
Abstract
Background:
Septic knee arthritis in pediatric patients is rare; however, timely diagnosis and treatment is key in preventing damage to articular cartilage and other structures in the joint. Risk and prognostic factors associated with treatment failure have not yet been studied in this patient population. In this study, we aim to assess how various lab and clinical findings at time of initial presentation associate with need for subsequent debridement among pediatric septic knee patients.
Methods:
This is a retrospective, single-center, case–control study comparing patients who did and did not receive subsequent irrigation and debridement for septic arthritis of the knee. Risk factors were assessed through univariate comparisons, utilizing chi-squared tests, t-tests, and Fisher-exact tests, as appropriate. Multivariate logistic regression and area under the receiver operating characteristic (AUROC) analysis was used to assess discriminatory ability of identified risk factors. Significance was defined as p < 0.05.
Results:
A total of 41 patients were included in this study, of which 18 underwent subsequent debridement. Patients requiring subsequent debridement had higher rates of positive blood culture (43.8% vs. 6.7%, p = 0.04), positive synovial cultures (66.7% vs. 26.1%, p = 0.01), and synovial white blood cell counts (WBC) > 100,000 cells/L (53.3% vs. 20.0%, p = 0.04). When these three variables were placed in a logistic model, an AUROC of 0.82 was observed (95% confidence interval: 0.64–0.99)
Conclusions:
Positive blood and synovial cultures, and synovial WBC > 100,000 cells/L, were identified as significant prognostic factors for subsequent septic knee surgery. Clinicians should consider these factors when counseling patients and caregivers about risk for subsequent debridement.
Level of Evidence:
III; Retrospective Case–Control Study.
Introduction
Septic arthritis of the knee is the most common form of septic arthritis in children, and although reported incidence varies widely, it is estimated to range from 4 to 37 cases per 100,000 children.1–3 Acute septic arthritis is typically caused by hematogenous spread from a distant site of infection in children and the most common pathogen is Staphylococcus aureus, with methicillin-resistant strains becoming increasingly prevalent. 4 Infection within the joint space presents with severe pain, swelling, erythema, and limited range of motion; septic arthritis can be diagnosed clinically or based on arthrocentesis. In children especially, timely diagnosis and management is critical to decrease the risk of damage to the articular cartilage and other intra-articular structures. 5 Septic arthritis can result in complications such as persistent infection, growth disturbance, chondrolysis, and degenerative arthritis.5,6 These patients are also at risk for osteomyelitis, recurrent joint infection, and sepsis. The rate of these sequelae has been cited at 10% among all patients with septic arthritis of the knee, with delayed diagnosis and treatment leading to an increased incidence of long-term complications. 7
At our institution, patients with a concerning clinical exam and laboratory studies undergo aspiration to evaluate the synovial fluid. Advanced imaging with magnetic resonance imaging (MRI) is typically obtained in patients for whom there is a high suspicion for adjacent osteomyelitis/soft tissue infection or an atypical presentation. If the aspiration results are consistent with intra-articular infection, patients at our institution undergo operative irrigation and debridement (I&D) via arthrotomy or arthroscopy according to surgeon preference, along with concomitant intravenous antibiotics. The majority of our attending surgeons prefer open arthrotomy for I&D. Our institution does not typically perform a trial of antibiotics prior to surgical intervention. Empiric antibiotics are routinely started after joint aspiration, to allow for acquisition of a tissue culture to guide subsequent narrowing of antibiotic therapy. Some patients will require repeat debridement due to persistence or recurrence of symptoms following initial operative intervention. Repeat I&D is posited to decrease the disease burden and decrease the risk of the above complications and sequelae. To our knowledge, there are no case–control studies investigating the need for subsequent debridement after index surgical management of septic arthritis of the knee in children.
The purpose of this study was to determine factors associated with pediatric patients who require a repeat debridement after index I&D for septic arthritis of the knee. The incidence and risk factors associated with repeat septic knee debridement in children have previously been investigated in a retrospective database study. This study found that an increased Charlson Comorbidity Index and shorter length of stay were predictive of requiring a subsequent I&D. 8 The need for subsequent debridement after initial washout has been similarly studied in pediatric septic arthritis of the hip.9–13 These studies reported a strong association among certain lab and clinical findings and subsequent operative debridement, including higher C-reactive protein (CRP), fever, and positive blood cultures. We hypothesize that similar preoperative risk factors may exist for recurrent septic arthritis of the knee in children.
Materials and methods
Study design
This is a retrospective, single-center, case–control study looking to determine risk factors for subsequent debridement in patients with septic knee arthritis. Patients were included if they were aged 0–18 years, underwent knee I&D for septic knee arthritis from 2005 to 2020. Data were collected from the electronic medical record. Cases were patients that underwent a second debridement, and controls were patients that did not undergo a second debridement. Demographic data including age, sex, ethnicity, race, insurance, and state were collected for all patients. Clinical data, including lab results and comorbidity data, were also collected. Specifically, data were collected on estimated blood loss, time to debridement from admission, blood and synovial fluid cultures, arthroscopic versus open procedure, CRP, erythrocyte sedimentation rate, inability to weight-bear, white blood cell count (WBC), neutrophil count, platelet count, left shift, intraoperative abscess or purulence, and synovial WBC. Patients were included if they had a minimum of 2 years follow-up after index I&D. Patients were excluded if they had concomitant osteomyelitis at index procedure. The study was reviewed by our university’s Institutional Review Board and found to be exempt.
Statistical analysis
Descriptive statistics were used to summarize the study population. Potential risk factors were identified univariately by comparing patients who received and did not receive subsequent debridement via chi-squared tests, Fisher-exact tests, and t-tests, as appropriate. Risk factors were considered significant at p < 0.05. Identified risk factors were then placed into a multivariate logistic regression model where discriminatory ability of the identified risk factors was assessed using an area under the receiver operating characteristic (AUROC) analysis. Analyses were conducted using Stata 15.1/SE (StataCorp LLC, College Station, TX, United States).
Results
Patient population and demographics
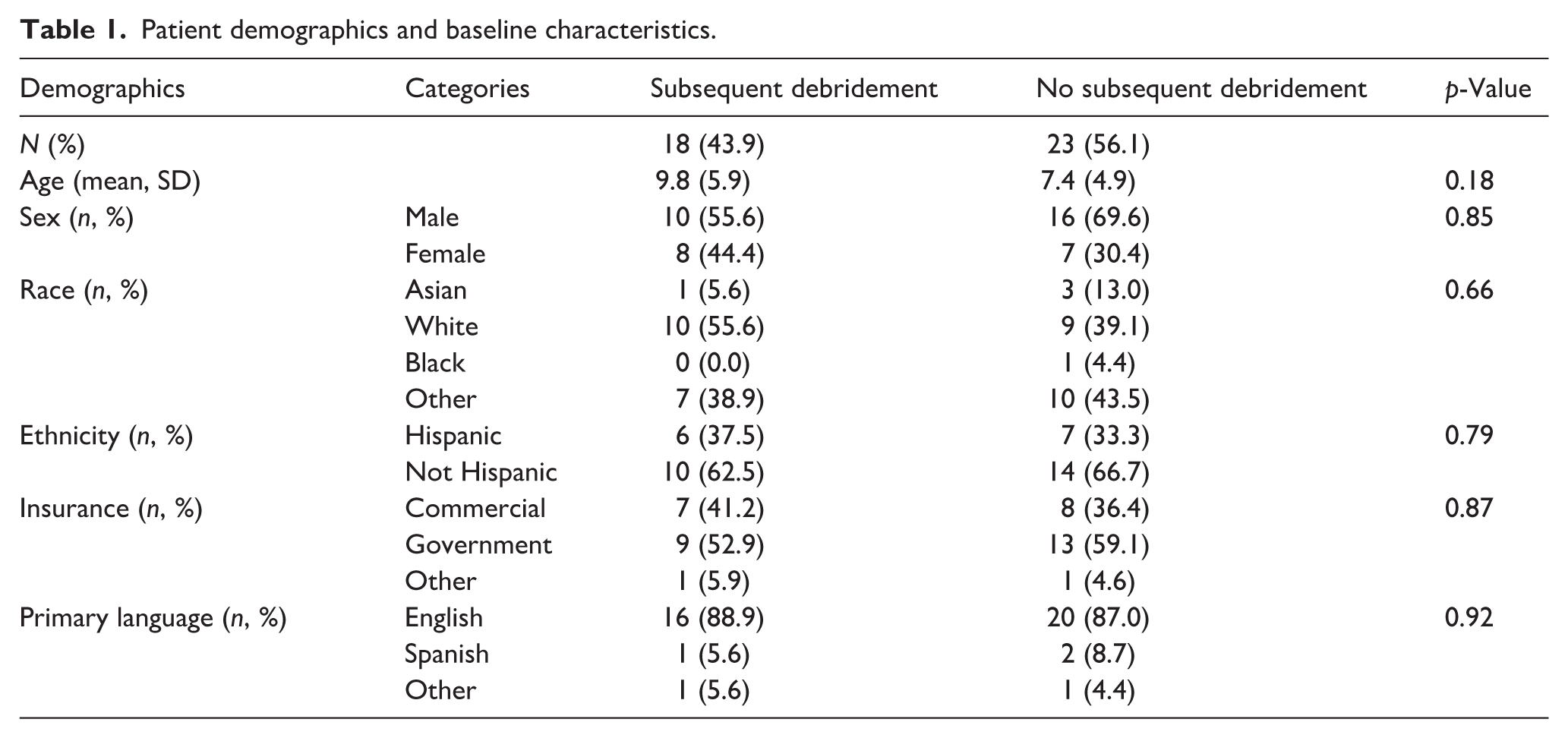
A total of 41 patients with septic arthritis of the knee were included in this study, 23 in the control group and 18 in the case group who had undergone repeat surgery for debridement. The patients ranged in age from 0 to 21 years of age. The average age of patients who did not receive subsequent debridement was 7.4 years (Standard deviation (SD) 4.9), while those who did receive subsequent debridement were an average of 9.8 years old (SD 5.9) (p = 0.18) (Table 1). There was only one infant (less than 1 year of age) in the study cohort, and this patient was in the control group. There were nine total toddlers (between 1–3 years of age) in the cohort, seven in the control group, and two in the case group that required subsequent debridement. The majority of patients in both control and subsequent debridement groups were male (69.6% vs. 55.6%, respectively, p = 0.85), non-Hispanic (66.7% vs. 62.5%, respectively, p = 0.79), used government insurance (59.1% vs. 52.9%, respectively, p = 0.87), and were primarily English-speaking (87.0% vs. 88.9%, respectively, p = 0.92). For the index surgery, 2 patients underwent arthroscopic I&D and 39 patients had an open arthrotomy with I&D. None of the subsequent debridements were performed arthroscopically. The majority of subsequent debridements (15 patients) occurred less than 1 week after the initial debridement, with an average time to second debridement of 3.13 days. Three patients underwent subsequent debridement more than 20 days after their first washout, with an average time of 27.3 days. Notably, six patients underwent an additional subsequent debridement after their second debridement surgery. These patients underwent this third I&D an average of 3.5 days after their second washout operation. There were also two patients who underwent subsequent debridement of additional septic joints that developed during their hospitalization, after the initial debridement of the septic knee that was symptomatic upon presentation.
Patient demographics and baseline characteristics.
Only two patients in the cohort received a preoperative MRI; both of these patients went on to require a second debridement after their index I&D. One of these patients required two subsequent debridement surgeries and developed chronic osteomyelitis. Two of the patients in the control group received a postoperative MRI compared with 11 of the patients in the case group who required subsequent debridement.
Seventeen of the patients in the cohort had no growth on culture collected during surgical debridement; 13 of these patients required only 1 debridement while 5 of these patients required repeat debridement. Only one patient (3 years old) was found to have Kingella kingae on polymerase chain reaction (PCR) analysis. Of the patients who had an organism identified on culture, seven patients grew methicillin-resistant staph aureus (MRSA), six patients grew menthicillin-sensitive staph aureus (MSSA), five patients grew group A, B, or viridans strep, and one patient each grew polymicrobial cultures, Escherichia coli, pseudomonas, Gram-positive rods, and Achromobacter xylosoxidans.
Risk factor identification
There were no significant differences in demographics or baseline characteristics between patients who did and did not receive subsequent debridement. In assessing lab results that were obtained at initial encounter prior to first I&D for septic arthritis, patients who required subsequent debridement were found to be more likely to have positive blood (43.8% vs. 6.7%, p = 0.04) and synovial fluid cultures (66.7% vs. 26.1%, p = 0.01) relative to those who did not require a second surgery for septic knee arthritis (Table 2). Additionally, patients who required a subsequent debridement were found to be more likely to have synovial WBC > 100,000 × 109/L (53.3% vs. 20.0%, p = 0.04) (Table 2).
Univariate risk factor assessment for subsequent debridement after initial irrigation and debridement for septic knee arthritis.
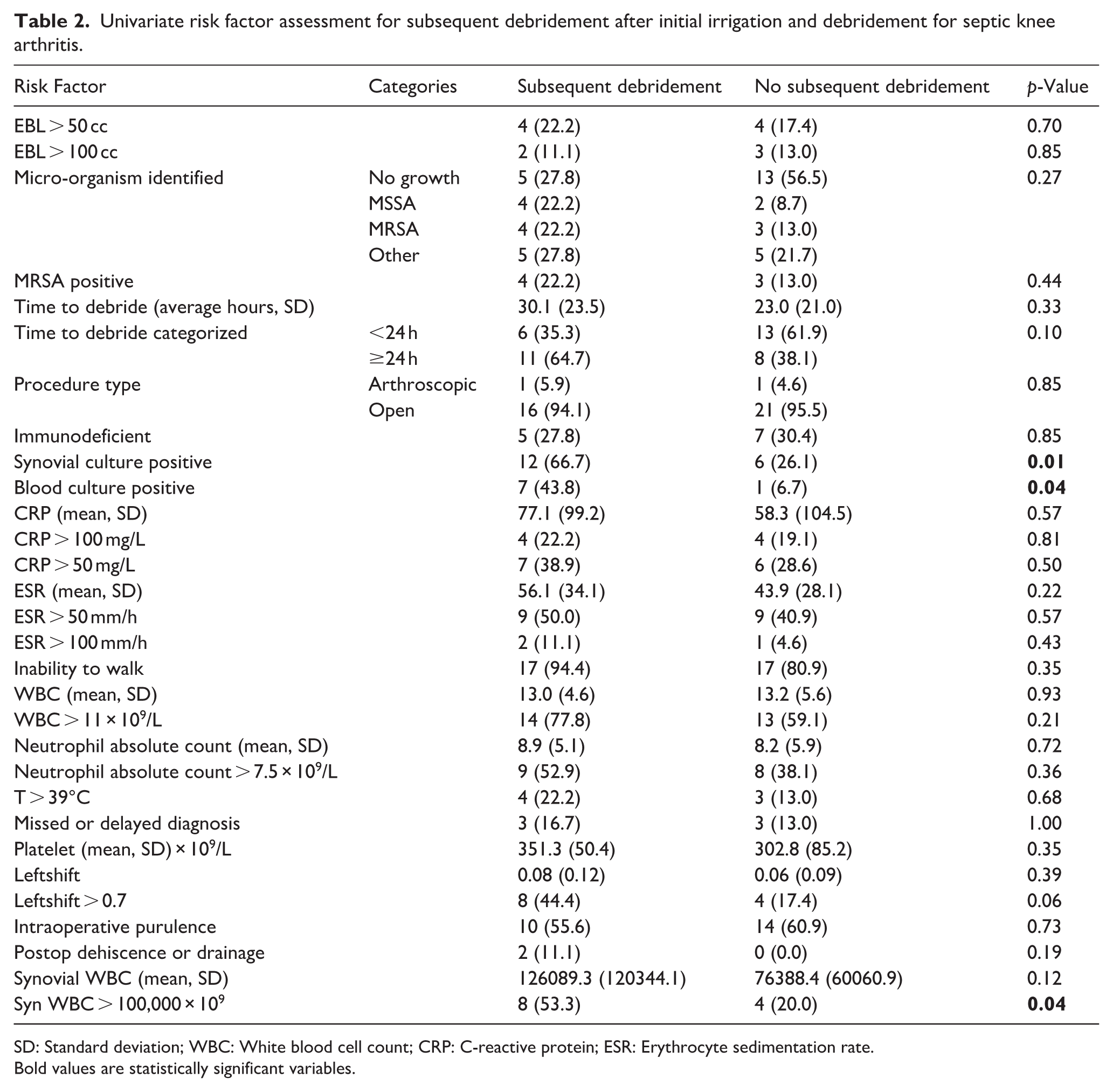
SD: Standard deviation; WBC: White blood cell count; CRP: C-reactive protein; ESR: Erythrocyte sedimentation rate.
Bold values are statistically significant variables.
There were no significant differences between our control and subsequent debridement group when comparing proportions of patients who had inability to walk at initial encounter, estimated blood loss (EBL) > 50 or >100, time to debridement, or whether they were immunodeficient (defined as having an underlying autoimmune condition, recent history of chemotherapy, recent history of steroid use, determined by chart review). There was no significance difference between receiving an open arthrotomy versus arthroscopic I&D as the index surgery. The age of patients who required subsequent debridement trended older (average 9.8 vs. 7.4 years of age) but did not reach statistical significance.
Multivariate logistic regression and AUROC
Identified risk factors, including blood culture positivity, synovial fluid culture positivity, and synovial WBC (both continuous and abovementioned categorical term) were placed into a multivariate logistic regression model to assess for discriminatory ability between patients who require and do not require subsequent debridement. From this model, it was determined that patients with risk factors of positive blood cultures (Odds ratio (OR): 12.28, 95% Confidence interval (CI):1.01–148.63, p = 0.04), positive synovial cultures (OR:1.25, 95%CI: 0.17–9.33, p = 0.83), and synovial WBC > 100,000 (OR: 3.09, 95%CI: 0.45–21.40, p = 0.25) were more likely to require subsequent debridement (Table 3). The multivariate model’s AUROC was found to be 0.82 (95% CI: 0.64–0.99) (Figure 1).
Multivariate and AUROC analysis to assess for subsequent debridement discriminatory ability with synovial neutrophil percentage binary categorization.
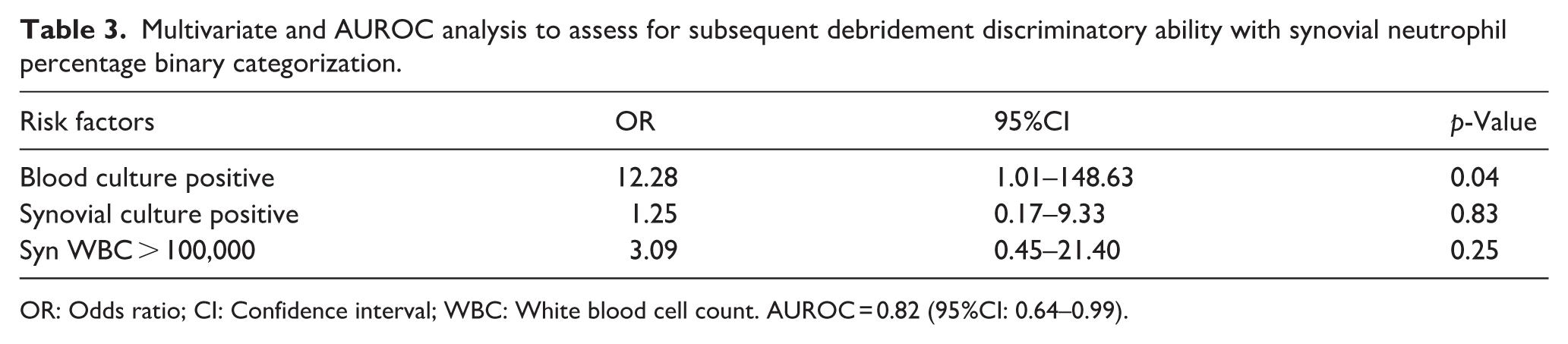
OR: Odds ratio; CI: Confidence interval; WBC: White blood cell count. AUROC = 0.82 (95%CI: 0.64–0.99).
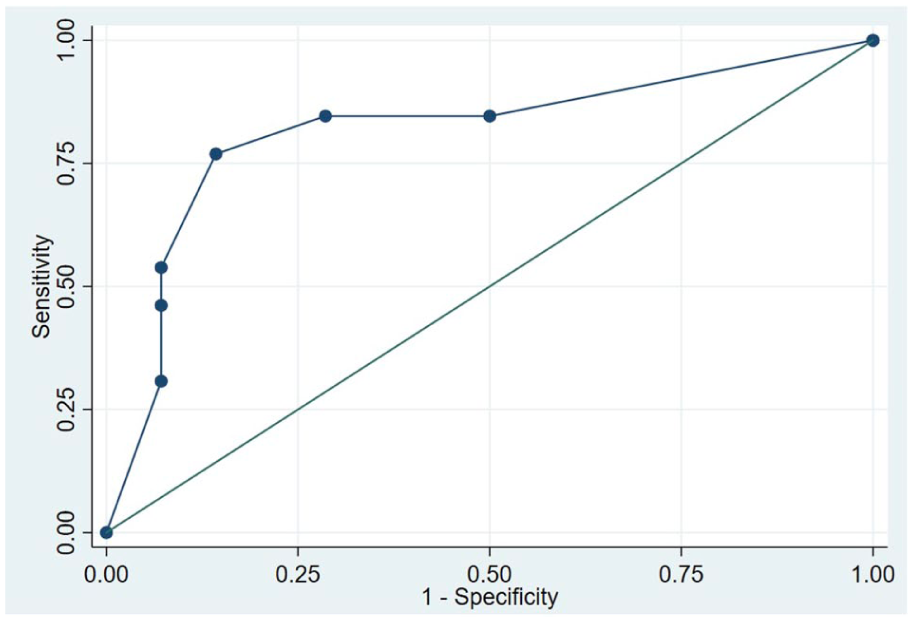
is the AUROCs measurement which assesses the performance of the multivariate logistic regression model.
Discussion
In this study, we conducted a case–control study to identify potential risk factors for subsequent debridement after index debridement in pediatric patients with septic arthritis of the knee. We found that positive blood cultures, positive synovial cultures, and synovial WBC > 100,000 cells/L may be useful predictors of subsequent debridement in this patient population. We also found that these variables have excellent discriminatory ability in assessing patients requiring subsequent debridement when applied to a logistic model. It is important to note that statistical significance of findings from our univariate analysis lost significance in the multivariate logistic model. This may be due to confounding or removing indirect effects of associated variables, as well as our small sample size. However, despite loss of significance, this model had excellent discriminatory ability with an AUROC of 0.82. This suggests that, together, these variables may be effective prognostic measures for identifying pediatric patients that may require additional debridement procedures for septic arthritis of the knee.
Several studies have shown that initial lab values at time of presentation are significant risk factors of subsequent debridement for septic arthritis in a particular joint. Most of these studies, however, have been studied in the setting of septic arthritis of the hip. Both Livingston et al. 9 and Murphy et al. 10 found that higher CRP counts and positive blood cultures are positive predictors for subsequent debridement in pediatric septic hip arthritis patients. We similarly found that positive cultures were associated with higher risk of subsequent debridement. There are limited studies assessing the association of synovial WBC count and secondary surgeries. Ascione et al. 14 have shown that patients with a synovial WBC of greater than 934 cells/µL had higher infection rates in the setting of periprosthetic joint replacement. In a retrospective analysis, Stake et al. identified that the combination of increased synovial WBC and concurrent infection was a significant risk factor for repeat debridement in adult patients with septic arthritis of the knee. In their cohort, the risk of subsequent debridement increased by 1% for every increase of 1000 nucleated cells in the synovial fluid of adult patients who had a concurrent infection. 15 As this finding was identified in an adult population, it is meaningful to have found a similar relationship between elevated synovial WBC and persistent infections in our pediatric patient population. Larger and prospective studies are needed in the future to validate these findings.
In this study, certain risk factors including CRP, MRSA positive cultures, and time to debridement were not found to be statistically significant predictors of repeat debridement. Although significance was not observed in this study, the average CRP and time to debridement was certainly higher in patients who required subsequent debridement. Similarly, rates of MRSA positive cultures were higher in patients who required subsequent debridement. It is possible that our sample size was not adequate to detect the differences observed in this study. However, assessment of risk factors for subsequent debridement for septic knee arthritis in children has only been studied in a limited capacity, so it is difficult to assess which uncaptured risk factors may have impacted outcomes. Further studies with larger sample sizes are required to establish relationships between pertinent risk factors and subsequent debridement for knee septic arthritis.
There are several limitations in this study. Certain analyses are limited by our sample size. However, subsequent debridement is not common for septic arthritis of the knee, and we used a case–control study design to study this question. This was required as previous studies have shown secondary debridement to be relatively rare, with a published rate of 3.6%. 9 Second, additional studies are needed to generalize our findings to other populations as well as assess the validity of this model. Prospective, multicenter studies will be useful in further elucidating factors that may be associated with risk factors for additional debridement in septic arthritis of the knee. Additionally, the majority of our attending surgeons prefer open arthrotomy compared to arthroscopy for I&D; as such, we were unable to meaningfully compare these two methods for debridement during index surgery to see if the surgical technique is a factor affecting the need for subsequent surgery. Lastly, we did not include long-term sequelae and the effects of surgical debridement on long-term risks and outcomes. Future studies are needed to further understand risks of septic arthritis on the pediatric knee.
In conclusion, positive blood cultures, positive synovial cultures, and synovial WBC > 100,000 cells/L were significant risk and prognostic factors for subsequent debridement in pediatric patients with septic knee arthritis. Surgeons should consider these factors when counseling patients, caregivers, and other members of the care team about the possible need for subsequent debridement.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251413464 – Supplemental material for Risk factors for subsequent debridement in pediatric patients with septic arthritis of the knee: A case control study
Supplemental material, sj-pdf-1-cho-10.1177_18632521251413464 for Risk factors for subsequent debridement in pediatric patients with septic arthritis of the knee: A case control study by Kian Niknam, Katherine Bach, Jennifer O’Donnell and Ishaan Swarup in Journal of Children's Orthopaedics
Footnotes
Author contributions
Kian Niknam: Manuscript preparation, study design, statistical analysis
Katherine Bach: Manuscript preparation and editing, study design
Jennifer O’Donnell: Data acquisition, manuscript preparation, study design
Ishaan Swarup: manuscript preparation, study design, supervision
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was reviewed and determined to be exempt from Institutional Review Board (IRB) review under our university institutional regulations as it involves retrospective analysis of de-identified data and does not meet the definition of human subjects research.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.