
Abstract
Background
Musculoskeletal infections are among the most common bacterial infections in children leading to hospitalization, invasive procedures and prolonged antibiotic administration. Blood, synovial and sometimes tissue cultures are essential for the diagnosis and treatment of musculoskeletal infections; 16S ribosomal DNA (rDNA) sequencing is a novel diagnostic tool for the detection of bacteria.
While the yield of 16S rDNA sequencing in synovial fluid was previously assessed, data regarding the efficacy of this method from blood samples or partially treated children with suspected musculoskeletal infections is lacking.
In this study we assessed the yield of 16S rDNA sequencing in blood, bone and synovial samples of children with musculoskeletal infections.
Methods
Blood, synovial and bone samples were collected from children with suspected musculoskeletal infections and analyzed for the presence of 16S rDNA, the results were then compared with the benchmark microbial cultures.
Results
During the study period, 41 children (18 boys and 23 girls) with suspected acute musculoskeletal infection were enrolled. A positive blood culture was found in 6/31 cases (19.4%) with methicillin-susceptible Staphylococcus aureus being the most commonly isolated bacterium. No significant 16S rDNA detection in blood samples was recorded.
Synovial fluid culture was positive in 6/28 samples (21%), Kingella kingae being the most common pathogen. When using the 16S rDNA sequencing method, the rate of positive results in synovial fluid was higher with bacterial detection in 12/23 (52%) samples. The 16S rDNA sequencing method was also able to identify pathogens in samples taken from partially treated children where cultures were negative with 16S rDNA detection in 5/5 samples.
Conclusion
Although 16S rDNA sequencing may increase the yield of bacterial detection in synovial samples of patients with musculoskeletal infections, there is no benefit from applying this method on blood samples. The 16S rDNA sequencing method may be particularly beneficial when antibiotic treatment was started prior to synovial fluid sampling.
Level of Evidence
Level-II diagnostic study
Introduction
Musculoskeletal infections are among the most common bacterial infections in children leading to hospitalization, invasive procedures and prolonged antibiotic administration.1,2 Most cases of musculoskeletal infections in children arise haematogenously and typically involve the metaphysis of long bones and joint synovia. 3
As there is no single test to confirm or exclude musculoskeletal infections, the diagnosis relies on combined assessment of clinical, laboratory and imaging parameters.
Although many ancillary tests such as MRI, Technetium-labelled methylene diphosphate bone scan and blood inflammation markers are available, bacterial isolation and susceptibility testing are fundamental to the definitive diagnosis and treatment of musculoskeletal infections.
A novel method for identifying infectious bacteria is 16S ribosomal DNA (rDNA) sequencing, 16S rDNA is a component of the 30S subunit of prokaryotic ribosomes and is present in all prokaryotic organisms. The specific 16S rDNA sequence of every microorganism is unique and thus allows identification of various species of bacteria according to their phylogenetic origins. 4
The 16S rDNA sequencing method may become an important diagnostic tool for identification of the causative pathogen in musculoskeletal infections. Although several studies have assessed the use of this method for microbial identification in musculoskeletal infections,5,6 they focused on synovial samples and not blood samples.
The aim of this study was to assess the yield of bacteria using16S rDNA sequencing in blood, synovial and bone samples compared with that of blood, synovial fluid and bone cultures of samples taken from children with musculoskeletal infections.
Patients and methods
Following approval by the hospital Ethics Committee and after obtaining the informed consent of all subjects or their guardians, children aged 16 years or younger who presented with suspected acute musculoskeletal infection (osteomyelitis or septic arthritis) at the emergency department during the study period (01 January 2012 to 31 December 2012) were enrolled.
The suspicion of infection was determined by the attending physician in the emergency department. Inclusion criteria included consent to take part in the study, signs of arthritis (swelling, local erythema, tenderness and pain), fever with limping, limping with refusal to bear weight and refusal to move a limb with or without focal tenderness.
Exclusion criteria included refusal to take part in the study, a clear history of trauma, limping without fever and limping without refusal to bear weight. Laboratory and other ancillary tests were not part of the inclusion criteria but were recorded in all patients.
Subjects and sampling
Laboratory tests (white blood cells (WBC) count, erythrocytes sedimentation rate (ESR), c-reactive protein (CRP) levels, blood cultures, synovial cultures, bone cultures) and imaging (bone scintigraphy, ultrasound, plain radiograph, MRI/CT) were conducted as deemed necessary by the attending physician from all children enrolled in the study. Synovial fluid aspirations were performed in all suspected infections involving joints. Bone aspiration was performed based on the consensus of the attending physician and the orthopaedic consultant on call.
Materials and methods
Blood and synovial fluid samples were collected using a 5 ml heparinized tube and were sent for 16S rDNA sequencing analysis in addition to routine cultures and gram staining. Bone samples were sent in saline media for 16S rDNA sequencing analysis.
For 16s rDNA analysis nucleic acids were extracted from the samples using QIAamp DNA mini Blood Mini Kit (QIAGEN, Germany) according to the manufacturer's instructions. Purified DNA was stored at -20°C until use.
The samples were tested for 16S rDNA with the Kapa SYBR® FAST qPCR Kit (KAPA Biosystems, Wilmington, Massachusetts) using a V3F+V6R primers mix. The polymerase chain reaction (PCR) mixture contained 6 µl of sample DNA within a total volume of 25 µl. Amplification was performed by a Rotor-Gene Q (QIAGEN), with an initial cycle of 30 seconds at 96.5°C, followed by 35 cycles of six seconds at 95°C, eight seconds at 56°C and 24 seconds at 72°C. An amplification product generated prior to the 35th cycle with one primer-specific peak was considered positive.
The PCR products of positive samples were sent to an external facility for sequencing. Sequencing results were analyzed with Geneious bioinformatics software (Biomatters, New Zealand) and compared with the National Center for Biotechnology Information world database for bacterial species (International Nucleotide Sequence Database Collaboration).
Standard laboratory procedures were performed in parallel for each sample and pathogen and served as the reference index in the present study. Both analytical sensitivity and analytical specificity of this method were evaluated. To assess analytical sensitivity serial dilutions of each individual pathogen were amplified. Specificity was demonstrated by the cross-amplification of each individual pair of primers targeting a specific pathogen.
Statistical analysis
Statistical analysis was performed using the IBM SPSS version 22.0 statistical package (SPSS Inc., Chicago, Illinois). McNemar's test was used and Kappa statistic was measured for interrater agreement of the parallel patient sample with standard pathogen specimens.
Results
During the study period, 41 children (18 boys and 23 girls) with suspected acute musculoskeletal infection were enrolled. The median age was 17 months (2 to 216).
A total of 14 patients were eventually diagnosed with septic arthritis, 17 with osteomyelitis, ten had other pathologies including cellulitis (four children), reactive arthritis/transient synovitis (three children), post-trauma (two children) and one child with chronic osteomyelitis.
Statistical analysis was performed only for patients with established diagnosis of osteoarticular infection.
Of the children with proved musculoskeletal infections, 18 patients had signs and symptoms consistent with lower extremities pathology while 11 patients had signs and symptoms consistent with upper extremities pathology. There were no cases of discitis or other spine pathology.
Leading presenting symptoms were: fever in 21 patients, refusal to use a limb or limping in 12 patients, pain in 12 patients and local signs of inflammation (fever, swelling and erythema) in eight patients.
Among children with proven osteoarticular infection, the mean WBC count was 17,400, the mean CRP level was 5.6 mg/dl and the mean ESR was 58 mm/hour.
In total, 27 of the patients underwent a bone scan which was positive for musculoskeletal infections in 15 (56%); 33 of the patients underwent ultrasound which was consistent with musculoskeletal infections in 28 (84%).
In total, 39 blood samples and 28 synovial fluid and bone samples for culture were obtained. Of these, 27 blood and 23 synovial fluid and bone samples underwent 16S rDNA PCR amplification; 17 samples were not analyzed by PCR due to technical difficulties.
A positive blood culture was found in six out of 31 proven cases of osteoarticular infections (19.4%) with methicillin-susceptible Staphylococcus (S.) aureus (MSSA) being the most commonly isolated bacterium (3/6, 50%). In contrast, positive blood 16S rDNA PCR results were found in 5/27 cases (19%), all with negative reciprocal blood cultures. Further, all positive blood 16S rDNA PCR results consisted of bacteria that are not common pathogens in musculoskeletal infections (Table 1) and were considered contaminants rather than evidence of pathogenic bacteria.
Bacterial isolates in blood polymerase chain reaction (PCR) and culture

MSSA, methicillin-susceptible Staphylococcus aureus; S. pneumoniae, Streptococcus pneumoniae
uncommon pathogens in musculoskeletal infections
A positive synovial fluid culture was found in six out of 14 proven cases of septic arthritis (42.9%) with Kingella (K.) kingae found in 3/6 (50%), MSSA was identified in 2/6 (33%) and S. pneumoniae was detected in 1/6 (17%) cases.
Using the 16S rDNA PCR method, the rate of positive results in synovial fluid was higher with detection in 12/14 (87.5%) samples. K. kingae was the most commonly identified bacterium (5/12 cases, 42%) using this method, followed by MSSA (4/12, 33%) and S. pneumoniae (1/12, 8%).
Of the 12 synovial fluid samples determined to be positive using 16S rDNA PCR, four were also positive in synovial fluid cultures. Significantly, eight (35%) synovial fluid PCR samples were positive despite a negative culture (Fig. 1).
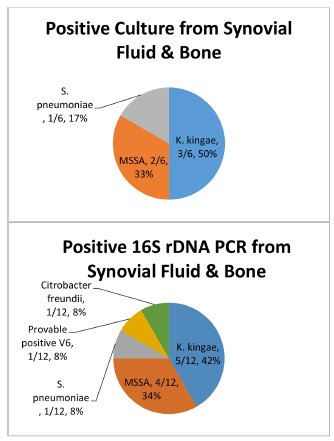
Relative bacterial isolates in synovial fluid polymerase chain reaction (PCR) versus culture (ribosomal DNA, Rdna; MSSA, methicillin-susceptible Staphylococcus aureus; K. kingae, Kingella kingae; S. pneumoniae, Streptococcus pneumonia; Provable Positive V6, insufficient information for identification of exact bacterial genus).
In four synovial fluid samples and one bone sample (from three children) collected after the initiation of antibiotic therapy, pathogens were detected by16S rDNA PCR. In all matching synovial fluid and bone cultures, no growth was detected after antibiotic treatment had been started.
In the case of the synovial fluid samples, antibiotic treatment was started two and three days prior to the arthrocentesis; in the case of the bone cyst aspiration, antibiotic treatment was started five days prior to aspiration.
A strong correlation was found between the presence of fever upon admission and microbial detection in synovial cultures (p = 0.017), synovial 16S rDNA PCR (p = 0.014) and blood cultures (p = 0.028). Similarly, a significant correlation between pathologic finding on bone scan and a positive 16S rDNA PCR result in synovial fluid samples (p = 0.009).
Discussion
The 16S rDNA PCR analysis method is an increasingly popular method for detection of bacterial pathogens. 7 Our study distinguished between bacterial detection in cultured blood, bone and synovial fluid samples as compared with detection rates using 16S rDNA PCR technology. To the best of our knowledge our study is the first to assess the yield of 16S rDNA PCR in blood samples in such infections.
Our results support those of previous studies that found high rates of bacterial detection using 16S rDNA PCR identification in synovial fluid.8,9 However, microbial identification in blood specimens using 16S rDNA PCR relative to culture did not yield a greater number of positive results. MSSA was the most frequently detected pathogen in blood cultures.
To the best of our knowledge no previous data has been published concerning the yield of bacterial detection using 16S rDNA PCR in blood from children with musculoskeletal infection, though studies assessing the use of 16S rDNA PCR in comparison with blood cultures in neonatal infection showed a 9.88% increase in the yield of pathogen detection using 16S rDNA PCR. 10
All 16S rDNA PCR products obtained from blood specimens in our study were eventually regarded as contaminants. One possible explanation for this is the technical difficulty surrounding the segregation of bacterial DNA from host DNA, especially in the early stages of infection when the number of the bacterial copies is low. 11
The yield of positive blood cultures was relatively low, 6/31 (19.4%) in this study, compared with that reported in the literature (30% to 50%), though other studies reported positive blood culture rate of only 9% to 20% in blood. 12
Our inclusion criteria were based on clinical assessment. Accordingly, over-diagnosis is a possible explanation for the low yield of positive blood cultures in our study. In order to minimize this effect, we included only established cases of osteoarticular infection, still resulting with a relatively low yield. Another explanation is that the clinical impression of a musculoskeletal infection may occur at a time when the bacterial load is still low. The strong association between the presence of fever and the detection of positive blood cultures supports this hypothesis.
Reports concerning the successful identification of bacteria after initiation of antibiotic treatment in the field of musculoskeletal infections have been few and anecdotal. However, in a study assessing the diagnosis of endocarditis based on PCR from culture-negative cardiac-valve samples, bacteria were identified in up to 60% of patients after the initiation of antibiotic treatment. 13
Although only five samples in our study were tested after the initiation of antimicrobial therapy (due either to administration prior to presentation at the hospital or in cases when treatment began before a second joint aspiration took place and sample fluid was obtained), our study suggests that synovial specimen remain positive for 16S rDNA PCR after initiation of antibiotic treatment even when microbial cultures did not result in bacterial growth even after several days of treatment.
Given the importance of a positive PCR product even after initiation of antibiotic therapy, further studies are needed to assess the overall yield of 16S rDNA PCR where the yield from cultures is very low.
The generalizability of this study was limited by its small cohort which, although not unique among similar studies 14 qualifies the statistical analysis. Another limitation was that subjects were recruited based on clinical evaluation without the use of ancillary tests, or previously published criteria such as Morrey's criteria, a limitation that might have contributed to the lower-than-expected yield of cultures and molecular tests.
As molecular technology is becoming more available, turn-around time for those tests is getting shorter (up to 48 hours) and costs are getting lower towards the point similar to traditional cultures.
The results of this study support the use of 16S rDNA PCR to detect bacteria in synovial fluids in untreated children as well as after the initiation of antimicrobial therapy.
The use of 16S rDNA PCR failed to demonstrate a greater number of positive results over traditional cultures in blood specimens.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Informed consent was obtained from all individual participants included in the study.