
Abstract
Background
The decision to recommend either reconstructive or ablative surgery to the parents of children with fibular hemimelia is difficult and debatable in the orthopaedic literature.
Methods
This is a retrospective study reporting our experience of the treatment of eight children (eight limbs) with fibular hemimelia with limb lengthening using Ilizarov or Taylor spatial frames. All of these children had type 1 or 2a fibular hemimelia (Achterman and Kalamchi). We used the number of rays present in the foot as a guide to decide on the treatment option. Children with more than three rays at the time of presentation were considered for limb reconstruction using Taylor spatial or Ilizarov frames.
Results
All patients were ambulatory and mobile with acceptable leg lengths and limb alignment at the time of last follow-up. All of them were satisfied with the outcome. Knee stiffness was a significant problem in the majority of the patients following lengthening.
Conclusions
We conclude that limb reconstruction in children with less severe forms of fibular hemimelia is a good option.
Introduction
Fibular hemimelia is the most common deficiency of long bones and includes a wide spectrum of congenital anomalies, ranging from mild fibular shortening to complete absence of fibula, and associated defects of the femur, tibia, ankle and foot. It is often associated with shortening of the femur in severe cases. It usually presents clinically as limb length discrepancy, anteromedial bowing of tibia, valgus deformity of the knee, equinovalgus deformities of the foot and ankle, and absent lateral rays [1–3].
The primary aim of treatment is to restore normal limb alignment and length with a stable plantigrade foot for the most effective gait. The two main surgical options for treatment are reconstructive or ablative surgery [4]. In our institution, we have used both of these options and based our decision on the extent of foot deformity present. We advised ablative surgery for patients with less than three rays and reconstructive surgery for patients with more than three rays. The two surgical groups are not comparable and we feel that they should be reviewed separately.
We present our results on reconstructive surgery, using circular external fixators, in children with fibular hemimelia and a functional foot, and introduce the Paediatric Quality of Life Inventory (PedsQL, version 4.0, short form 15)—a validated important paediatric outcome measurement—as a tool and the basis for the assessment of outcome in congenital limb deformities [5].
Materials and methods
A retrospective review was carried out of all children with fibular hemimelia who were treated by limb lengthening at our hospital between the years of 1999 and 2008. The patients were identified through the theatre database and all demographic data, associated congenital anomalies, the pre- and postoperative limb length discrepancy, the type and timing of surgical intervention, and the postoperative complications were obtained from a review of the patient's notes. A final clinical and radiological review was carried out on patients who had attained maturity and were discharged. Patients who were still under clinical follow-up were reviewed at the time of their regular outpatient appointment. The Paediatric Quality of Life Inventory (PedsQL, version 4.0, short form 15)—a validated outcome measure to determine the quality of life in children and patients’ ambulatory status at the time of the last follow-up—was also recorded [5]. This measure includes four main components: physical functioning, emotional functioning, social functioning, and school functioning. All of these components are scored by the children or their parents from 0 to 4, with 0 being the best outcome and 4 being the worst. For the purpose of analysis, the items are reverse scored and linearly transformed to a 0–100 scale, with higher scores indicating better health-related quality of life (0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0). The maximum possible score is 100. The mean (SD) PQLI score in a perfectly healthy child has been reported to be 83 (SD 11.84) [6].
All patients with fibula hemimelia referred to our centre—which is a regional limb reconstruction centre—are referred to the local limb rehabilitation centre, where a comprehensive clinical and radiological assessment is carried out by a multidisciplinary team. The patients also have an opportunity to meet other children and their families with a similar condition. Children with a functional foot were offered reconstructive surgery and those without were offered amputation. We have used the number of rays present in the foot as an indicator of a functional foot. Children with four or five rays were considered to have a functional foot and were offered limb reconstructive surgery, whereas those with one or two rays were considered to have a nonfunctional foot and were offered Syme's amputation. Patients with three rays were considered borderline and were considered for both surgical options; the decision was based on the associated deformities. The parents were also given a choice of lengthening or amputation, and were encouraged to meet other children who have been through the same decision-making process. The Achterman and Kalamchi classification [1] was used to classify these limbs for the purpose of this study, but we did not use it for clinical decision making.
All patients were operated on by the two senior authors or under their direct supervision. All patients received prophylactic intravenous antibiotics at the time of induction. A pneumatic tourniquet was used and inflated only while performing osteotomies. Fibular osteotomy was performed in all type 1 fibular hemimelias through a small lateral incision at the junction of the middle and distal third. A proximal reference wire was inserted just distal to the proximal tibial physis. The frame was constructed mounted onto the reference wire. Further wires and half pins were inserted to attach the frame to the limb. When the Ilizarov frame was used we applied four rings on the tibia, but only two rings in the cases with the Taylor spatial frame (TSF) (Fig. 1). The tibial osteotomy was performed using a small osteotome or a Gigli saw, through small percutaneous incisions. The preferred site for lengthening was the proximal tibial metaphysis. Patients with a diaphyseal deformity underwent correction of the deformity as well as lengthening at the site of the deformity (Fig. 2). Distraction was started 5 days after surgery. All patients had lengthening of the tibia at an average rate of 0.25 mm four times a day. The frame extended to the foot when there was deformity present in the hind foot. Extension to the femur was carried out if the knee was clinically unstable (Fig. 2). When the frame was extended above the knee, the femoral ring was connected to the proximal tibial ring via hinges, allowing supervised knee mobilisation four times every day. Frame extensions above the knee and below the ankle were removed 6 weeks after the end of distraction. Femoral lengthening was carried out in cases with femoral shortening. Intensive supervised active and passive physiotherapy and weight-bearing mobilisation were maintained throughout the period of treatment.
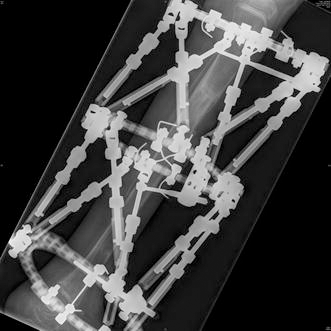
A patient with fibula hemimelia undergoing bifocal lengthening using a Taylor spatial frame
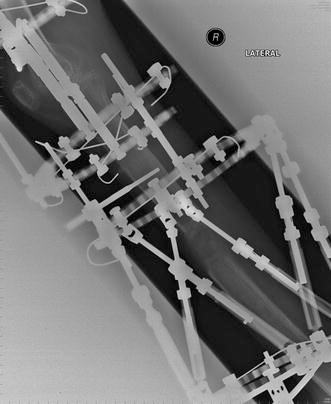
A patient with fibula hemimelia undergoing limb lengthening and mid-shaft deformity correction using a Taylor spatial frame. The frame was extended above the knee because of significant instability
Patients were seen in the outpatient clinic at 2–3 week intervals during the initial period of correction. All patients received standard guidelines for frame care, including pin site care. The maximum lengthening done at a single stage was 5 cm. Once the desired length was achieved, the frame was left in situ for the regenerate to consolidate. Once the consolidation of the regenerate had been achieved clinically and radiologically, the frame was removed. Special attention was paid in these visits to the alignment of the limb and the ranges of motion of the knee, foot and ankle.
Results
Eight patients with fibular hemimelia treated by limb lengthening were included in the study (Table 1). Five of these children had a type 1a deformity and three had a type 2 deformity as per the Achterman and Kalamchi classification [1]. Three children had three rays in their foot, three had four rays, and two had all five rays in the foot. Six of these children had other congenital abnormalities associated with fibular hemimelia. Six were males and two were females. The right leg was involved in five and the left in three children. The mean age at surgery was 8.3 years (range 4–15). The average period of follow-up was 5.4 years (range 1–11). Three of these children required soft tissue surgery including excision of fibular anlage and posterolateral soft tissue release at below 3 years of age in order to achieve centralisation of the foot and to correct the deformity.
Demographic data, associated congenital anomalies, limb length discrepancy (LLD) at latest follow-up, the number of lengthenings and the postoperative complications of all patients with fibula hemimelia who underwent limb reconstruction
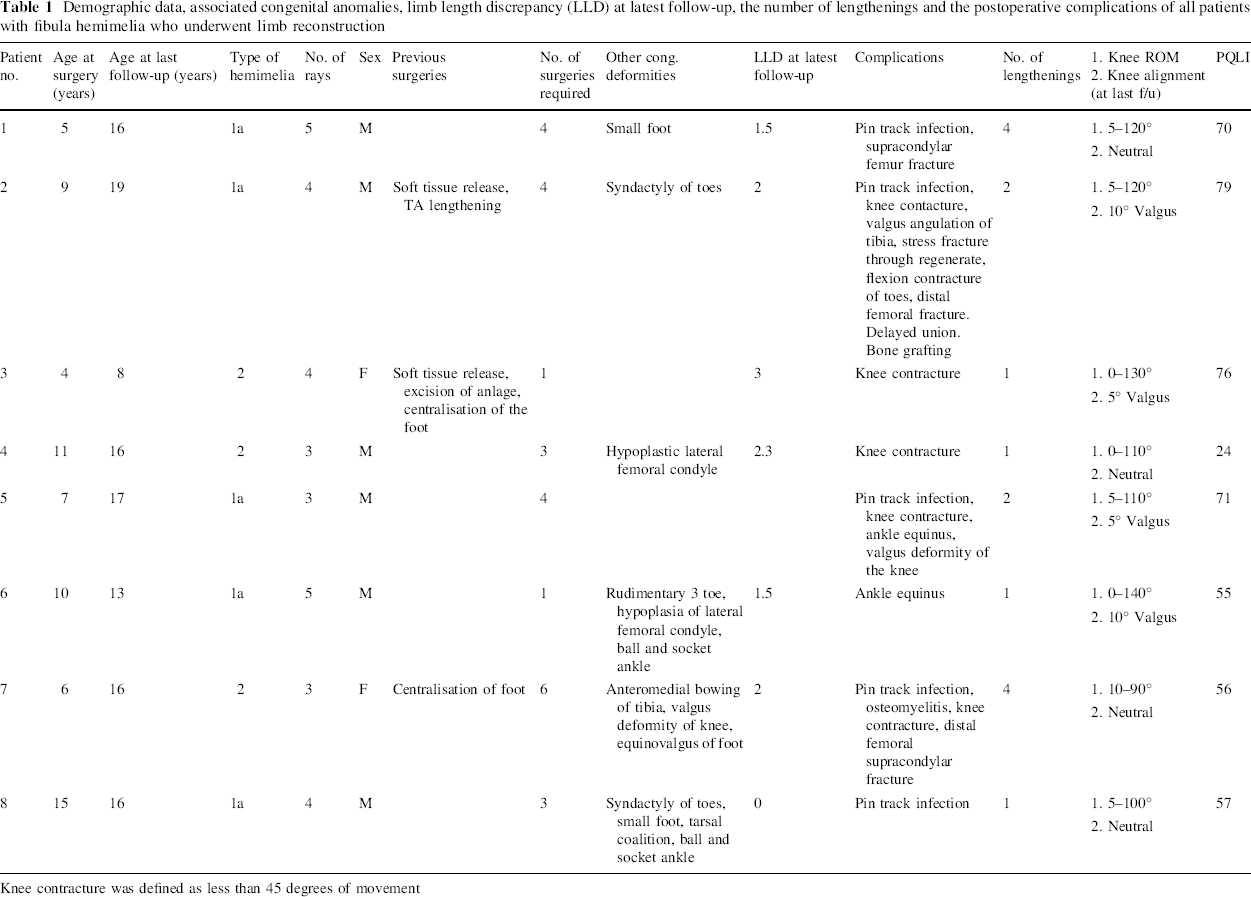
Knee contracture was defined as less than 45 degrees of movement
The mean duration of application of the frame was 7.3 months (range 3.5–19) and the mean lengthening index (total treatment time in months per cm of lengthening) was 1.3 (range 0.55–1.8). One patient required femoral lengthening and the rest had tibial lengthening. Good correction was achieved in all cases. The average limb length discrepancy postcorrection was 0.8 cm (range 0–3). The average number of lengthenings required per patient was 2 (range 1–4). The average number of surgeries performed per patient was 3 (range 1–6).
All patients developed minor complications such as pin track infection, which were treated with antibiotics. Stiffness of the ankle (less than 15° of movement) and knee joints (less than 45° of movement) was seen in six out of the eight patients when the frame was removed, with the knee contractures being more common. The contractures improved with time and intense physiotherapy. At the last follow-up three patients were able to fully extend the knee and the other five had a small degree (up to 10°) of fixed flexion contractures. One patient required bone grafting for delayed union. Three patients sustained a distal femoral fracture during treatment (Fig. 3). Two out of the three fractures occurred after a fall during the frame treatment and were treated with femoral plating. The other supracondylar femoral fracture occurred following a minor injury after frame removal and was treated with a plaster. The other complications encountered are summarised in Table 1.

Long leg X-ray film showing a patient who underwent limb reconstruction for fibula hemimelia. During treatment he sustained a fracture which was treated with femoral plating. His X-rays show almost equal leg lengths but residual valgus deformity
The average age at last follow-up was 15 years (range 8–19), with 6/8 children having reached skeletal maturity at the time of last follow-up. All patients were ambulatory and mobile with acceptable leg lengths and limb alignment at the time of last follow-up. All of them were satisfied with the outcome. The average PQLI (Paediatric Quality of Life Inventory, version 4.0, short form 15) score was 61 (range 23–79).
Discussion
Fibular hemimelia has a wide spectrum of presentations which can range from mild leg length discrepancy to severe deformities of all the segments of the lower limb along with inequalities in leg length of up to 17 cm [7]. It is thus conceivable that there will be more than one strategy for managing this condition. In the past, amputation (both Syme's and Boyd's) was the mainstay of the treatment. Many follow-up studies have shown good functional results with this treatment [2, 8, 9]. This management has its support in the current literature when performed early for severe forms of fibular hemimelia [10, 11].
Early results with Wagner's technique for limb lengthening were disappointing, with a high rate of complications observed [4]. With the introduction of Ilizarov's method of limb lengthening and deformity correction, several centres have reported encouraging results with significant lengthening and preservation of the foot [12, 13]. Of the studies that have attempted to compare amputation and reconstructive surgery, all have suggested that results were better in the amputation group in severe fibular hemimelia as regards to function, complications and number of operations [4, 10, 11]. The main criticism of these studies has been that they were retrospective comparisons of small, unmatched patient populations [14].
In our practice, the two groups—amputation and reconstruction—could not be matched, as the severity of deformity at presentation was quite different in the two groups. So, in this study, we only wanted to look at the results of reconstruction in children who had a functional foot. We feel that severity of foot deformity, particularly the number of rays absent in the foot, is an indicator of the severity of other deformities present in the limb, and we have used this as a guide to decide treatment. Patients with less than three rays in the foot underwent Syme's amputation at a very young age, with all of them below the age of two. Children who underwent limb lengthening had three or more rays and their overall deformities were less severe.
At the time of last follow-up, six of our patients (75%) were skeletally mature and all of them have achieved good alignment of their tibial axis, a functional aligned foot and a residual limb length discrepancy of 2 cm or less. They are managing well, with a small shoe raise if necessary. The remaining two patients have not yet reached skeletal maturity and their progress is being monitored very closely. They are eight and 12 years old with well-aligned feet and limb length discrepancies (LLDs) of 3 and 2 cm, respectively, at the time of last follow-up. Both of these patients had their first stage of lengthening performed and are potential candidates for second-stage lengthening at the time of pubertal growth spurt if there is worsening in their LLD.
All patients in this series underwent tibial lengthening using the Taylor spatial frame, with two patients undergoing first-stage lengthening using the Ilizarov frame. One patient underwent femoral lengthening using the Ilizarov frame. All of the patients had an extension of their frame to the foot during the period of lengthening, and four patients had the frame extended to the femur to stabilise the knee. The decision to extend the frame to the knee was made if there was clinical demonstration of knee laxity or instability on Lachman's or pivot shift or varus/valgus tests. Knee flexion contractures were present in all of these patients and were the most disabling in the long term, often slowing the rehabilitation process. We now feel that extending the frame above the knee should be reserved for truly unstable knees. Knees that demonstrate mild laxity can be treated with a tibial frame that does not extend above the knee, subject to careful monitoring of the knee's range of motion and stability during treatment. This may reduce the incidence of knee stiffness in these patients.
Limb lengthening in fibular hemimelia is associated with a higher incidence of complications, and patients often require multiple surgeries [4, 7, 11, 12]. In our series, the average number of surgeries performed per patient was three. All patients had minor complications from pin track infections that were treated successfully with oral antibiotics alone. One patient developed osteomyelitis, which required surgical drainage along with intravenous antibiotics. Two patients developed valgus angulation of the tibia after first-stage tibial lengthening. This was managed with corrective osteotomy at the time of second stage lengthening and both of them eventually achieved satisfactory limb alignment. Three patients sustained a distal femoral supracondylar fracture during treatment, two of which were treated with plating. This is presumably due to generalised osteopenia as a result of poor mobilisation during treatment. We consider this a significant complication which may require surgical intervention and also interferes with the intense physiotherapy regime the patients go through. Patients are encouraged both pre- and postoperatively to mobilise as much as possible under the close supervision of the physiotherapist in an attempt to reduce the risk of osteopenia and fractures.
We used a patient-centered outcome measure, the Paediatric Quality of Life Inventory (version 4.0, short form 15) to determine final outcome. This is a validated outcome measure to determine quality of life in children that can be applied across all ages in childhood and can be reliably completed by both the children and parents [5, 6]. Children with acute or chronic illnesses have been shown to score lower than healthy children [6]. The PedsQL version 4.0 has not been used as an outcome measure in children with congenital lower limb deformities, and we are hoping to use that as a baseline measure for future assessments in our unit.
We conclude that limb reconstruction using circular frame fixation in children with the less severe forms of the condition is a good option. These children need multiple operations, and success depends on a multidisciplinary approach. The number of rays present in the foot can act as an indicative guide when deciding upon the treatment options. However, a multicentre prospective controlled study is needed to compare the various treatment strategies and their success.