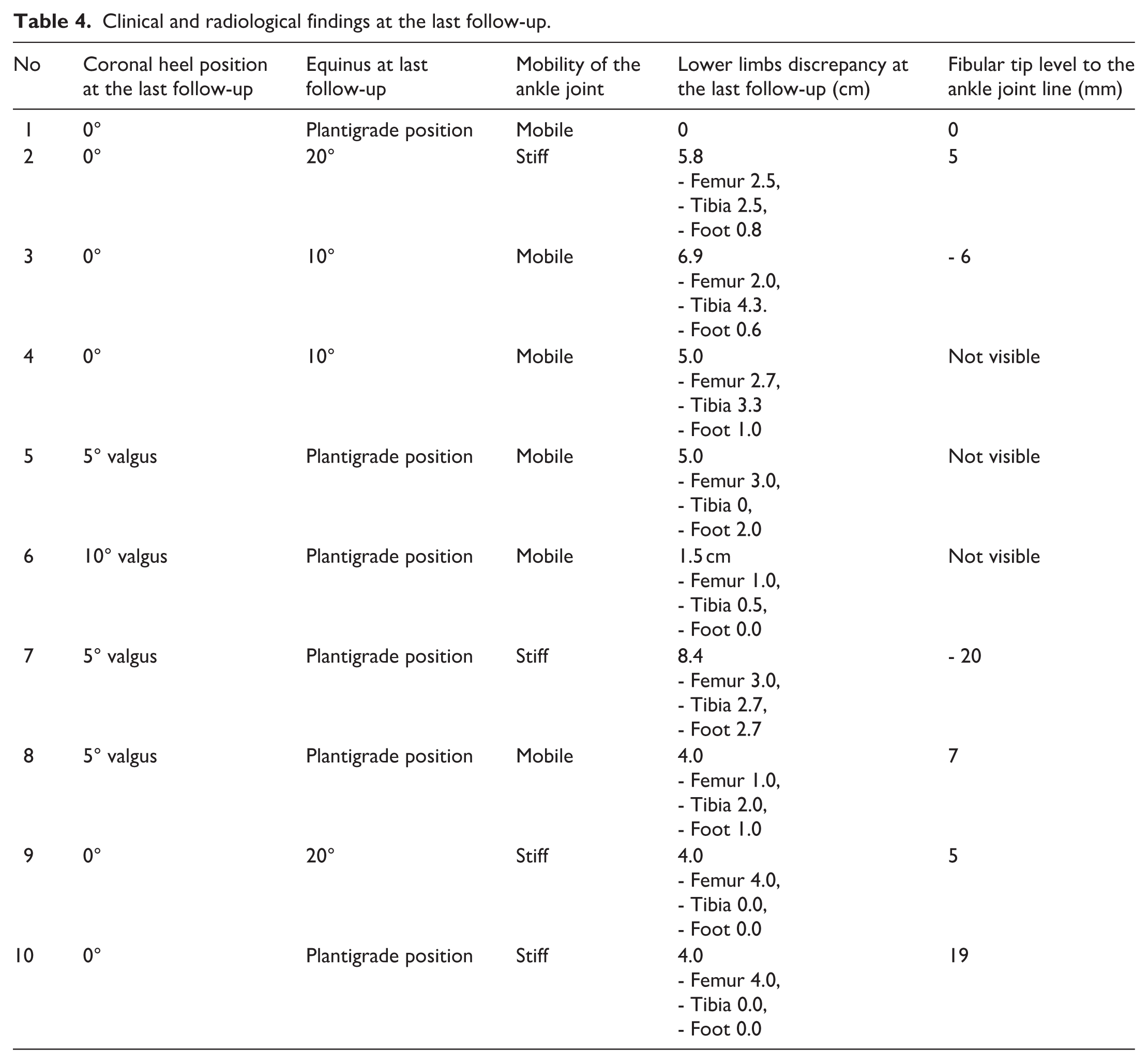
According to our definition, the overall recurrence rate was 50%, including 20% valgus deformity and 30% equinus deformity (Tables 3 and 4). None of the patients required ankle arthrodesis.
Clinical and radiological findings at the last follow-up.
Other additional procedures during follow-up included the following: (1) Correction of knee valgus with temporary hemi-epiphysiodesis of the medial distal growth plate of the femur with eight plate in one patient, one time, in six patients repeated twice, and in three patients three times. (2) Correction of knee valgus with temporary hemi-epiphysiodesis of the medial proximal growth plate of the tibia with eight plate in six patients one time and in one patient repeated twice. (3) Opposite side symmetrical epiphysiodesis of the distal femur four patients and proximal tibia in one. (4) In one patient, an additional foot correction was performed with Chopart joint resection. (5) In one patient, a SUPERknee procedure and in another SUPERhip and SUPERknee procedures (Table 3). Clinical photographs and radiographs of an exemplary patient are presented in Figure 5.

Clinical and radiographic images of a representative patient.
Clinical findings
Clinical findings of the foot and ankle at the last follow-up were as follows: six limbs (60%) presented a clinically plantigrade foot, while four limbs (40%) presented a mild equinus foot up to 20°. In the coronal plane, a neutral heel position was found in six limbs (60%), while four limbs (40%) presented a mild heel valgus up to 10°. The ankle joint was mobile in six limbs (60%) (Table 4).
At the last follow-up, the tibial segment was equal in four patients, and in the remaining six patients, the difference between tibial segments was ≤5.0 cm. The total limb-length discrepancy takes into account both foot height and femoral length and is presented in Table 4.
Radiological findings
The valgus axis of the ankle joint and the calcaneus valgus position were improved, and the correction was maintained at follow-up. The mLDTA was corrected to normal values and during follow-up revealed a tendency to not statistically significant recurrence (Table 5).
Radiological evaluation.
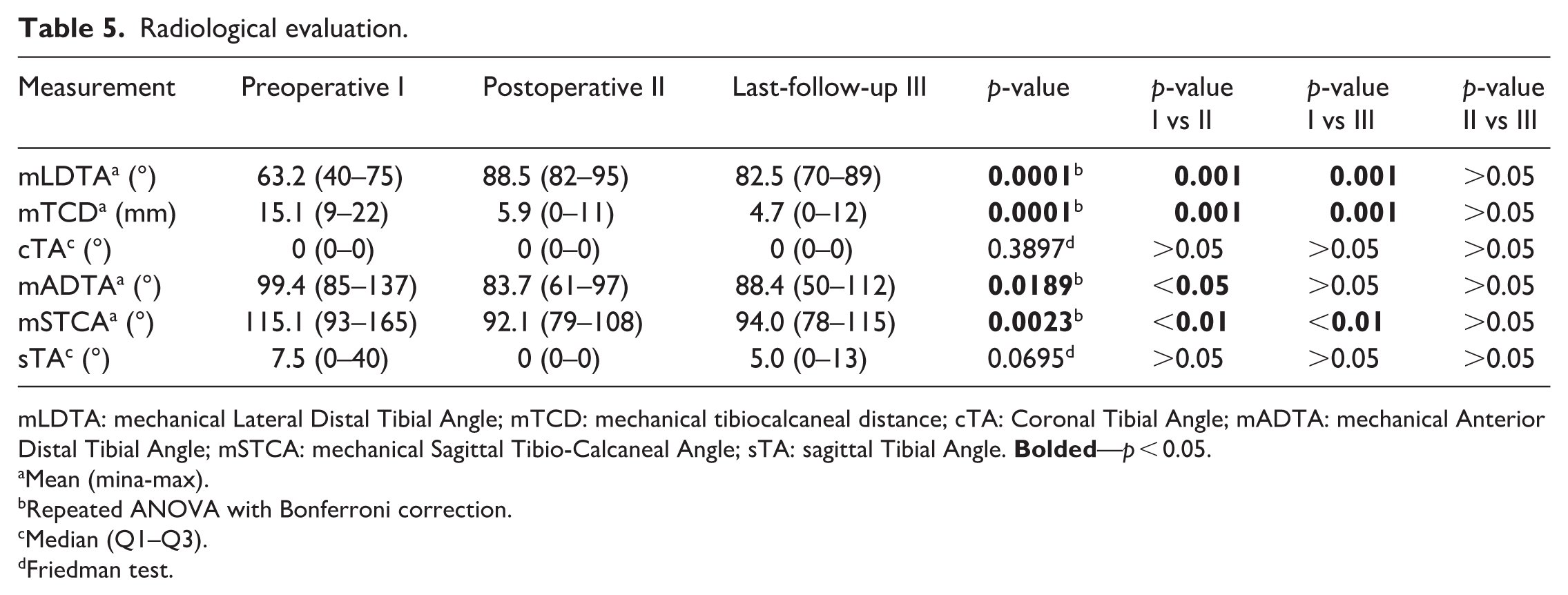
mLDTA: mechanical Lateral Distal Tibial Angle; mTCD: mechanical tibiocalcaneal distance; cTA: Coronal Tibial Angle; mADTA: mechanical Anterior Distal Tibial Angle; mSTCA: mechanical Sagittal Tibio-Calcaneal Angle; sTA: sagittal Tibial Angle.
Mean (mina-max).
Repeated ANOVA with Bonferroni correction.
Median (Q1–Q3).
Friedman test.
The equinus calcaneus position was significantly decreased, and this improvement was maintained at follow-up. The sagittal axis of the ankle joint was improved to the normal value after surgery; it slightly decreased (not significant) at the last follow-up.
Tibia shaft axis in all patients in both coronal and sagittal planes improved (differences not significant).
The ossification of the anlage occurred in 70%. The reconstructed lateral malleolus position in relation to the ankle joint was from 20 mm to −19 mm mean of 1.4 mm. The fibular tip was below the joint line in four patients, at the joint level in one patient, and above the joint line in two patients (Table 4).
Quality of life
The mean LD-SRS score at follow-up was 3.78 (range 3.0–4.60). Domain analysis showed that the best outcome was found in the pain level 4.24 (range 2.55–5.0) with 70% of patients scoring ≥4.
Patients revealed a high level of satisfaction 4.15 (range 2.55–5.0) with 50% of patients scoring ≥4. The mental health score was 3.84 (range 2.8–5.0), and 50% of patients scored ≥4. The function score was 3.62 (range 2.14–4.71), 20% of patients scored ≥4. The lowest ratings were given to the self-image with a score of 3.55 (range: 2.67–4.22), 40% of patients scored ≥4.
Discussion
Severe fibular hemimelia is a complex deformity that necessitates a multi-stage treatment approach and carries a significant risk of recurrence. To achieve better treatment outcomes, it is essential to thoroughly understand the unique characteristics of each deformity and to address all its components effectively. Providing proper orientation of the ankle joint and subtalar alignment is crucial for stable results and successful lengthening.1,4 The absence of the lateral malleolus in fibular hemimelia also leads to subluxation and valgus deformity of the ankle due to the lack of lateral support.2,15 Creating a substitute for the lateral malleolus to support the ankle joint laterally appears logical to enhance its overall stability.
In our study, we found that this surgery achieved correct coronal position in 80% of patients even 10 years after surgery. Two patients required guided growth due to the recurrence of the coronal plane deformity. Radiological data confirmed these findings, demonstrating very satisfactory and stable valgus correction. Although a tendency toward slight recurrence was observed in measurements of the distal tibia and heel position, this did not affect the need for additional procedures or clinical outcomes.
We found a tendency for recurrence of equinus deformity, both at the distal tibia (ADTA) and at the ankle joint. Equinus deformity required corrective osteotomy in three cases (30% recurrence). Among these three patients, two showed further recurrence to 20° at the final follow-up.
Two other studies described the short-term outcome of the reconstruction of the lateral malleolus.3,7
El-Tayeby et al. reported very good treatment outcomes in 13 patients (15 limbs), with no tendency toward recurrence after a mean follow-up of 1.5 years (range, 1–3.1 years). The mean age at surgery was 13 months (range, 9–26 months). 7 Hefny et al. reported results of lateral malleolus reconstruction in eight patients (10 limbs). Nine ankles had a stable plantigrade foot, one ankle had residual equinus, and five ankles had residual valgus heel after a mean follow-up of 4.4 years (range: 4–8 years). The mean age at surgery was 18.9 months (7–36 months). 3 Due to the substantially longer follow-up period of this study (mean 10.0 years), as well as the multiple lengthening procedures performed in our patients, the impact of growth, and the different ages of the children at the time of evaluation, it is difficult to directly compare our study with the previously published studies. Over time, we observed a reduction in range of motion and a tendency toward recurrence in some cases, which suggests that long-term outcomes may differ from short-term reports.
In comparison with the SUPERankle procedure for FH treatment, Shadi et al. 11 found that 42% of patients treated with the SUPERankle procedure had recurrence after a follow-up of 5.2 years (in this group, 5 of the 11 limbs underwent leg lengthening) and required additional procedures to provide a plantigrade foot, including ankle joint arthrodesis in three patients. Kulkarni et al. reported on a larger group of patients with an average follow-up duration of 9.37 years. Among them, 10 patients classified as Paley type III were treated with the SUPERankle procedure and subsequent lengthening. Four of them experienced a recurrence of equinovalgus deformity (40%). 9 When clinically insignificant heel valgus (up to 10°) is considered acceptable, our recurrence rate concerning coronal plane was 20% and concerning the equinus position was 30%, despite the fact that all patients in our study underwent tibial lengthening (three patients once, six patients had double lengthening, and one had triple lengthening). Furthermore, none of our patients required ankle arthrodesis.
The sample size in this study is too small to draw definitive conclusions about which method is superior. However, one key observation is that during long-term follow-up, the risk of recurrence must be carefully considered. This recurrence is primarily influenced not by inadequate correction of the deformity but by the natural history of the condition itself, which is characterized by impaired growth potential. In addition, mechanical forces associated with lengthening procedures can further complicate the situation.
Our results concerning the LD-SRS score were relatively good, with a mean of 3.8. The lowest scores were noted in the self-image domain. As our study did not include a control group, we compared our findings with data available in the literature. To our knowledge, no studies have reported on lateral malleolus reconstruction in relation to LD-SRS questionnaire outcomes. Compared to our results with data published by Shadi et al. for the SUPERankle procedure, they reported a slightly higher total score by 0.2 points and similar slight differences for domain-specific scores: pain (difference of 0.2), satisfaction (0.2), mental health (0.1), and self-image (0.1). The largest difference was observed in the function domain, with a 0.4-point advantage in favor of the SUPERankle group. However, these studies are not directly comparable due to significant differences in follow-up duration and patient age. 11
To avoid recurrence, we have addressed all potential recurrence risk factors. We performed excision of the entire remaining part of the anlage, except for the most distal portion, which was used for lateral malleolus reconstruction. The fibrous anlage tethering the tibia growth and transferring valgus and bending forces during lengthening. This approach is similar to the method described by El-Tayeby 3 and aligns with Paley’s recommendation for its removal. 4 Another reason for the recurrence of the tethering effect of contracted Achilles and peroneal muscle tendons. We performed Achilles and peroneal tendons “Z” plasty, similar to Kulkarni et al., Hefny et al., and El-Tayeby et al.3,7,9 Even after these procedures, the risk of recurrence should be considered, as results of impaired growth potential. The management of the recurrences should be considered in long-term treatment planning.
An interesting issue is the position of the graft in relation to the joint line at the final follow-up. Although a bulky region in the area of the lateral malleolus was found in all patients, ossification occurred in 70% of cases. El-Tayeby and Ahmed 7 found no evidence of ossification of the fibular anlage. Nevertheless, during the follow-up period, physiological tibial growth was observed, and surgical tibial lengthening was performed; proximal migration of the graft was either not detected or minor.
We are aware that the amputation remains a valid option in severe cases of fibular hemimelia, being associated with high patient satisfaction, low complication rates, and minimal hospitalizations. 16 Amputation eliminates the need for repeated surgeries but necessitates lifelong use of a prosthesis, which lacks proprioception and sensory feedback.4,17 The decision is complex and usually based on the family’s acceptance of amputation, as well as social or religious reasons, and is rarely acceptable in our society.
A strength of this study is the relatively long follow-up period and the close monitoring of our patients, including functional evaluation using the LD-SRS questionnaire. A limitation of this study is the small number of patients. It is due to the fact that severe FH is a rare condition. What is more, the other studies concerning the lateral malleus reconstruction study groups were comparable.3,7 Another limitation is that most of our patients have not yet completed their growth. Although half of them are already past the growth spurt, the rest are still growing; therefore, the final evaluation can only be performed once growth is complete. Not all of our patients have equal limb lengths yet. Successful management aims to restore normal weight-bearing and equal limb length.3,4 However, the treatment is not yet complete, and further lengthening is planned. Importantly, in half of the patients, femoral lengthening needs to be considered. A limitation is also the lack of an MRI evaluation of the ankle at the beginning and the end of treatment. Although in 70% of our patients’ anlage grafts ossified, the real shape of the reconstructed lateral malleolus may differ significantly from the ossified part, and in the remaining 30%, the actual position of the reconstructed lateral malleolus could not be measured.
Conclusions
Lateral malleolus reconstruction provided good clinical, radiological, and functional outcomes. However, due to a tendency for recurrence, additional procedures may be required for optimal long-term results.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261432859 – Supplemental material for Lateral malleolus reconstruction for fibular hemimelia as a prevention of foot deformity recurrence following tibial lengthening—A long-term analysis
Supplemental material, sj-pdf-1-cho-10.1177_18632521261432859 for Lateral malleolus reconstruction for fibular hemimelia as a prevention of foot deformity recurrence following tibial lengthening—A long-term analysis by Milud Shadi, Piotr Janusz, Eliza Kortus and Tomasz Kotwicki in Journal of Children's Orthopaedics
Footnotes
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Poznan University of Medical Sciences approved this study. The approval number No KB—635/23. All patients gave informed consent for participation in this study.
Data availability statement
Exact data in anonymized form can be obtained from the corresponding author upon reasonable request.*
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.