
Abstract
Correct diagnosis and treatment of septic arthritis (SA) are essential to achieve satisfactory results and avoid lifelong consequences. Diagnosing septic arthritis is not always easy, which is why new biomarkers have been sought. Another difficulty in diagnosis is the increase in septic arthritis due to Kingella Kingae, which does not show the same signs and symptoms as classic Staphylococcus aureus infections. Increasingly, magnetic resonance imaging plays a more fundamental role in diagnosing septic arthritis, and many studies are focused on this line, especially for the study of associated pathologies. Numerous studies have been published on less invasive treatments for septic arthritis, although the evidence suggests that the results should be taken cautiously. Although most of the published studies focus on the hip and knee, there have also been recent publications on SA in the upper limb, foot, and ankle. Finally, the literature also pays attention to SA in young children due to its different etiology and the greater difficulties in its diagnosis.
Introduction
Even though the incidence of septic arthritis (SA) in affluent countries has fallen significantly, it is still an important cause of morbidity and lasting sequelae. The estimated incidence of SA in Europe is between 2 and 7 per 100,000 children, 1 and most commonly involves hip and knee joints. Making a correct diagnosis followed by early and appropriate treatment is key to avoiding long-term sequelae that can be very disabling.
Diagnosis
The diagnosis of SA is not always easy, and recent works have been directed toward identifying those signs and symptoms that could be more relevant for the diagnosis and management of this condition.
Since Kocher’s original work 2 established the criteria for differentiation between hip SA and irritable hip, there have been many attempts to find better parameters to determine a diagnostic of certitude. While the five Modified Kocher-Caird criteria 3 predictive of SA are widely used, difficulties in establishing a diagnosis are well reflected in a recent review of monoarthritis in children below 6 years of age, where clinical and biological parameters did not allow differentiation between an infectious and inflammatory etiology. In this recent work, 95% of patients with juvenile idiopathic arthritis (JIA), 100% of SA, and 95.4% of unknown arthritis (UA) received antibiotics, while 66.7% of JIA patients, 79.6% of SA, and 71.1% of UA eventually underwent surgery. 4
The Kocher criteria have also been shown to be of limited value for predicting knee SA in general, particularly in infections with Kingella Kingae. 5 The most valuable parameter in predicting knee SA appears to be an inability to weight bear combined with an elevated C-reactive protein (CRP), which has an 89.7% positive predictive value for the septic knee: the inability to weight bear is the strongest independent risk factor for a septic knee. 6
Finding parameters to establish a diagnosis is not an easy task. Some systematic reports have shown that the main problem is that the overall quality of the current literature is relatively low. The definitions and cutoff values used for the clinical, laboratory, and imaging findings vary between series, making comparisons difficult. 7
Serological markers have value in identifying the severity of the infection, but many times fail to reflect the course of the infection because of the immaturity of the immunological system, characteristics of the infecting organism, or confounding factors such as patients reaching the hospital after having already received antibiotic treatment. These difficulties have led to the search for new biomarkers more sensitive to identify the diagnosis and the evolution of musculoskeletal infections. Alpha defensin, which is an innate part of the immune system and plays an important role in our defense against infection, has shown to be much superior to other biological markers, with a sensitivity and specificity of 97% and 96%, respectively, and the added advantage is that its values are not affected by antibiotic use. 8 Alpha defensin has recently been approved by the Food and Drug Administration (FDA) for use in periprosthetic infections. However, it may yield false-positive results in the presence of metallosis or false-negative results in the presence of low-virulence organisms. Furthermore, a fluid or tissue sample of the affected joint is needed, so while this marker is non-viable as a predictor of infection, it is useful for confirmation of the diagnosis. 9
Altogether 50% of infections have no pathogen identified, and diagnosis cannot be confirmed. Kingella kingae infection reflects very well the problems associated with establishing a diagnosis of SA. Kingella kingae is a Gram-negative coccobacilli, found to be the main organism responsible for bone infection in children aged between 6 and 48 months. K. kingae SA is characterized by a mild clinical presentation and a moderate biological inflammatory response to infection. Theoretically, these children do not require invasive surgical procedures and a shorter antibiotic treatment leads to a favorable prognosis. 10 Unfortunately, clinical differentiation between infections by Kingella or by Staphylococcus aureus, which requires much more aggressive treatment, is impossible to establish clinically or with laboratory tests. 11 In a study of 198 patients with SA with 37 cases associated with acute osteomyelitis (AO), it was found that children with SA and no fever, low CRP, and negative culture for Staphylococcus aureus respond simply to a course of combined intravenous (IV) and oral antibiotics, with no other investigations or invasive procedures being necessary. 12
Kingella kingae is present in the oropharynx after 6 months of life and gradually increases to reach a prevalence of 10%–12% among children at 24 months, decreasing thereafter. It is rarely detected by Gram stain due to its low bacterial concentration, and blood cultures are of limited help in its diagnosis, as it appears that the bacteremia phase is very short and cultures are rarely positive once the signs of arthritis have already appeared. To improve positive culture rates of synovial fluid for Kingella, adequate blood-agar or chocolate-agar plates should be used. Due to these inherent difficulties, the most reliable diagnostic aid is a PCR, which combined with nucleic acid amplification tests (NAATs) makes the test more specific increasing grossly the power of detection. The negative predictive value of specific DNA sequences virtually excludes the bacterium as the cause of infection. However, the problem with NAATs is that they cannot replace cultures, as NAATs give no information about the strain and its antibiotic sensitivity. 13
When no joint fluid is available for NAATs, and in the presence of arthritis in a group risk, an oropharyngeal specimen could be obtained and, if the specific molecular assay is positive for Kingella, the patient could be treated as a confirmed infection.7,10
While PCR has proven efficacy for Kingella kingae, it has not been developed with similar success for Staphylococcus aureus, 8 so we need new techniques that allow us a more reliable diagnosis. One of the emerging techniques is whole-genome sequencing, which focuses on the whole genome, and a branch of this is metagenomic next-generation sequencing (mNGS), this a novel cell-free DNA technology and able to detect any non-human sequence of DNA that could be considered the responsible pathogen. It can detect about 1400 species in a 1- to 3-day period and has the advantage of not only determining the causing agent but also identifying the genes responsible for pathogen resistance. Needing a very small sample is another perk for small children, and even if the patient has been started on antibiotics, it does not decrease its ability to detect the responsible pathogen. Finally, this test may allow the start of antibiotic treatment as soon as the child is seen and the diagnosis is suspected, potentially, diminishing the harm to the joint tissues.10,13
Imaging
The criteria for imaging in SA remains controversial, and the exact role of magnetic resonance imaging (MRI) is still to be defined. Although MRI may be very specific in detecting SA and the associated AO, there are no clear protocols for its use (Figure 1). A recent consensus guideline published by the BSCOS (British Society of Children Orthopaedic Surgery) concluded that all children should have an X-ray of the suspected bone or joint involved and MRI should be the gold standard second-line imaging, leaving ultrasound reserved for those cases where obtaining a MRI promptly is not possible. 14 However, MRI is not readily available in many institutions and often requires general anesthesia in young children, factors that need to be considered in the management and decision-making concerning these patients.
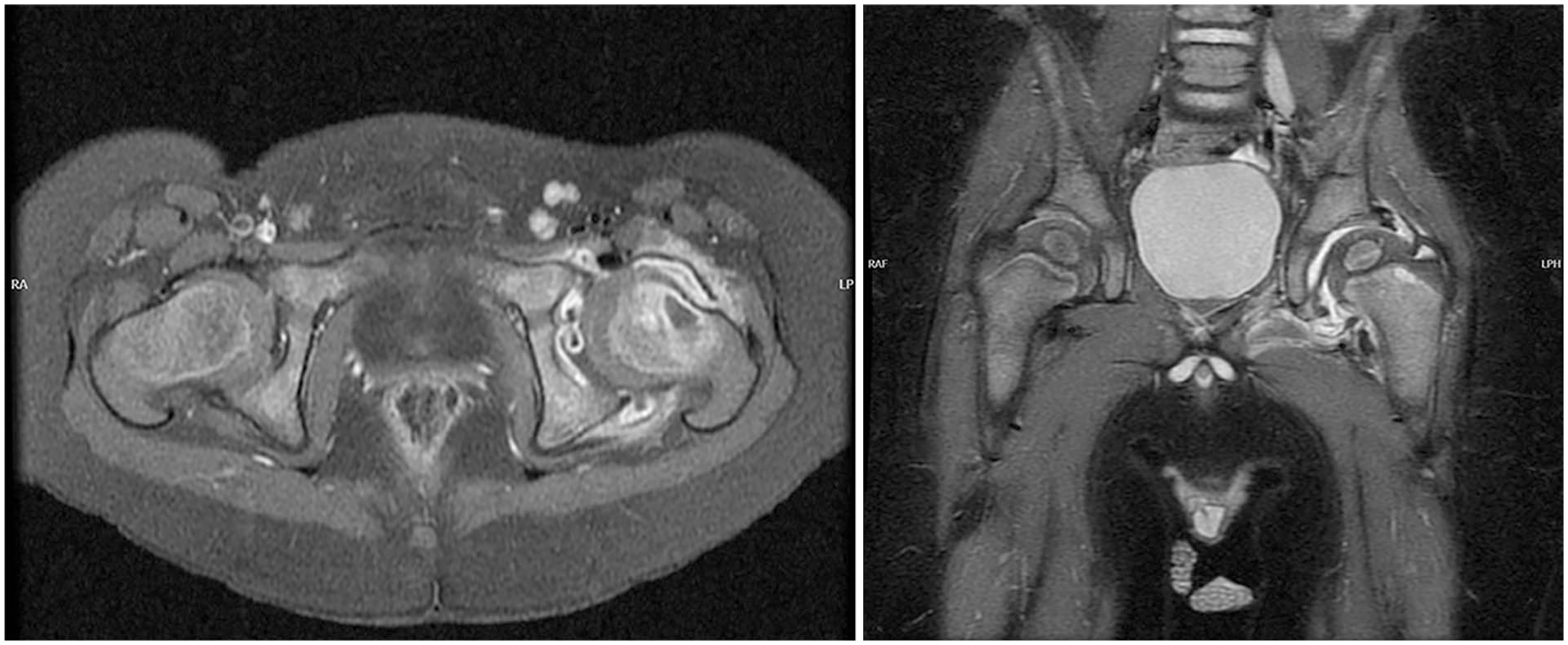
MRI pictures (STIR sequence) show hip septic arthritis associated with osteomyelitis of the femoral neck.
A recent study found that the combination of hip effusion on ultrasound and two or more Kocher criteria may lead to unnecessary surgery in a high percentage of patients. When MRI was added to the diagnostic workup of these patients, it was found that only about 35% of patients with ultrasound (US) positive and Kocher criteria had hip SA. The use of MRI in these patients could have saved unnecessary surgery in 65% of the cases. 15
MRI is an important tool to help with diagnosis. However, sometimes the differential diagnosis between toxic synovitis (TS) and SA may be extremely difficult. The changes seen in these entities are highly dependent on evolution over time, and assessment should take into account whether the patients were early presenters (<2 days) or late presenters (>2 days). In the early group contralateral hip effusion and the late presenter’s group, the absence of enhancement of signal in soft tissues was the most significant predictor of TS (Figure 2). 16

STIR sequence MRI shows an isolated MRI with intraarticular effusion and increased uptake of the sin.
A meta-analysis concluded that the most specific finding for hip SA in MRI is the bone marrow changes, followed by the femoral head changes, while the most sensitive MRI findings for SA were synovial enhancement, conversely, the femoral head changes are the less sensitive as these changes need time to occur. 17 Also, worth keeping in mind in cases where contrast-enhanced gadolinium cannot be used, that the diffusion-weighted (DWI) MRI sequences may be a good alternative, as it has a high ability to detect abscesses, its drawback is, its limited value to evaluate chondroepiphyseal involvement of the femoral head, especially in children below age 30 months. 18
SA and associated pathology
One issue of debate in SA is the frequency of associated osteomyelitis and other musculoskeletal infections, and their role in the prognosis and management. Controversy exists about the criteria that should lead to the suspicion, and what protocols should be implemented to detect it.
Despite the fact that hip SA associated with AO has a similar clinical picture to isolated hip SA, treatment and prognosis are completely different to the point that certain authors consider them as distinct entities and some studies suggest that AO is the primary disease process that potentiates osteonecrosis and joint destruction. 19 In general patients with associated AO are older, have a higher initial CRP, a higher rate of bacteremia, and are more likely to be Staphylococcus aureus infections. Others have found that when pain is present for longer than 4 days and there is a positive joint culture, there is a significant risk of concomitant AO.20,21
MRI may help in the diagnosis of associated AO, but most of the time, it is not performed routinely before hip irrigation, and there is no consensus for its preoperative indication. Griswold studied the implementation of a preoperative MRI protocol in patients with musculoskeletal infection: 53 patients with osteoarticular infection were compared to 40 cases in whom the preoperative MRI protocol was implemented. In the preoperative MRI group, the number of repeated and unplanned surgeries was significantly reduced and there was a decrease in the overall length of stay because the MRI detected concomitant AO with subperiosteal abscesses and pyomyositis with abscesses, allowing for adequate treatment at first surgery. 22
The association of SA with osteomyelitis is not only common at the level of the hip but is also encountered in other joints.23,24
Treatment
A systematic review of different techniques of treatment of hip SA showed that the less invasive the techniques were, the higher the risk of requiring a repeated procedure. On the other hand, they found that arthrotomy may have inferior outcomes in the long term. When hips were treated with arthrocentesis, a repeat procedure was needed in 15% of cases, and if no drain was left behind, the need for additional arthrocentesis increased still further up to 71%. When arthroscopy was the method of choice, only those treated without in situ drainage needed additional arthroscopy (14%). Finally, in the arthrotomy group, only 3% required additional surgery. Clinical and radiological results were superior in the arthrocentesis and arthroscopy group with only 4% and 9%, respectively having radiographic sequelae. These findings contrast with the arthrotomy group where 8% had a poor clinical outcome, and up to 30% presented radiological changes. 25 A possible explanation for these differences could be the characteristics of the patients treated, while arthrocentesis and arthroscopy only include patients with short presenting symptoms, arthrotomy also included patients who presented late; therefore, these results should be interpreted with caution. In a similar study, Caldaci et al. 26 found that 70% of patients treated with arthrocentesis required an additional arthrocentesis and 15% eventually required an arthrotomy. Of those treated by arthroscopy, 12% needed an additional procedure, while among those treated by arthrotomy only 3% precise further procedures. Remarkably, in this study, the clinical and radiological sequelae were quite similar between all the groups.
One of the theoretical disadvantages of arthrotomy over arthrocentesis is the surgical aggression and leaving a scar behind. This issue has recently been analyzed, and the authors concluded that although significant differences existed in the perception of the scar, the scar in itself was not an important issue for the patients. 27
The adequacy of the drainage techniques for the knee joint has also been studied. A systematic review of 279 knee SA, including 171 (64%) treated by arthrocentesis, 96 by arthroscopy (34%), and 12 (7%) by arthrotomy, found that repeated drainage was needed in 35% of arthrocentesis (including 13 arthrotomies), 4% of arthroscopies, and 17% of arthrotomies. The functional outcomes show that up to 15% of the arthrocentesis group were left with some functional limitation, while 10% of patients with arthrotomy had limitations. Bone sequelae were present in 25% of patients in both the arthrocentesis and the arthrotomy group. The arthroscopy group showed the best results with no permanent radiological changes. 28 However, Caldaci et al. 26 using the same methodical found that midterm bone changes were more common in the arthrocentesis and arthroscopy group.
Nevertheless, the reasons for these differences, as pointed out by Royer et al., 29 may not be related to the technique of drainage. The need for a second procedure may have more to do with factors such as associated multiple infections, the virulence of the germs, and the presence of a positive blood culture. 26
Unfortunately, the limitations of the treatment literature are similar to those found in diagnosis, as most studies are based on poor retrospective reviews, with short follow-ups, and rarely reporting the delay of treatment. Therefore, on this ground, comparisons are unreliable. Advancements in the field of SA are going to require the application of more unified criteria to make information comparable. The use of such implementations may ease the sharing of information but also may impact the welfare of our patients. A study 30 showed that by introducing guidance for the use of central intravenous lines, the incidence decreased which also, consequently, reduced the global number of sedations required.
Unusual locations
Most of the literature on SA is focused on the hip and knee as the most common locations.
Despite its rarity, upper limb SA should be suspected in any child with persistent upper limb pain and functional limitation, especially when associated with systemic symptomatology. On a search of over 18 major institutions, the authors were only able to identify 68 patients, representing about 10% of all SA, and about 1 single case per institution per year. 23 The most common infected joint was the elbow (53%) followed closely by the shoulder (41%). Patients with shoulder SA were found to be younger (1 year) than those with elbow involvement (4.6 years). The rate of positive blood culture in these patients was 34%, while samples taken during surgery yielded a positive result in 72% of patients. The most common organism grown at the shoulder was Streptococcus, while at the elbow was Staphylococcus non-methicillin resistant, and as much as 46% of these patients presented an associated adjacent musculoskeletal infection or persistent bacteremia. Surgical debridement was the treatment most used, with some patients requiring repeated debridement. The outcome was generally good with 3 patients having complications secondary to avascular necrosis (1 at shoulder and 2 at elbow) and 1 patient sustaining a humerus pathological fracture.
The best method for drainage in upper limb SA is also a matter of controversy. In a systematic review, no conclusive differences between treatment with aspiration or arthrotomy were found, 31 but again the authors concluded that due to the low quality of the studies, it was impossible to reach any definitive conclusions.
Another unusual location in children is the foot and ankle. A report of 23 children with foot and ankle musculoskeletal infections found 9 SA, 8 of them located at the ankle joint and 1 at the cuneiform-cuboid joint. The average age of patients was 8.5 years, and nearly half of them had no fever on arrival. Cultures were negative in 3 patients, while Staphylococcus aureus followed by Streptococcus was the most common infecting organism. Two of the ankle SA presented with associated distal tibial AO and both ended with spontaneous ankle joint fusion. 24
SA in young children
While SA beyond 6 months is commonly produced by Kingella kingae, it normally does not affect younger patients. In a series from New Zealand, 11 cases of SA in children below 3 months of age, they found that Streptococcus agalactiae was the most commonly responsible organism, representing nearly 50%, followed by Staphylococcus aureus in 36% of cases. In patients between the ages of 3 and 12 months, Streptococcus pneumoniae was the most frequent pathogen. 32
When we deal with SA in neonates, the diagnosis may be difficult, due to the vague signs of infection and biological biomarkers inside the normal range. Therefore, most protocols include methods of evaluation assessing the presence of fluid inside the joint and the use of ultrasound-guided aspiration to confirm diagnosis. However, a recent report warns about the possibility of obtaining false-negative results despite the presence of active infection. 33
Conclusions
The criteria of Kocher applied to patients susceptible to having a Kingella infection should be used cautiously, as they are more unreliable than in other types of infections. New infection markers, such as alfa defensin, or technologies, such as mNGS, may prove of value in doubtful cases, even if already under antibiotic treatment.
Identifying SA with associated osteomyelitis is paramount as both entities seem to be different diseases with different prognoses, even if the infecting organism is the same. In this context, MRI is emerging as the gold standard for imaging diagnosis in SA, regardless of whether bone infection is associated.
While surgery has been considered the cornerstone of treatment for hip SA, the literature has failed to confirm such an approach; larger and better-quality studies would be needed to define the role of each therapeutic resource, although there is a trend toward less aggressive techniques.
Although most joint infections happen in the knee and hip, they may also happen in other joints; joint infections may also present outside the typical age range, such as in neonates. Atypical infections, either by location or age, have a much lower incidence and are frequently produced by different infecting organisms; the explanations for this behavior are poorly understood.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241311302 – Supplemental material for Diagnosis and management of septic arthritis. A current concepts review
Supplemental material, sj-pdf-1-cho-10.1177_18632521241311302 for Diagnosis and management of septic arthritis. A current concepts review by Ignacio Sanpera, Marta Salom, Cristina Alves and Deborah Eastwood in Journal of Children’s Orthopaedics
Footnotes
Author contributions
All the authors have contributed to the elaboration of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work has not been approved by an ethical board committee because it is a Current Concept Review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.