
Abstract
Background:
Osteogenesis imperfecta (OI) is characterized by bone fragility and deformities. Treating long bone fractures and deformities in OI patients typically involves intramedullary (IM) rods. The Simple Locking Intramedullary (SLIM) nail is a novel surgical device developed to address challenges in patients with narrow medullary canals, which are unsuitable for larger telescoping rods. This study aims to evaluate the outcomes and complications associated with SLIM nail use in pediatric patients with OI.
Methods:
A retrospective chart review was conducted at our institution, analyzing 23 patients (41 limbs) who underwent surgery using the SLIM nail between April 2016 and March 2022. Data on patient demographics, surgical intervention, post-operative outcomes, and complications were collected. Radiological evaluations were performed from the immediate post-operative period up to the most recent follow-up.
Results:
The SLIM nail demonstrated a 2-year survival rate of 82.8% and a 4-year survival rate of 77.1% in tibial applications. The most common complication was angular deformity in the distal tibia, occurring in 19 patients. Other complications included anterior cortical penetration, nail bending, and one case of nail breakage.
Conclusions:
The SLIM nail is a viable option for patients with narrow intramedullary canals, particularly in cases where telescoping rods are not feasible. While the SLIM nail provides adequate stabilization and reduces the need for multiple surgeries, careful monitoring is essential to manage complications such as distal angular deformity. Early revision to a larger rod, when possible, is recommended to prevent further complications as the patient grows.
Level of evidence:
Level IV
Introduction
Osteogenesis imperfecta (OI), also known as brittle bone disease, is a rare genetic disease characterized by bone fragility and low bone density, leading to multiple fractures and limb deformities.1,2 Historically, the diagnosis of OI has been based on clinical and radiological features. 3 Pertinent clinical features include fractures from mild trauma, growth deficiency, and bowing deformities of long bone. 1 Skeletal radiographs reveal osteopenia, long bone bowing, undertubulation, metaphyseal flaring, and vertebral compressions. 1 Modern genomics can also be a basis for diagnosis; however, studies show that clinical features, physical exams, and radiological findings have the same sensitivity as biochemical diagnostic testing for identifying children with OI; thus in many institutions, it is not used as a protocol.4,5 Treatment of OI is based on the patient’s age, OI type, and severity of symptoms. Mild cases may only require monitoring, while moderate–severe cases may require a multidisciplinary approach, including medication, physiotherapy, and orthopedic surgery.6 –8 The optimal goals of treatment are improving quality of life, increasing mobility, decreasing bone pain, and decreasing the risk of fractures and deformities.9,10 The most widely used medical intervention for OI is intravenous bisphosphonate therapy, which helps increase bone mineral density and reduce bone turnover.6,11 –13 Surgical realignment and intramedullary (IM) rodding are indicated for recurrent fractures and severe bowing deformities.14,15
Sofield and Millar introduced IM rodding in the mid-20th century, later refined to telescoping rods by Dubow–Bailey.9,16 The telescoping rod revolutionized the treatment of pediatric patients with the concept that as the child grows, the telescoping nail elongates, thereby decreasing the revision rate and associated complications of multiple surgeries.16,17 Now, there are several telescoping rods available commercially. The Fassier–Duval (FD) rod is a self-extending, intramedullary surgical rod that is routinely used at our institution, and globally, to treat children with osteogenesis imperfecta, skeletal dysplasia, and other bone deformities. Some advantages of the FD rod include fewer rates of revision, fewer complications, and more optimal outcomes.18 –21 However, the smallest rod diameter manufactured in this system is 3.2 mm, which is not suitable for smaller bone canal diameters. 15 Thus, pediatric orthopedic surgeons need alternative surgical treatments to help correct bone deformities. To overcome this problem, the Simple Locking Intramedullary (SLIMTM) system was invented. 22
Basic principles and indications of the SLIMTM nail
The SLIM nail is a solid intramedullary nail designed specifically to provide fixation in long bones with small medullary canals that cannot accommodate other larger solid nails (whether telescoping or non-telescoping). Like other intramedullary nails, it operates on the principle of load-sharing, rather than load-bearing, allowing for natural bone stimulation and remodeling, making it especially advantageous in osteopenic bone conditions such as OI.23 –25 Proximal and distal locking options are also available to help control the rotational stability of the fixation (Figure 1). Another advantage is the wide range of diameters (2.0 mm–6.4 mm) and length ranges from 80 mm to 400 mm. The SLIM nail can be inserted into the femur, tibia, humerus, ulna, and fibula and can be used in children, adolescents, and adults of a small stature. 22 The main disadvantage of the SLIM nail is that it is not a telescoping rod, meaning it does not follow the distal bone during growth, allowing distal deformity and fracture to occur.
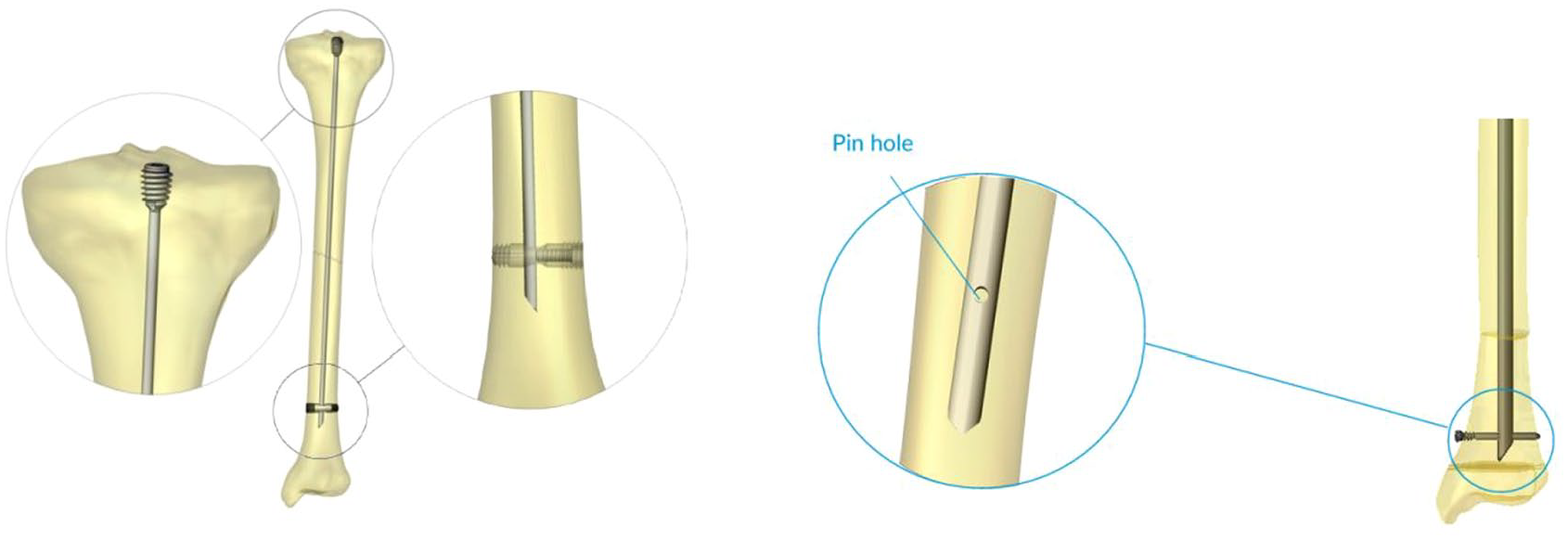
The SLIM nail—a closer look at the proximal threads, distal bullet, and distal pin hole are shown.
The SLIM nail is designed for use in patients with a narrow intramedullary canal, whether they are skeletally immature or mature. For example, while the smallest available diameter for a telescoping FD rod is 3.2 mm, conditions such as osteogenesis imperfecta or skeletal dysplasia may result in intramedullary canals too small for these rods. In these cases, the SLIM nail is indicated to accommodate the unique anatomical challenges. Additionally, as patients approach skeletal maturity, a revision surgery is often required to replace the telescoping rod with a solid rod. In such revision cases, the SLIM nail is indicated as an alternative. The SLIM nail can therefore be indicated for both initial treatment and revision surgeries in skeletally immature or mature patients with narrow intramedullary canals.
The SLIM nail is a relatively new surgical device, and to the best of our knowledge, no reports exist in the literature describing the use of the SLIM nail and its associated outcomes. Hence, a retrospective chart review was conducted to identify, report, and analyze the surgical cases completed at our institution where a SLIM nail has been used. More specifically, we will report our experience with the use of this nail in patients with OI, focusing on the results and complications of the SLIM nail. Our goal is to evaluate if the SLIM nail is a viable option in patients with a narrow intramedullary canal that may not accommodate telescoping rods or larger nails.
Methods
Following ethical approval from the institutional review board (A04-E17-22A), a retrospective study was conducted at a single hospital on 23 patients with a diagnosis of OI for a total of 41 limbs. All patients were operated on using the SLIM Nail (33 tibia, 7 femur, 1 humerus) between April 2016 and March 2022. The minimum follow-up was 2 years. Most SLIM nail operations were on the tibia due to its narrow intramedullary canal. The indications for surgeries in patients with OI are multiple fractures in the same bone (>1), deformity greater than 30 degrees in the coronal or sagittal plane, and the presence of multiple episodes of long bone pain in patients diagnosed with OI with small canal diameters. The vast majority of our patients were ambulatory; however, indications for surgery are the same in non-ambulatory patients.
Data collection
Data extracted from medical records included demographics, medical treatment, radiological data, surgical intervention, post-operative outcomes, and complications. Patient demographics data included age, sex, race, age at surgery, and diagnosis. Medical treatment data pertained to pre-operative and post-operative use of bisphosphonates. Radiological data were collected via the default PACS system (picture archiving and communication system) software using anteroposterior and lateral views of the lower extremities and long films from the immediate post-operative visit until the most recent follow-up visit. Data collected included bone growth distal to the SLIM nail (measured by subtracting the length of the limb between the immediate post-operative X-ray from the most recent one), the presence of angular deformity of the bone, nail deformity, and any cortical break. Surgical intervention data included the diameter of the nail, limb of interest, side of interest, use of plating adjacent to the SLIM nail, survival rate of the nail, number of revision surgeries, cause of revision, and deformity of the nail. Rotational stability was assessed clinically after insertion of the nail with physical exam, if gentle rotation of the bone caused motion at the osteotomy/fracture site. Distal locking was avoided due to the associated risk of complications in skeletally immature patients, and supplementary plating was used when additional rotational control was required. Finally, survival of the nail was calculated by time from index surgery to revision, otherwise until the end of follow-up.
Post-operative protocol and follow-up
After surgery, patients were hospitalized for 2–3 days and discharged in a three-sided slab, maintaining non-weight-bearing status for 6 weeks. A follow-up evaluation, including X-ray imaging, was performed at 6 weeks. If evidence of healing was observed and the patient was progressing clinically, they were transitioned to a KAFO (knee-ankle-foot orthosis) and allowed gradual progression from partial to full weight bearing. If there was no radiographic evidence of healing at 6 weeks, non-weight bearing was continued for an additional 4 weeks. A second follow-up with additional X-rays was then conducted at approximately 10 weeks. If healing was satisfactory, patients were re-evaluated at 3 months with repeat X-rays, followed by imaging every 6 months, and then annually thereafter.
Results
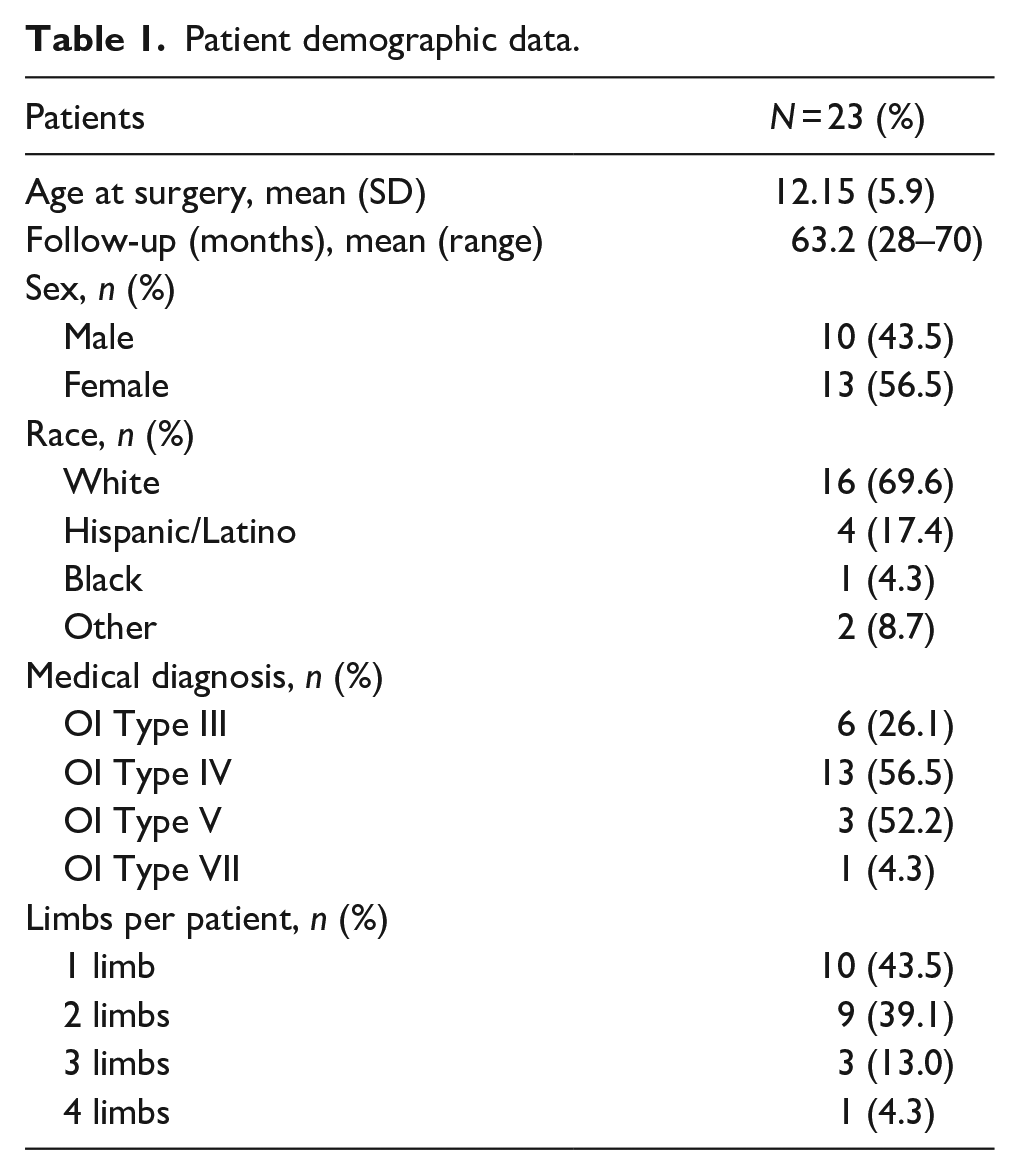
This retrospective study was conducted on 23 patients and 41 limbs, who underwent SLIM nail rodding at our institution between April 2016 and March 2022. The mean age at surgery was 12.15 years (SD = 5.9 years; range = 1–20 years) and mean follow-up was 63.2 months (SD = 7.8). Most surgeries were performed on female patients n = 13 (56.5%). The majority of patients were diagnosed with osteogenesis imperfecta type IV (n = 13) and osteogenesis imperfecta type III (n = 6). Table 1 summarizes patient demographic data.
Patient demographic data.
While most patients had multiple limbs operated on with a SLIM nail (n = 15), 10 patients had one limb operated on only. Among the 41 operated limbs, the majority were the tibia (n = 33; 80.5 %), then the femur (n = 7; 17.1%), and one humerus (2.4%). The SLIM nail diameter used ranged from 2.0 to 5.6 mm, with the most common nails used being the smaller diameter nails—2.0 mm (n = 13; 31.7%), 2.6 mm (n = 9; 22.0%), and 3.2 mm (n = 12; 29.3%). The SLIM nails with diameters >3.2 mm were used in skeletally mature patients, in which the patients’ IM canal could not accommodate the smallest solid IM nail (7.0 mm). In some cases, rotational instability was noticed intraoperatively; thus a semi-tubular plate was used to stabilize the osteotomy site in 17 limbs (41.4%), including 13 tibiae, 3 femurs, and 1 humerus. Table 2 summarizes surgical demographic data.
Surgical demographic data.
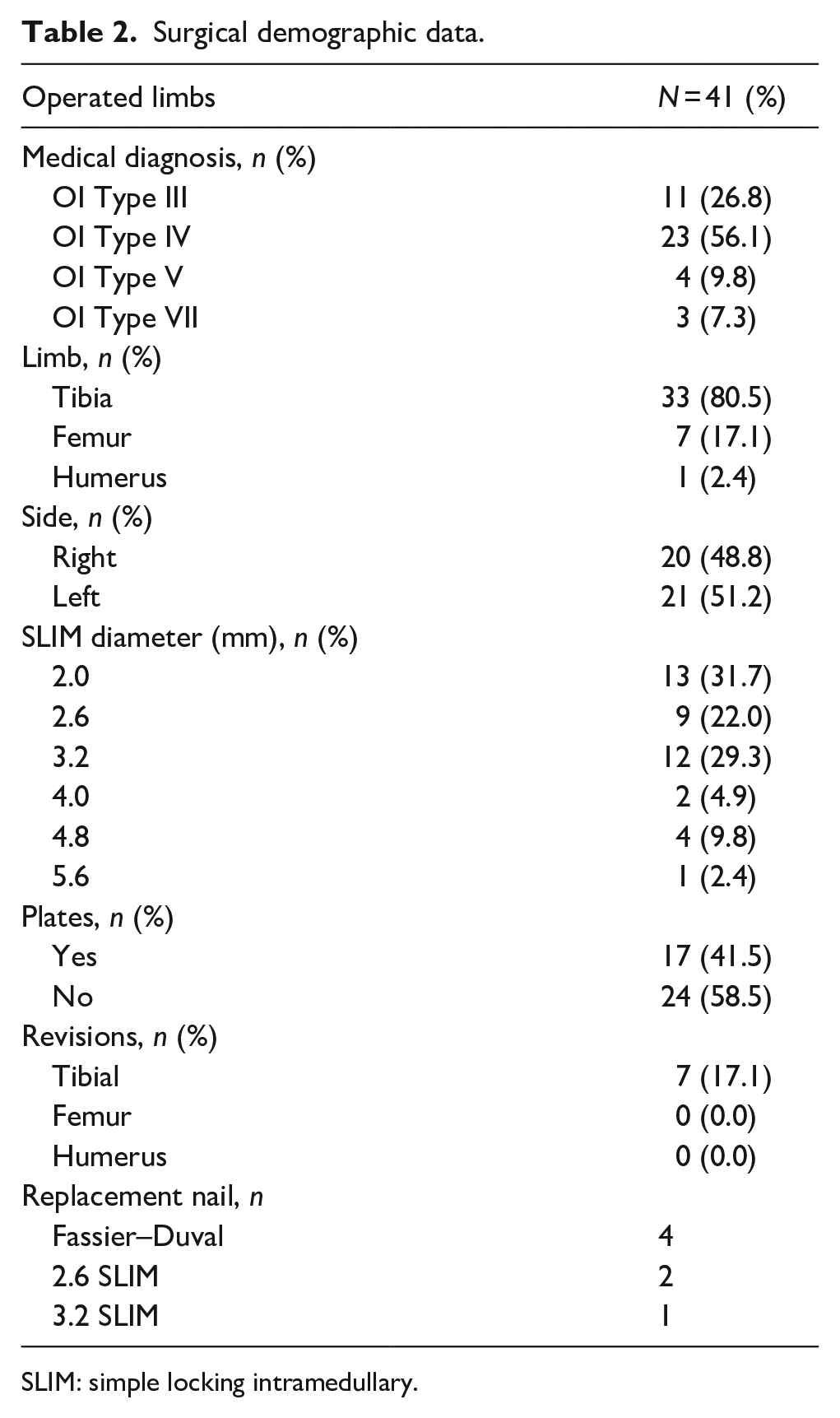
SLIM: simple locking intramedullary.
Bisphosphonate treatment was administered following standard protocol at our institution 26 prior to 41 surgeries, using Zoledronate (n = 38) or Pamidronate (n = 3), and following 23 surgeries using Zoledronate (n = 22) or Pamidronate (n = 1). Dosage and frequency of bisphosphonate treatments were dependent on age, exposure to IV bisphosphonates, and lumbar spine areal bone mineral density. 26
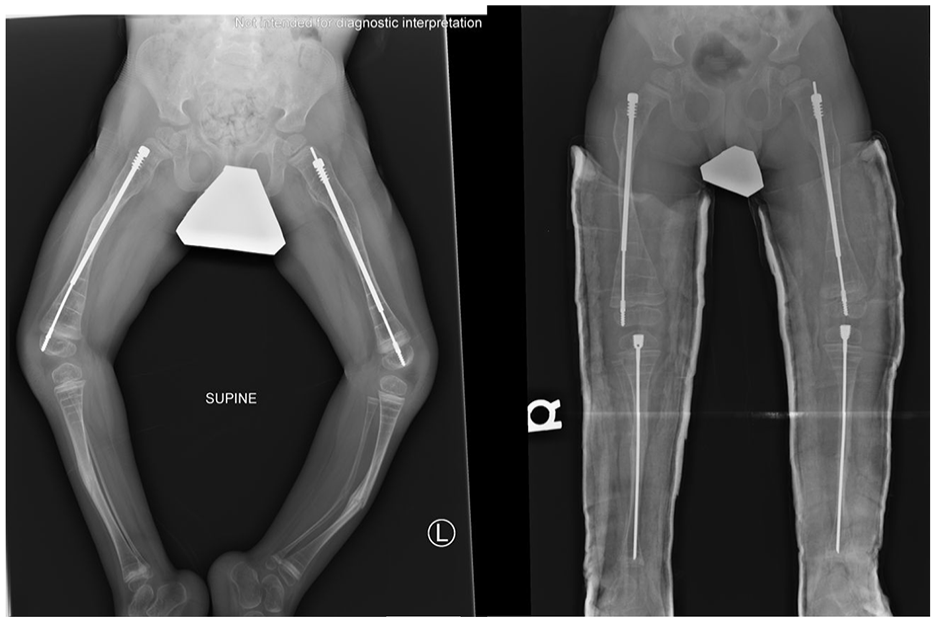
The following case provides an example of a common indication for SLIM nail use in our cohort. A 2-year-old boy with osteogenesis imperfecta type IV presented with severe femoral and tibial deformities, indicating the need for surgical correction (Figure 2). SLIM nail was indicated in both tibias because of the narrow intramedullary canal that would not accommodate the smallest diameter FD rod. Therefore, he underwent bilateral femur osteotomies with FD rods, followed by bilateral tibial osteotomies with SLIM nails at age 3 (Figure 3). At 7 years, incomplete osteotomy healing was noted (Figure 4), and at 9 years, severe angular deformity in the distal unprotected bone was observed, thus indicating revision (Figure 5). The right tibial SLIM nail was replaced with the same size (2.0 mm) due to persistence of the narrow canal (Figure 6).

Pre-operative X-ray of a 2-year-old boy with osteogenesis imperfecta type IV, showing severe bilateral femur deformity.
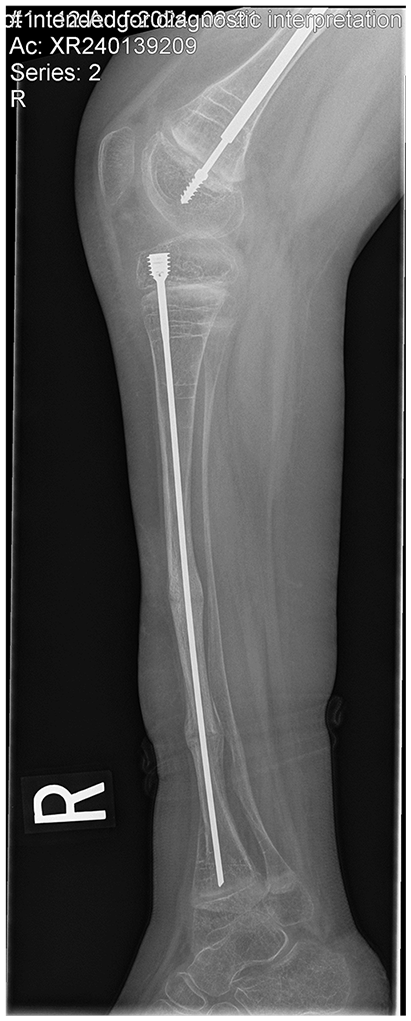
Post-operative X-ray following bilateral femur osteotomy and FD rod insertion at age 2, followed by bilateral tibial osteotomy and SLIM nail insertion at age 3.
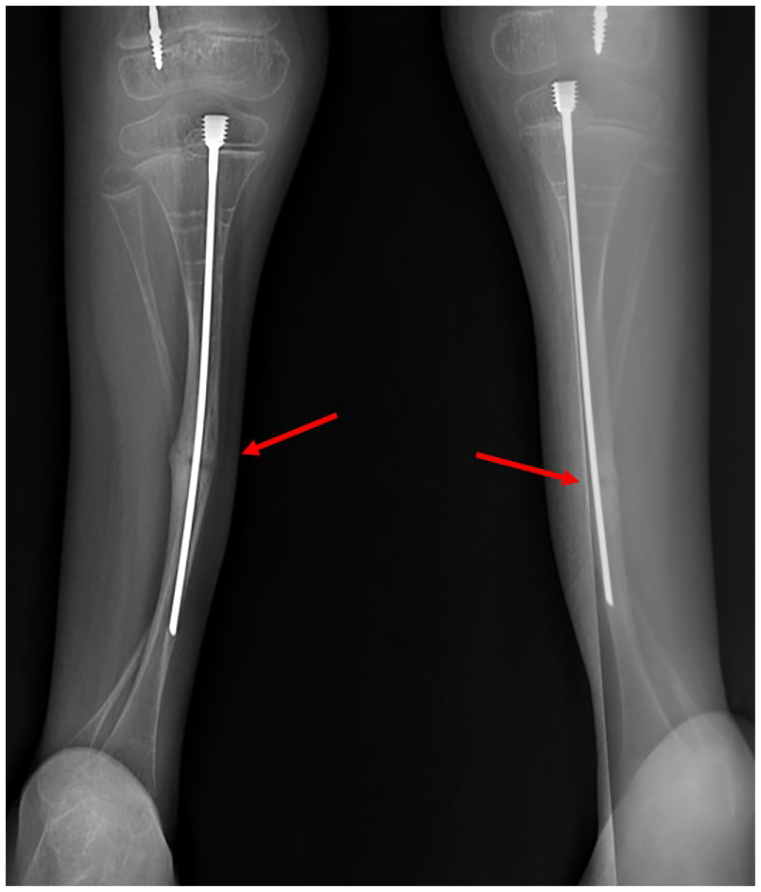
Follow-up X-rays in the patient at 7 years old showing incomplete healing of the osteotomy fracture lines.
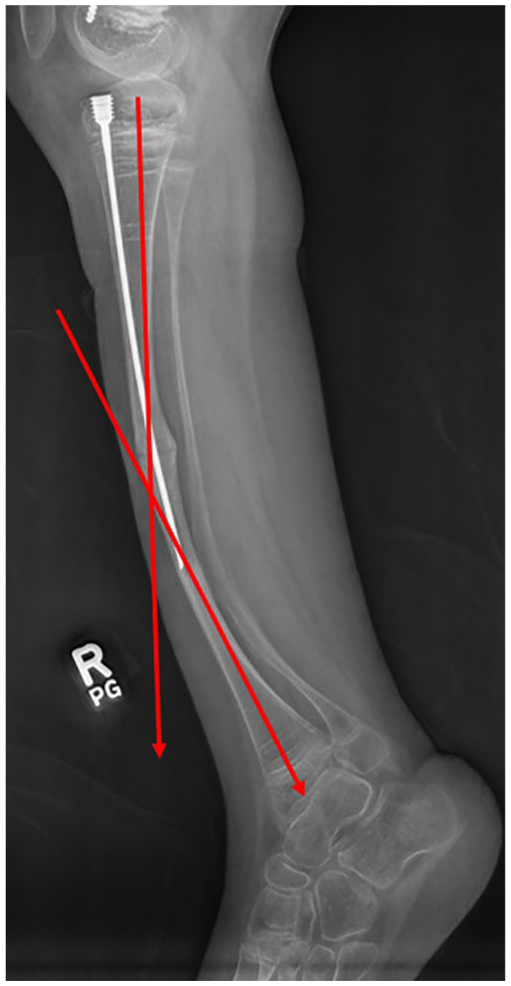
Pre-revision X-ray in the patient at 9 years old, showing angular deformity in the distal unprotected bone.
Post-revision X-ray of right tibia in the patient at 9 years old following revision of the SLIM nail with a longer SLIM nail of the same diameter.
Complications and revisions
The most common complication in non-telescoping nails is developing angular deformity in the distal growing part of the bone, which is not protected by the nail (Table 3). This complication occurred in 19 tibia patients. One patient had a broken SLIM nail (2.0 mm) 34 months after the index surgery, which was revised with a 3.2 mm SLIM nail. The new nail remained intact. One patient had a tibia nail that was too long (3.2 mm) that migrated proximally under the patella 3 months after the initial surgery and was revised with a smaller (2.6 mm) and shorter nail. (Figure 7)
Complication rates.
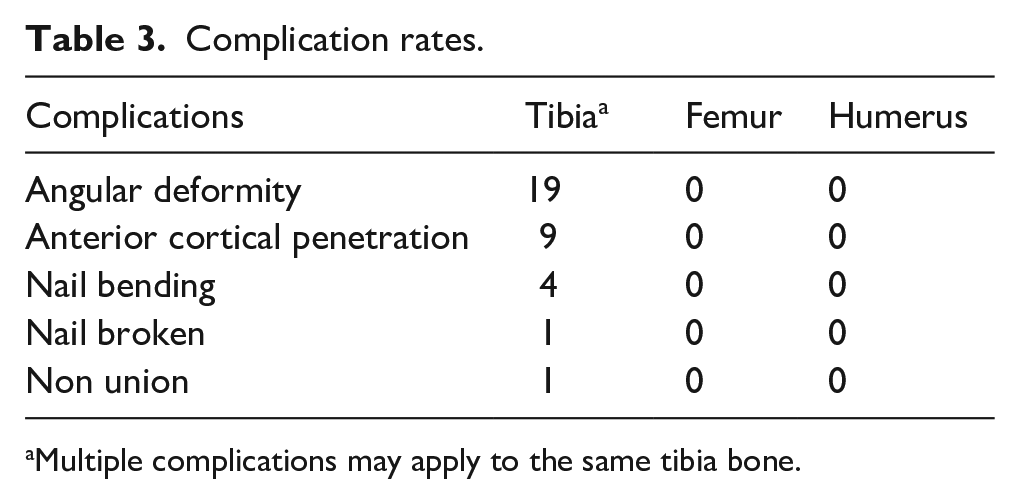
Multiple complications may apply to the same tibia bone.
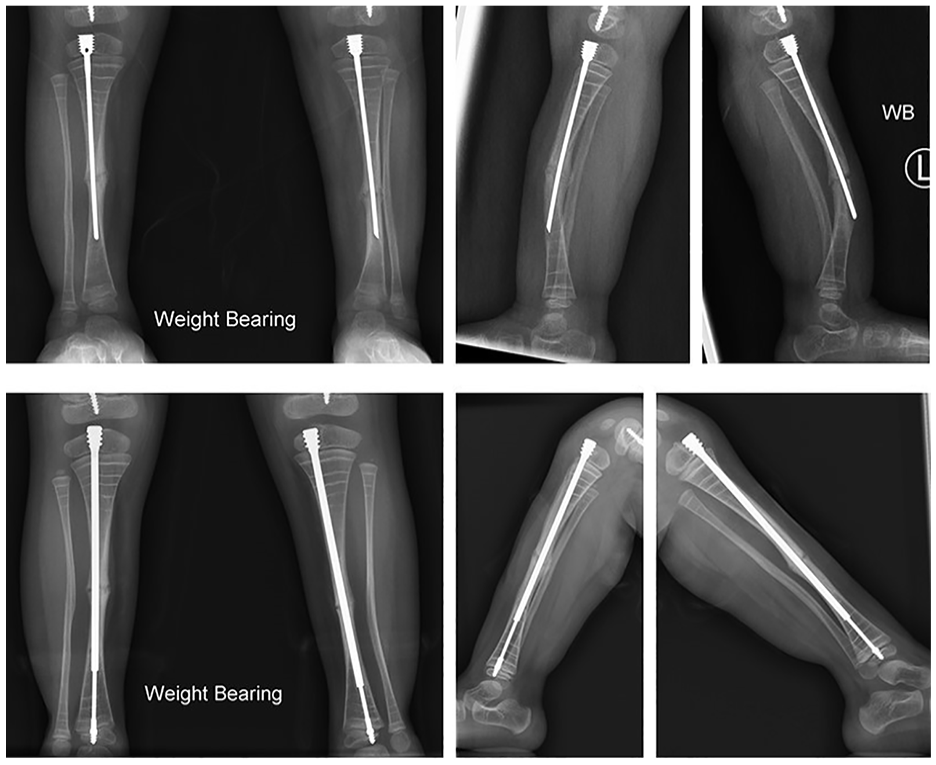
Top row showing 16-month follow-up X-rays demonstrating bone growth, deformity, and rod perforation at the anterior cortex. The bottom row shows 10-month follow-up X-rays of both tibias done post-revision of the SLIM nails to FD rods.
In the present series of 41 rods, 7 rods needed revision. It is important to note that the outgrowth of the nail alone was not an indication for revision in this series, whether the bone and rod are straight or in cases with slight angular deformity. Our criteria for revision are based on the presence of one or more of the following:
- Fractures, including fractures in the presence of a nail, displaced or angulated fractures, repeated fractures in the same bone, and some cases of nondisplaced fractures
- Pain even without angulation or deformities
- Radiologically, angulated rods or bones more than 25 degrees in the coronal or sagittal plane, or penetration of the cortex distally with deformity
The SLIM nail survival rate was analyzed using the Kaplan–Meier Survival Analysis. The SLIM nail has a 2-year survival rate of 82.8% and a 4-year survival rate of 77.1% when used in the tibia (Figure 8). All 33 tibia nails were included in this analysis. The average age of the patients with tibia nails was 12.0 years old.
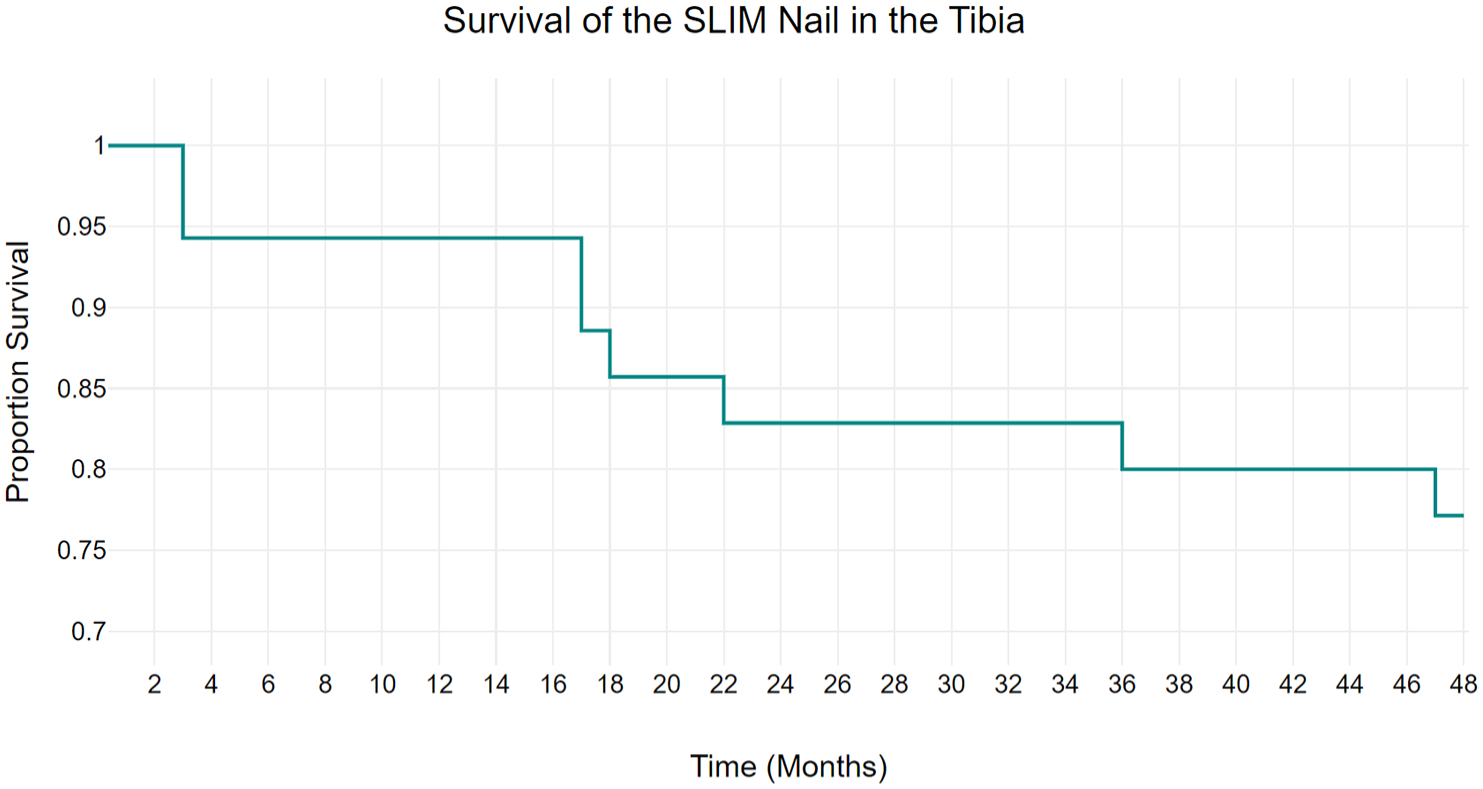
Kaplan–Meier survival analysis demonstrating the survival rate of the SLIM nail in the tibia.
None of the femur nails were revised during this study period as there were no complications, likely due to the fact that most femur operations were done at an older age and with larger nails.
The total revision rate of the tibia was 21.2 % (n = 7 patients), 4 of them revised to FD telescoping nail, 2 revised to 2.6 SLIM, and 1 revised to 3.2 SLIM. A revision may be due to multiple causes. Pain was present in all revisions. Causes include anterior cortex breaking (n = 5), deformity of the unprotected distal bone (n = 4), and hardware failure (n = 2) (Table 4). To further clarify, five patients had angular deformity with anterior cortex penetration, one patient had a nail that was too long, and one patient had a broken nail. All patients who underwent revision had relief of pain post-operatively and remained asymptomatic.
Revision causes.
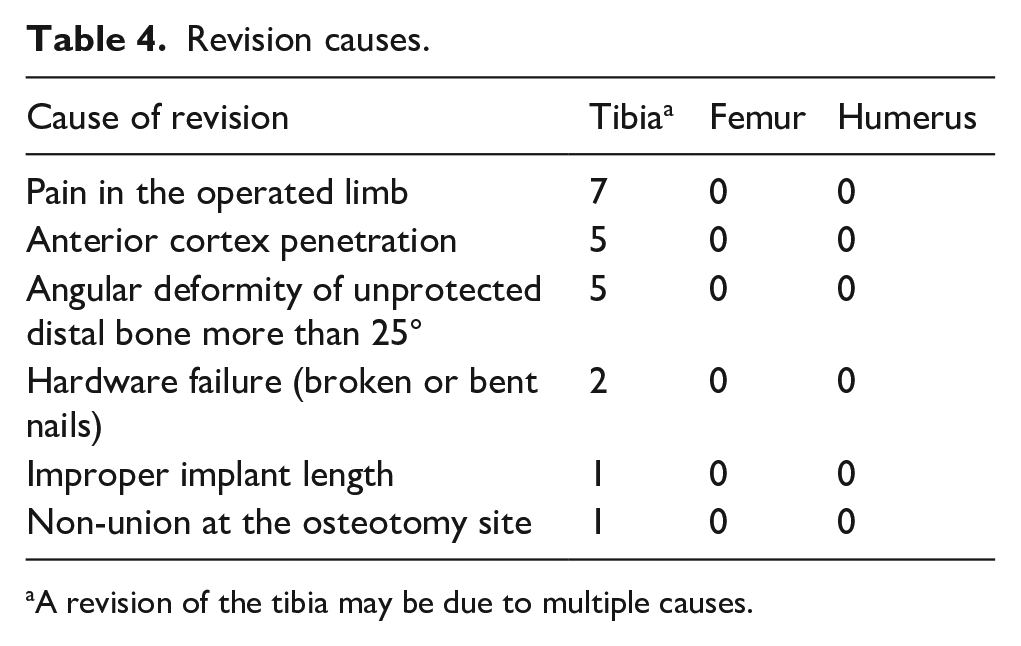
A revision of the tibia may be due to multiple causes.
Discussion
To the best of our knowledge, this is the first reported study on the outcomes and complications of the simple locking intramedullary nail (SLIM nail) in the treatment of patients with OI and other osteopenic bone diseases. In patients with OI, the indications for surgery with the use of the SLIM nail are the same indications as other rods: multiple fractures in the same bone (>1), deformity greater than 30 degrees in the coronal or sagittal plane, and the presence of multiple episodes of long bone pain. The primary goal of surgery in this population is to correct the bone deformity and provide full-length support to the bone throughout skeletal growth. Biomechanically, straight bones are less vulnerable to fractures than deformed bones, making proper alignment important for long-term stability. 27 The vast majority of our patients were ambulatory; however, if non-ambulatory patients present with fractures, pain, or discomfort, rodding was still indicated due to the potential for increased quality of life.
Historically, fracture and deformity in OI patients with small intramedullary canals were treated either conservatively by casting or by other static intramedullary rods such as K-wires or Rush rods. However, these methods were associated with high complications, including migration of rods and worsened deformity.28,29 The SLIM nail design avoids migration, as the nail head is threaded through the proximal epiphysis of the bone and prevents it from migration. A meta-analysis by Scollan et al. 30 assessed post-operative outcomes of non-elongated intramedullary nails for lower limbs in OI patients. 7 studies (229 OI patients) were included in their final analysis with most of the nails that they used being Rush nails. They found that the most common complication post-operatively was migration (25.7 %), followed by fracture (15%). In our series, only one case (2%) had migrated immediately post-operative due to wrong length measurement.
Our study demonstrated that the most common complication of using SLIM nails is bone deformity due to outgrowing of the limb at the unprotected distal part of the bone in 19 limbs. In our series, seven revisions occurred, five at ages 1, 1, 3, 3, and 9 due to implant outgrowth along with the previously mentioned indications for revision, and two at ages 14 and 17 due to hardware failure. Notably, the average age of revision (5.42) was younger than the mean age of the study cohort (12.15), highlighting the challenge of implant longevity in younger, growing patients. This has been previously reported in the literature with the use of non-elongating rods.29,31 Wei-Chun Li et al. conducted a study involving 18 patients with an average age of 6.9 years old, with 32 femurs undergoing fixation using non-elongating rods. Their findings revealed that 24 of these rods required revision due to outgrowing, with five of the 24 revisions requiring re-revisions also due to outgrowing. 31 In a case series by Imajima et al., 17 patients with 29 femur rod placements with K-wires were evaluated. 32 They recommended revising the K-wire before the wire-length ratio drops below 70%, based on their findings that show a significant increase in wire-tip fractures when the wire-length ratio is between 65% and 70%. They concluded that this was the proper time to prevent further fracture of the outgrowing part of the bone. The wire-length ratio is defined as the length of the intramedullary K-wire divided by the length of the bone from the proximal femoral epiphysis to the distal femoral epiphysis. Although we did not apply this measurement in our study, it represents a reasonable guideline for surgeons using SLIM nails in the femur or tibia to determine optimal timing for revision. Figure 9 demonstrates this ratio using the SLIM nail in a skeletally immature tibia.
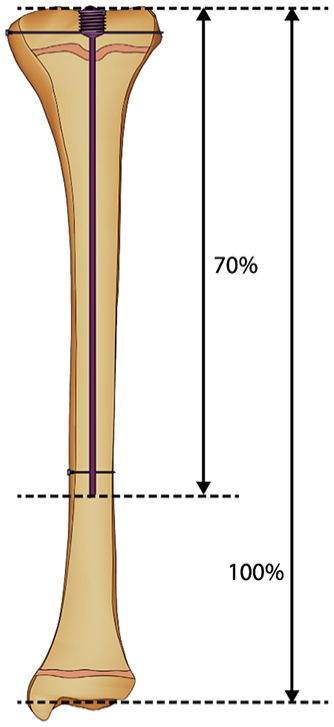
Wire-length ratio of 70% in a skeletally immature tibia.
Our study exclusively observed complications in the tibia bones, likely due to the predominant use of SLIM nails with smaller diameters in these cases. The Kaplan–Meier curve demonstrated survivorship rates of 82.8% at 2 years and decreasing to 77.1% at 4 years. These rates compare favorably to previous studies using static rods, where survivorship ranged from 36% to 52% at similar time points.17,32 –34 However, they are lower than survivorship rates reported for telescoping nails, which range from 77% to 92.9%.17,35
Conclusion and limitations
Our study demonstrated that the SLIM nail could be a viable option in the management for patients with a narrow intramedullary canal that cannot accommodate a telescoping rod. Additionally, our results showed that the SLIM nail performed better than other non-elongating nails in treating lower extremity fractures and deformities in OI patients. However, since skeletally immature patients often outgrow the SLIM nail, it is important to inform patients and their parents that revision surgery will likely be required. Although the SLIM nail effectively addresses nail migration, it still has a high incidence of deformity in the distal unprotected part of the bone due to outgrowth. Given that all observed complications and revisions were due to overgrowth, we strongly recommend monitoring the ratio of the nail to bone length to anticipate the need for revision before fracture or deformity occurs. Once indicated, we recommend converting the SLIM nail to a telescoping nail if the intramedullary canal is large enough to accommodate it. Limitations of this study include it being a retrospective study and the small number of cases.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251359105 – Supplemental material for Using the simple locking intramedullary (SLIM) system for bone deformity stabilization: A retrospective cohort study
Supplemental material, sj-pdf-1-cho-10.1177_18632521251359105 for Using the simple locking intramedullary (SLIM) system for bone deformity stabilization: A retrospective cohort study by Peter Joseph Mounsef, Sofia Addab, Saleh Alfaisali, Mitchell Bernstein and Reggie Hamdy in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
Not applicable.
Author contributions
Peter Joseph Mounsef—Conceptualization, data curation, article redaction, and article review. Sofia Addab—Conceptualization, data curation, article redaction, and article review. Saleh Alfaisali—Conceptualization, data curation, article redaction, and article review. Mitchell Bernstein—Providing data, article review, and supervision. Reggie Hamdy—Study planning, data review, article redaction, article review, supervision, and final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethical approval from the institutional review board was obtained (A04-E17-22A) and informed consent for publication was received from all participants, or in the case of children, their parent or legal guardian, for use of their data.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to patient confidentiality but are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.