
Abstract
Purpose
The study was undertaken to identify the patterns and spectrum of aberrant development of the skeletal elements of the leg and foot in children with pre-axial mirror polydactyly of the foot.
Methods
Case records and radiographs of eight children (ten feet) with pre-axial mirror polydactyly were studied. Four feet were seen in association with fibular dimelia, three feet with dysplastic trapezoid shaped tibia, two with tibial aplasia and one with tibial hypoplasia.
Results
Distinct patterns of anomalies of the hindfoot, midfoot and forefoot were noted, with different patterns of leg malformation. Fibular dimelia was associated with duplication of the calcaneum, cuboid and the lateral cuneiform. Talar duplication occurred in children with a trapezoidal tibia. No duplication of tarsal bones was seen in association with tibial aplasia or hypoplasia. The first metatarsal was hypoplastic wherever the tibia failed to develop. Mere resection of the supernumerary rays resulted in a near normal looking foot in feet without calcaneal duplication. The cosmetic appearance of the foot was poorest in children with fibular dimelia.
Keywords
Introduction
Pre-axial mirror polydactyly of the foot, which is also known as mirror foot or diplopodia, is a very rare congenital anomaly usually associated with major developmental defects of the leg such as fibular dimelia [1–13], tibial aplasia [14–16] or dysplasia [15]. Though reports of fibular dimelia and tibial aplasia mention the association of these anomalies with mirror polydactyly of the foot, little attention has been paid to the foot deformity per se. One reason for this may be that several authors opted to amputate the affected foot or the leg [4, 6, 9] on account of the severity of the associated anomalies of the leg. Over the last 10 years we have encountered ten feet with pre-axial mirror polydactyly in eight children who had a spectrum of associated anomalies of the involved limb.
We studied these children to: (1) describe the spectrum of aberrant development of the skeletal elements in the feet, (2) determine if the patterns of anomalies of the feet are related to the type of anomaly in the leg, and (3) determine if the pattern of different anomalies of the foot has a bearing on treatment planning.
Materials and methods
Feet with supernumerary rays (metatarsals and phalanges) situated pre-axially (i.e., medial to the first ray) but with characteristics of post-axial toes were considered as pre-axial mirror polydactyly. Case records and radiographs of eight children (three boys and five girls) who presented with polydactyly of the feet that met the criteria of mirror duplication as outlined above were reviewed. The age of presentation varied from 9 months to 5 years, and the follow-up ranged between 5 years and 9 months.
The associated anomalies of the leg were documented, and each of the skeletal abnormalities of the digits, the metatarsals, the mid-tarsal region and the hindfoot were carefully noted from the radiographs. An attempt was made to correlate the pattern of foot anomalies with the skeletal anomalies of the leg.
In five of the children, the quadriceps function was good and active knee extension was possible (one child with bilateral tibial aplasia; one child tibial hypoplasia and three children with dysplastic tibiae). In four of these children we opted to reconstruct the limb by choice. The parents of one child refused any treatment. Though the quadriceps function was poor in the remaining three children, we attempted limb reconstruction, since the parents declined amputation. As part of the reconstructive surgery, the supernumerary rays were amputated in each of the feet. No attempt was made to remove the duplicated talus, calcaneum or other tarsal bones if they were present. As the follow-up of these children was not long enough for us to evaluate the overall outcome of the reconstructed limbs, the appearance of the feet alone was assessed.
Results
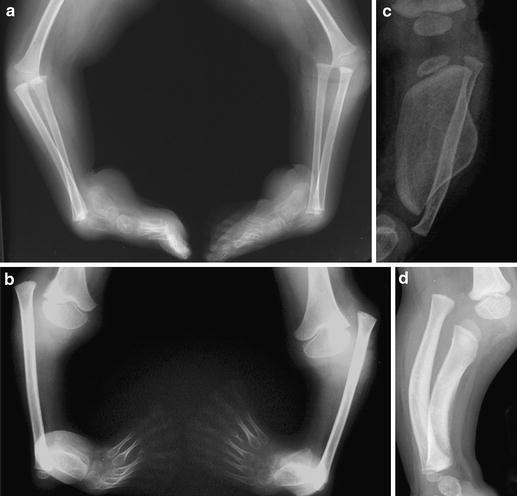
Four patterns of anomalies in the leg were seen in these patients; fibular dimelia in four limbs (Fig. 1 a), total tibial aplasia in two limbs (Fig. 1b), dysplastic tibia with a trapezoidal configuration in three limbs (Fig. 1c) and a hypoplastic tibia in one limb (Fig. 1d).
All the feet were plantarflexed and in varus angulation at the ankle. The varus deformity was predominantly at the ankle joint, and the subtalar joint was not appreciably deformed. The deformity of the ankle was severe in children with fibular dimelia and tibial aplasia (Fig. 2), and much milder in children with a dysplastic trapezoidal tibia. The pattern of anomalies encountered in each foot is shown in Table 1.

Clinical photograph of a child with pre-axial mirror polydactyly. Severe equinovarus deformity, mirror duplication of the toes and a normal-looking heel are seen. The child had tibial aplasia without fibular duplication
Patterns of skeletal malformation seen in the feet and legs of children with pre-axial mirror polydactyly
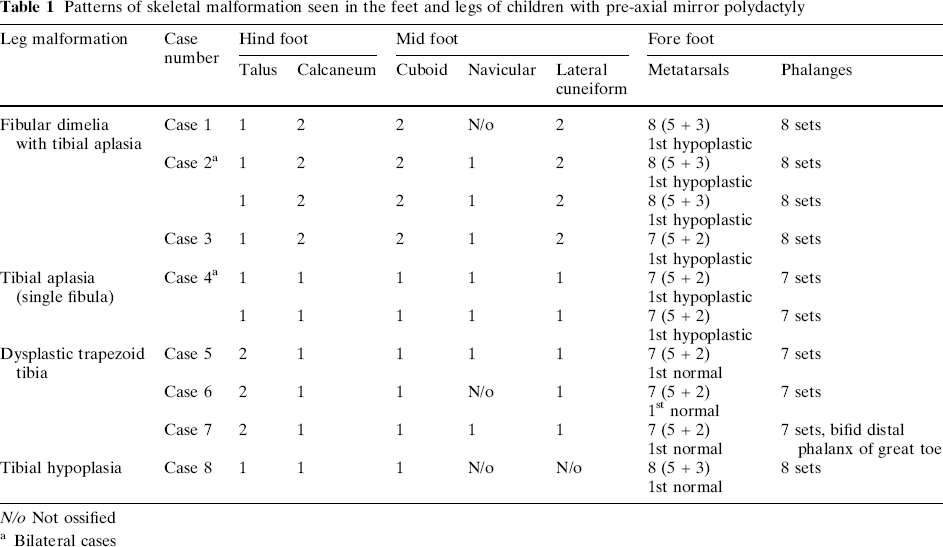
N/o Not ossified
Bilateral cases
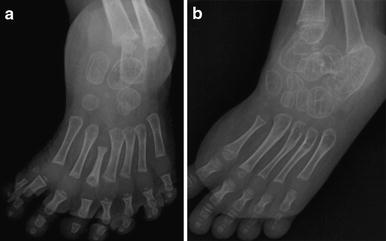
The skeletal elements in the hindfoot were in one of three patterns. In the three feet with tibial aplasia or hypoplasia, there was one talus and one calcaneum (Fig. 3a), in the three feet with dysplastic trapezoidal tibiae the talus was duplicated but there was only a single calcaneum (Fig. 3b), and in the four feet with fibular dimelia there was a single talus with calcaneal duplication (Fig. 3c). In one child with fibular dimelia, the initial radiographic appearance was deceptive, with the duplicated calcaneum looking short and similar to a talus. However the follow-up radiograph clearly showed that both calcanea were of equal size, with a well-formed cuboid articulating with each calcaneum (Fig. 4a, b). There was no suggestion of a synchondrosis or synostosis, either between the two duplicated calcanea or between the calcaneum and the talus, in any of these feet.
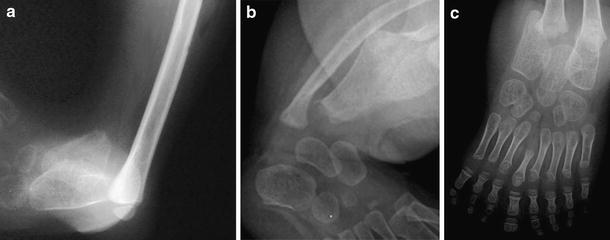
The mid-tarsal pattern also varied depending on the anomalies present in the leg. In patients with tibial aplasia, tibial hypoplasia and tibial dysplasia, no duplication of the midtarsal bones was noted. However, in patients with fibular dimelia, a uniform pattern of duplication of the cuboid and lateral cuneiform was noted (Fig. 3c).
Either two or three supernumerary toes were seen in these ten feet. The first metatarsal was hypoplastic in the feet of all patients with total failure of formation of the tibia. In the four feet associated with a dysplastic tibia or hypoplastic tibia, the first metatarsal was normal. In one patient with fibular dimelia, a rudimentary medial toe without a corresponding metatarsal was noted, and in another patient with dysplastic tibia, a bifid distal phalanx was noted.
Following ablation of supernumerary rays of mirror feet without tarsal duplication, the feet looked virtually normal (Fig. 5); similarly a good cosmetic outcome was seen in feet where only the talus was duplicated. However, the results of just amputating supernumerary rays were poor in patients with a duplicated calcaneum, due to the broad appearance of the foot with a duplicated heel that would persist even if the rays were ablated (Fig. 6).

Post-operative clinical photograph of the foot of the patient with tibial hypoplasia, showing a plantigrade foot with a normal-looking heel

Appearance of pre-axial mirror polydactyly with fibular dimelia. The double heel is clearly seen
Discussion
Definition and nomenclature
There is no universal agreement on what constitutes a mirror foot [17]. While some authors [18] consider mirror foot as any foot with mirror-image polydactyly, others [15] believe that mirror duplication of all the skeletal elements of the foot on the tibial aspect must be present to fulfill the criteria for diagnosing a mirror foot. We suggest that feet with supernumerary rays situated pre-axially (i.e., medial to the first ray) but with characteristics of post-axial toes be considered as mirror feet. We have chosen to avoid including tarsal duplication in the definition since this is very variable, as is evident from the data presented in this report.
With respect to terminology, the descriptive terms ‘mirror foot’ and ‘diplopodia’ do not adequately describe the embryological defect. Diplopodia simply suggests that the foot is duplicated, and the supernumerary toes need not be mirror duplication, as in the case reported by Hamanishi et al. [19]. On the other hand, simply referring to this anomaly as ‘pre-axial polydactyly’ does not convey the unique pattern of duplication, where the pre-axial supernumerary toes show features of post-axial toes. Hence we suggest that this anomaly be referred to as ‘pre-axial mirror polydactyly’, which we believe is sufficiently descriptive and also conveys the nature of the embryological anomaly.
This study reconfirms the earlier observations that pre-axial mirror polydactyly can be associated with fibular dimelia with complete tibial aplasia [1, 2, 6, 7, 9, 11], tibial aplasia without fibular duplication [16], tibial hypoplasia [15, 20] and dysplastic trapezoidal tibia [15].
Patterns of skeletal malformation associated with pre-axial mirror polydactyly
The study also shows that there are distinct patterns of skeletal malformation with pre-axial mirror polydactyly, and that these patterns seem to be related to the type of leg malformation (Table 1).
The foot in children with pre-axial mirror polydactyly and fibular dimelia
Based on earlier reports [1, 2, 6, 7, 9, 11] and data from this study, it is clear that a characteristic pattern of anomalies is seen in feet with pre-axial mirror polydactyly and fibular dimelia. In the hind foot, duplication of the calcaneum is invariably seen, with the characteristic external appearance of a double heel (Fig. 6). Duplication of talus may also occur [6], though this is not a consistent feature.
In the midfoot, duplication of both the cuboid and lateral cuneiform occurs consistently [2, 9]. In anatomical dissection of an amputated limb, Ganey [2] noted the presence of a sixth tarsal bone, which articulated with the five distal tarsal bones including both the cuboids and lateral cuneiforms. He considered this to be an anomalous fusion of the navicular and medial cuneiforms. In one of our patients we too noted a sixth tarsal bone (Fig. 3c) similar to that described by Ganey [2].
In the forefoot, up to four duplicated metatarsals and associated phalanges may occur [9, 16]. The first metatarsal is either hypoplastic or sometimes completely deficient [2]. In patients with fibular dimelia, the ankle is unstable, and gross varus deformity of foot is invariably present.
The foot in children with pre-axial mirror polydactyly and tibial aplasia
Duplication of tarsals of the hindfoot and midfoot is not a feature of feet with pre-axial mirror polydactyly associated with tibial aplasia [15, 16, 20]. The first metatarsal is characteristically hypoplastic in all feet with tibial aplasia. The ankle is unstable, and the varus deformity is severe.
The foot in children with pre-axial mirror polydactyly and tibial dysplasia
Karchinov [15] first noted a dysplastic “trapezoid”-shaped tibia associated with pre-axial mirror polydactyly. The hind foot in patients with this form of tibial dysplasia is characterised by duplication of the talus without duplication of the calcaneum. Karchinov [15] described the presence of an “accessory tarsal bone” articulating medially with the dysplastic tibia. The accessory bone noted by Karchinov may well be the duplicated talus seen in all our patients with dysplastic “trapezoid” tibia. In this form of pre-axial mirror polydactyly, the mid-foot and the first metatarsal are normal.
Patterns of anomalies and treatment planning
The factors that should be taken into consideration while deciding between amputation of the limb and reconstruction in children with these complex anomalies would include: (1) the degree of limb shortening, (2) the integrity and function of the quadriceps mechanism, and (3) the severity of deformity at the knee and ankle. If these factors were favorable for limb reconstruction, we would then need to see how best the appearance of the foot could be improved, since the most unsightly component of the anomalies in these children was the appearance of the foot.
Simple ablation of the supernumerary rays can restore a near normal looking foot when the calcaneum is not duplicated. Hamanishi et al. [19] reported excellent results after excision of a supernumerary foot in a child with diplopodia without deficiency of the tibia. Their surgery included partial excision of the calcaneum, accessory tarsal bones and the extra rays. Similarly, Karchinov [15] emphasized the importance of excising all the duplicated tarsal bones in feet with pre-axial mirror polydactyly. While this may result in a better-looking foot, when calcaneal duplication is present there is a risk of damaging the blood supply to the sole, as the neurovascular structures to the sole would probably run in the plane of dissection between the calcanea.
Another interesting feature that was observed in this study was that normal quadriceps function was present in children with talar duplication and when none of the tarsal bones were duplicated. No active knee extension was present in children with fibular dimelia and calcaneal duplication. It would be interesting to see if this is a consistent association when more such cases are documented in future.
If such an association can be confirmed, we may justifiably recommend amputation in children who have fibular dimelia and calcaneal duplication in association with pre-axial mirror polydactyly, since it would be difficult to obtain a limb that functions well or looks acceptable by reconstructive surgery.
Finally, we acknowledge that concrete recommendations for treatment of these rare anomalies will depend on the long-term outcome of these children assessed at skeletal maturity in terms of knee and ankle function.