
Abstract
Background:
Idiopathic clubfoot is a congenital disorder necessitating time-sensitive treatment. Delayed application of the Ponseti method may result in poorer outcomes. Adverse social determinants of health, as measured with the Childhood Opportunity Index version 3.0, hinder access to care. This study aimed to determine the association between Childhood Opportunity Index, insurance status, and treatment disparities for patients with idiopathic clubfoot.
Methods:
This retrospective cohort study included patients with idiopathic clubfoot who underwent Ponseti treatment at an urban tertiary care orthopedic hospital between October 2004 and September 2022. Patients presenting for care before 6 months of age and with a minimum 2-year follow-up were included. A threshold Childhood Opportunity Index value of 60.0 categorized patients into low (<60.0) and high (≥60.0) cohorts. Clinical and treatment/outcome variables were compared.
Results:
A total of 156 patients (mean follow-up 5.1 ± 2.5 years) merited inclusion: 31 (20%) with Childhood Opportunity Index <60 and 125 (80%) with Childhood Opportunity Index ≥60. Patients with low Childhood Opportunity Index presented at older ages (18 ± 23 versus 11 ± 10 days, p = 0.03) and had fewer prenatal orthopedic evaluations (42% versus 64%, p = 0.03). Recurrence and necessity for further treatment were similar (p > 0.05). Patients with public insurance presented at older ages (28 ± 31 versus 10 ± 9 days, p < 0.01) and were less likely to undergo prenatal consultation (13% versus 65%, p < 0.01). Black/Hispanic patients were more likely to experience a recurrence (odds ratio 6.4, 95% confidence interval 1.2–35.4, p = 0.03), whereas patients who had a prenatal orthopedic evaluation were less likely to experience a recurrence (odds ratio 0.3, 95% confidence interval 0.1–0.9, p = 0.03).
Conclusions:
Patients with idiopathic clubfoot and low Childhood Opportunity Index/public insurance experienced delayed presentation to care and fewer prenatal orthopedic consultations. However, low Childhood Opportunity Index and public insurance status were not associated with adverse treatment outcomes. Clubfoot specialists remain a critical component of the multidisciplinary prenatal team, as orthopedic consultations served as a protective factor against recurrence. These findings contribute to the existing literature by highlighting discrepancies in the care for patients with adverse social determinants of health.
Level of evidence:
Level III.
Introduction
An increasing emphasis is being placed on understanding the interplay of social determinants of health (SDOH) and orthopedic care. SDOH represent the overarching non-medical factors that influence health outcomes and can be understood as five domains from the Healthy People 2030 Initiative: economic stability, education, health and health care, neighborhood and the built environment, and social and community context. 1 Adult and pediatric orthopedic patients with unfavorable SDOH—including lower socioeconomic status (SES), minority race, and non-English primary language—experience adverse outcomes, including greater rates of non-home discharge, readmission, medical and surgical complications, revision surgeries, and extraneous healthcare utilization.2–6 The Childhood Opportunity Index (COI) version 3.0 is a validated composite assessment that captures numerous facets of SDOH7,8 including education, health and environment, and socioeconomic domains, and outperforms other leading composite neighborhood indices such as the Area Deprivation Index, the Social Vulnerability Index, and COI version 2.0, in terms of predictive and equity validity. 9 Given the association of adverse SDOH and delays to medical care, the COI is useful to evaluate disparities in access to care in pediatric disorders that require timely treatment.
Affecting 1–2/1000 births, idiopathic congenital clubfoot, or congenital talipes equinovarus, is a musculoskeletal birth defect that necessitates time-sensitive treatment.10,11 The Ponseti method is the current gold-standard treatment. 12 It consists of a serial cast phase, possible percutaneous Achilles tenotomy and a post-corrective bracing phase of 2–5 years to prevent relapse. Although the Ponseti method has shown efficacy even in the setting of delayed presentation, early management is recommended when the foot is most flexible as a measure to avoid surgical intervention including13–15 tibialis anterior tendon transfers, Achilles lengthening, or other soft tissue releases,16,17 which may be necessary due to increased rigidity secondary to bony changes and soft tissue contractures.18,19 Considering the detrimental effects of delayed treatment, it is imperative to identify factors that hinder access to care for clubfoot, including non-medical factors related to SDOH. Previous reports have investigated the effects of COI and insurance status on limited outcome variables, including missed clinic visits, transportation access, and recurrence of clubfoot.20,21 There remains a paucity of literature that comprehensively evaluates the effects of both COI and insurance status on variables pertaining to the full timeline of clubfoot treatment, from prenatal evaluation that may play a role in preparing a family for several years of treatment to post-management.
This study aimed to determine the association between COI and insurance status with treatment disparities for patients with idiopathic clubfoot. We hypothesized that patients with lower COI and public insurance would present at older ages and have a higher rate of recurrence. We also hypothesized that families with lower COI and public insurance would be less likely to receive prenatal counseling and evaluation.
Materials and methods
Patient selection
Following institutional review board approval (2023-0453-MS5), a retrospective query of all patients with idiopathic clubfoot who underwent treatment with the Ponseti method at a single urban tertiary care orthopedic hospital between October 2004 and September 2022 was conducted using International Classification of Diseases—9th and 10th Edition diagnosis codes: 736.7X, 754.5X, 754.6X, 754.7X, M21.54X, Q66.0X (Figure 1). These dates were chosen to ensure that all patients had a minimum of 2-year clinical follow-up. Additionally, only patients with idiopathic clubfoot who presented to care before the age of 6 months (180 days) were included. This ensured that these patients received Ponseti casting as the initial treatment modality, as is standard of care in our institution. This cutoff is consistent with those utilized in prior clubfoot literature. In some treatment centers, patients older than 6 months of age are less likely to undergo initial casting if they are ambulating, possibly indicating initial operative treatment.18,22,23 Patients with insufficient follow-up and insufficient data such as incomplete demographic (e.g. zip code), clinical characteristics (e.g. physical exam), missing treatment notes, or a later diagnosis of complex clubfoot were excluded (Figure 1). All patients were treated by one of four (DMS, JSB, ERD, SMD) fellowship-trained pediatric orthopedic surgeons.
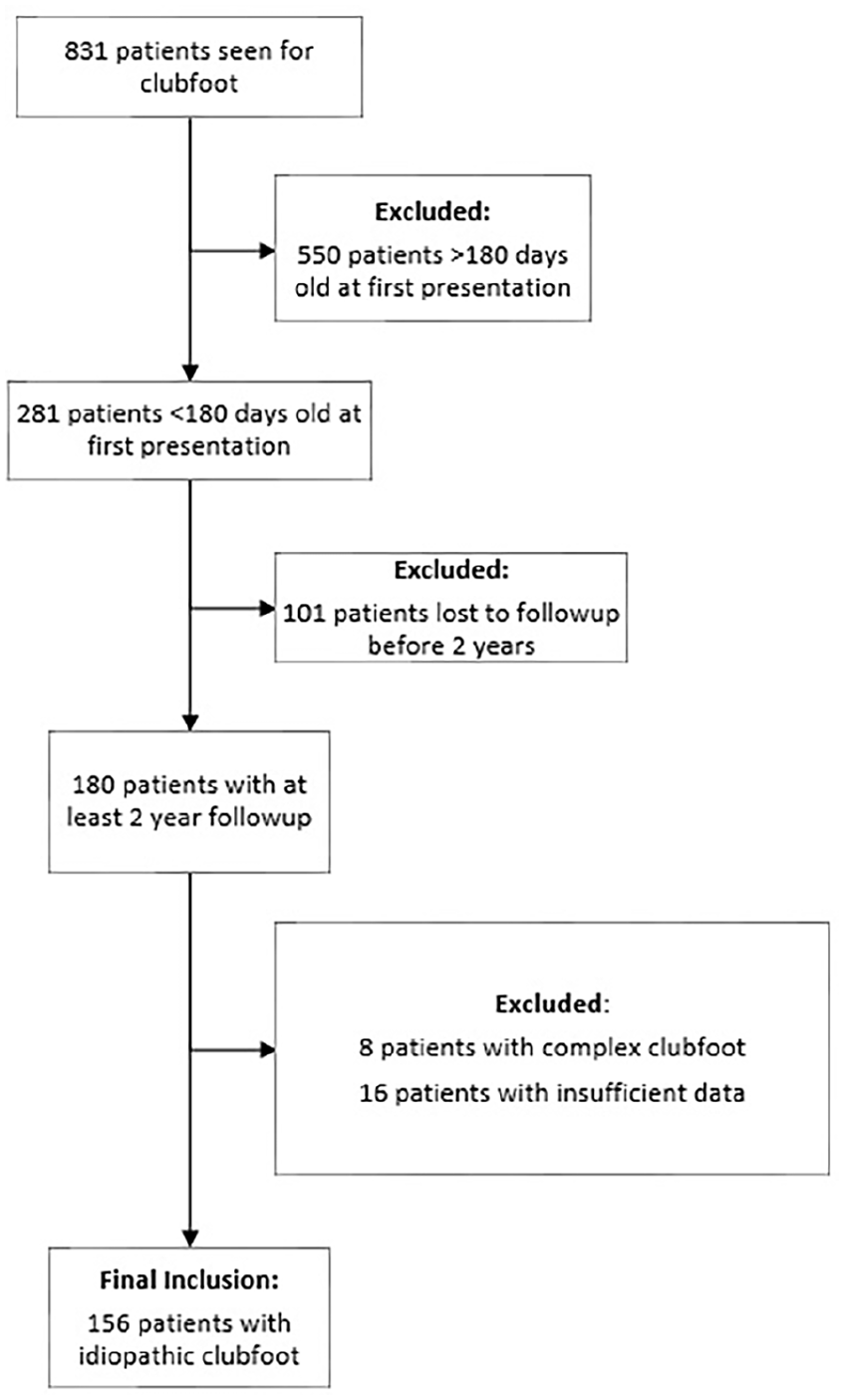
Flowchart of patient exclusions.
Treatment algorithm
The standard of care for initial clubfoot treatment at our institution aligns closely with the Ponseti method. Serial long leg Plaster of Paris casts are applied to patients weekly, or sooner if cast slippage or substantial soiling occurs. Casts are placed until all components of the deformity are clinically corrected. Persistent equinus is the typical indication for a percutaneous Achilles tenotomy. The final cast following tenotomy remains for 3 weeks and correction is confirmed upon its removal. Next, the FAO brace is applied. Patients are braced full-time for 23 h a day for 3 months, with follow-up visit at 1, 3, and 12 weeks after the initiation of bracing. After 3 months of full-time bracing, patients progress to part-time/nighttime wear for naps and nighttime, ~12 h/day. Bracing continues until the patient reaches 5 years of age. Brace compliance is disclosed by the caregiver(s), with instances of noncompliance typically being self-reported. Follow-ups during the part-time bracing phase occur at 6-month intervals until 1 year after brace removal. Typically, there is yearly follow-up into adolescence.
All patients in this study achieved initial correction. Recurrence was defined when one or more components of deformity and loss of plantigrade alignment were noted following initial correction. All relapsed, non-ambulatory patients underwent repeat casting and revision tenotomy as indicated. However, ambulatory patients with dynamic supination in swing phase and/or equinus typically underwent short leg casting followed by tibialis anterior tendon transfers and Achilles lengthening, if warranted. Additionally, cases of excessively stiff or resistive deformity in older children necessitated more invasive surgical intervention such as posteromedial release, gastrocsoleus recession, or osteotomies. Figure 2 displays a visual representation of the chronological treatment algorithm.
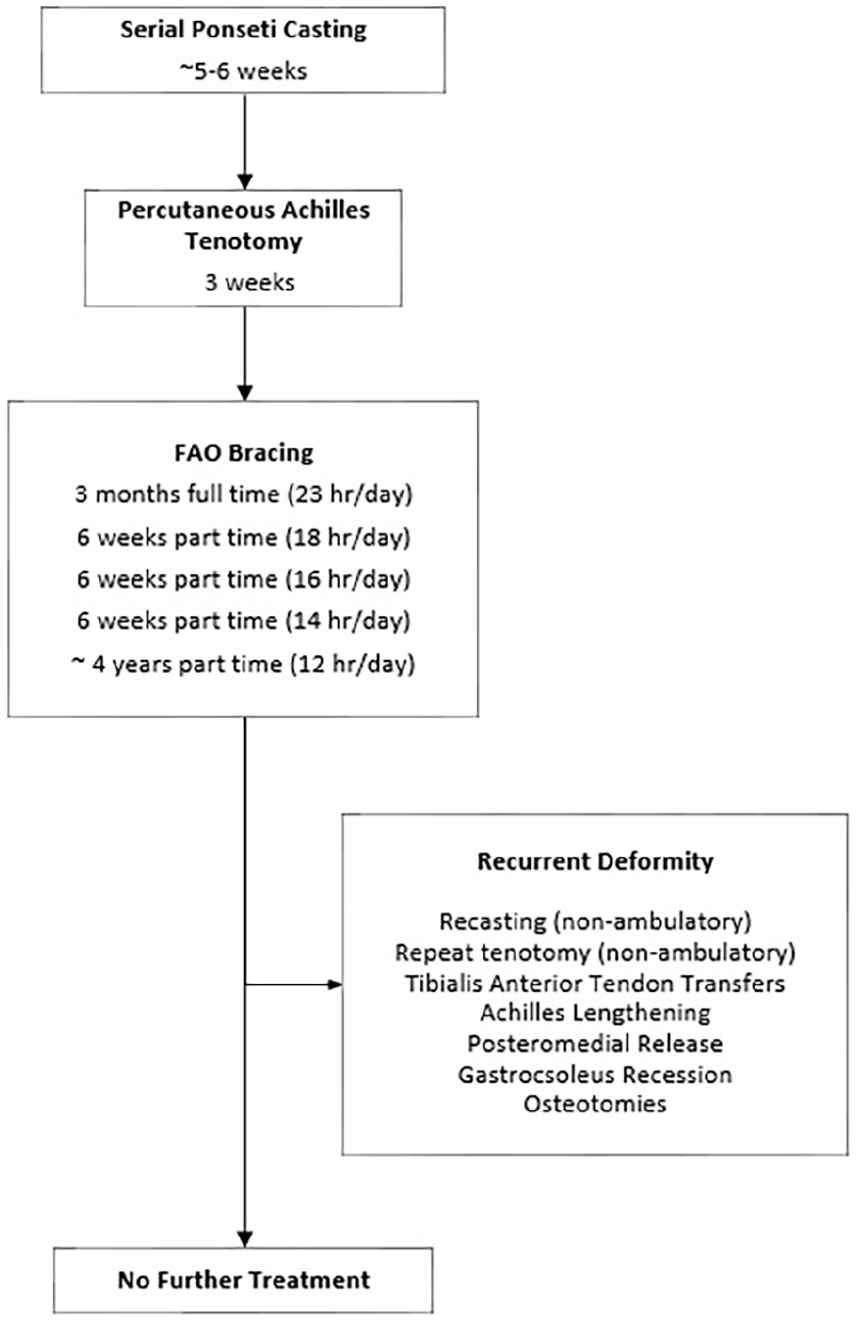
Flowchart of clubfoot treatment algorithm.
The COI version 3.0
COI was the primary risk factor for clubfoot treatment disparities evaluated in this study. The COI is a nationally available database that provides a validated composite measure of neighborhood features that captures variation of opportunity across the United States by utilizing 44 indicators in education, health and environment, and social and economic domains. 8 The COI is available in an overall index and in sub-scores for education (COI-ED), health and environment (COI-HE), and social and economic domains (COI-SE), as well as 14 additional subdomains. Reported on a percentile scale from 1 to 100, individual neighborhoods are divided into five ordered groups by percentile: “very low” (at or below the 20th percentile), “low” (above the 20th and at or below the 40th percentile), “moderate” (above the 40th and at or below the 60th percentile), “high” (above the 60th and at or below the 80th percentile), and “very high” (above the 80th percentile) opportunity. A threshold COI value of 60.0 was used to categorize patients into low (<60.0) and high (≥60.0) COI cohorts as defined by previous orthopedic studies.5,24
Outcomes of interest
Demographic variables of interest included age, sex, race, public insurance status, and ZIP code. Race was reported by the patient’s family and recorded as White, Black, Asian, Hispanic, and other. The patient’s ZIP code was linked to the corresponding COI overall score and COI-ED, COI-HE, COI-SE sub-scores. Clinical variables of interest included age at first presentation, laterality of clubfoot, birth weight, gestational age, vaginal or non-vaginal delivery, prenatal clubfoot screening and/or evaluation, family history of clubfoot (first or second degree), and associated clinical conditions. Pirani and Dimeglio scores at presentation were noted when available, with the higher score (i.e. more severe clubfoot) used for analysis in cases of bilateral clubfoot. Additionally, treatment parameters including the performance of an Achilles tenotomy, complications, and necessity and the type of further treatment (e.g. posteromedial release) were collected. The most involved treatment required for clubfoot recurrence—with the necessity of further treatment defined by the treating provider (e.g. tibialis anterior transfer for dynamic supination versus further casting for recurrence)—was specifically noted. Similarly, the most involved additional treatment for either foot was used for analysis in cases where both feet were affected.
Statistical analyses
A priori sample size estimation to detect a large effect size of 0.67 for age at presentation with an alpha = 0.05 and power = 0.80 determined that 27 patients in the “low COI” group and 55 patients in the “high COI” group would be required. Standard descriptive statistics were reported for demographic and clinical variables. Categorical variables were analyzed using chi-squared (χ2) or Fisher’s exact test, as appropriate. The Shapiro–Wilk test was used to evaluate normality of continuous variables. Continuous variables were analyzed using independent t-test or Mann–Whitney U test, as appropriate. A multivariable binary logistic regression was used to determine variables associated with clubfoot recurrence and was reported as odds ratio (OR) with 95% confidence intervals (CIs). Only demographic variables (age at presentation and sex) and variables achieving p < 0.1 in univariable analysis were selected for the multivariable regression model. A p < 0.05 was designated as the threshold for statistical significance. All analyses were conducted in SPSS (IBM Corporation, Armonk, NY, USA).
Results
Of 831 patients who were seen for clubfoot at our institution across the 18-year study period, 550 patients were excluded for presenting at more than 6 months of age, 101 were excluded due to loss to follow-up, 16 were excluded for insufficient data, and eight were excluded for complex clubfoot (Figure 1). A total of 156 patients with idiopathic clubfoot were included in this study. This consisted of 31 (20%) patients with low COI and 125 (80%) with high COI (Table 1). Mean COI was 37 ± 16 in the low COI group and 90 ± 10 in the high COI group (p < 0.01). All three COI sub-scores (COI-SE, COI-HE, and COI-ED) were lower in the low COI group. There were no differences in sex, race, or clubfoot laterality between cohorts (p > 0.05). Mean follow up was 4.7 ± 2.2 and 5.2 ± 2.5 years for the low and high COI groups, respectively (p > 0.05). Patients with low COI presented at an older age than patients with high COI (18 ± 23 versus 11 ± 10 days, p = 0.03). Mean birth weight, gestational age, method of delivery, family history of clubfoot, and presence of associated disorders were similar between groups (Table 2, p > 0.05). The low COI group was less likely to receive a prenatal evaluation for clubfoot with an orthopedic surgeon (42% versus 64%, p = 0.03). When assessing clubfoot severity on initial presentation, there was no difference in mean Dimeglio scale between groups (Table 3). Pirani scale scores were higher in the group of patients with a COI ≥60 (5.1 ± 0.9 versus 4.6 ± 1.2, p = 0.04). The proportion of patients needing an Achilles tenotomy and time to initial reported correction were similar in both groups. Clubfoot recurrence and necessity for further treatment were also not different when sorting cohorts above, at, or below the 60th COI percentile.
Demographics.
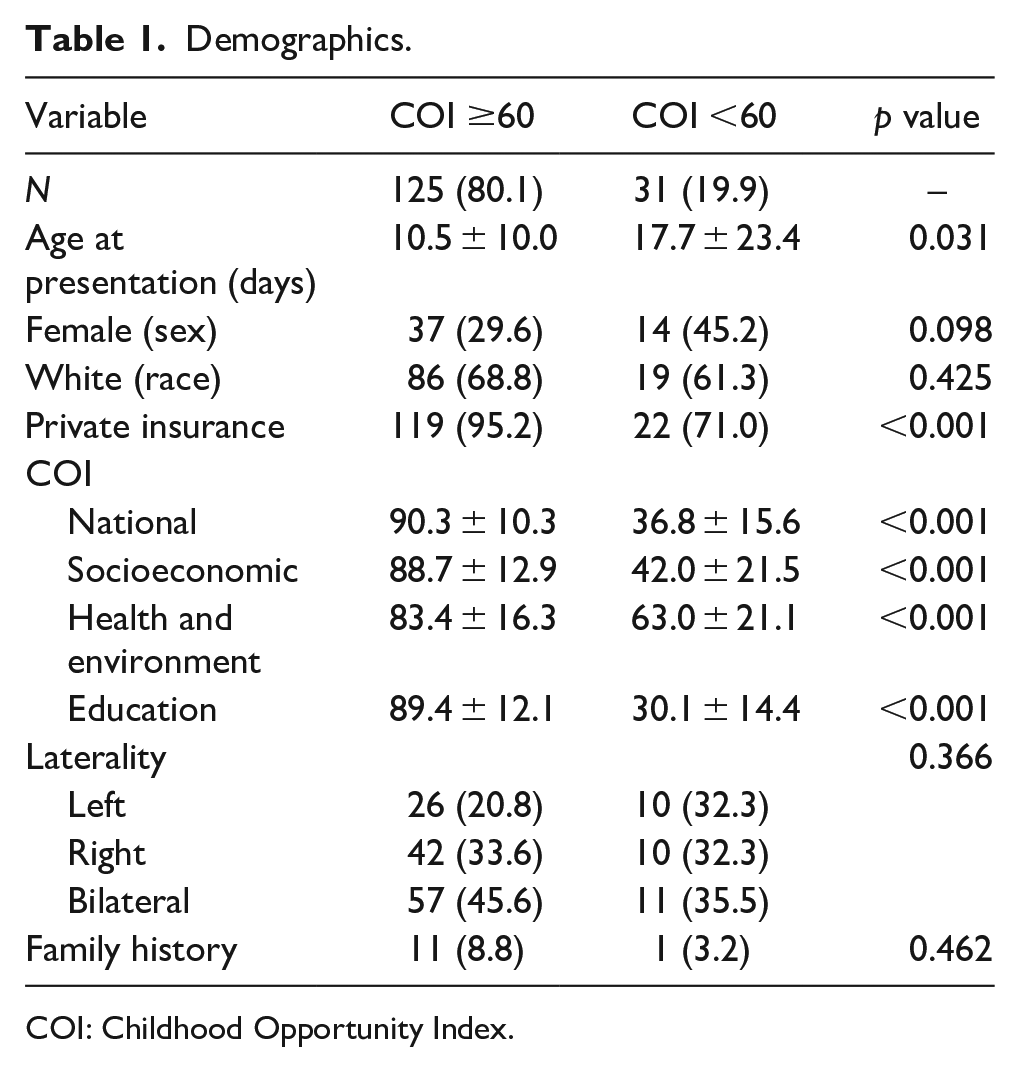
COI: Childhood Opportunity Index.
Perinatal characteristics.
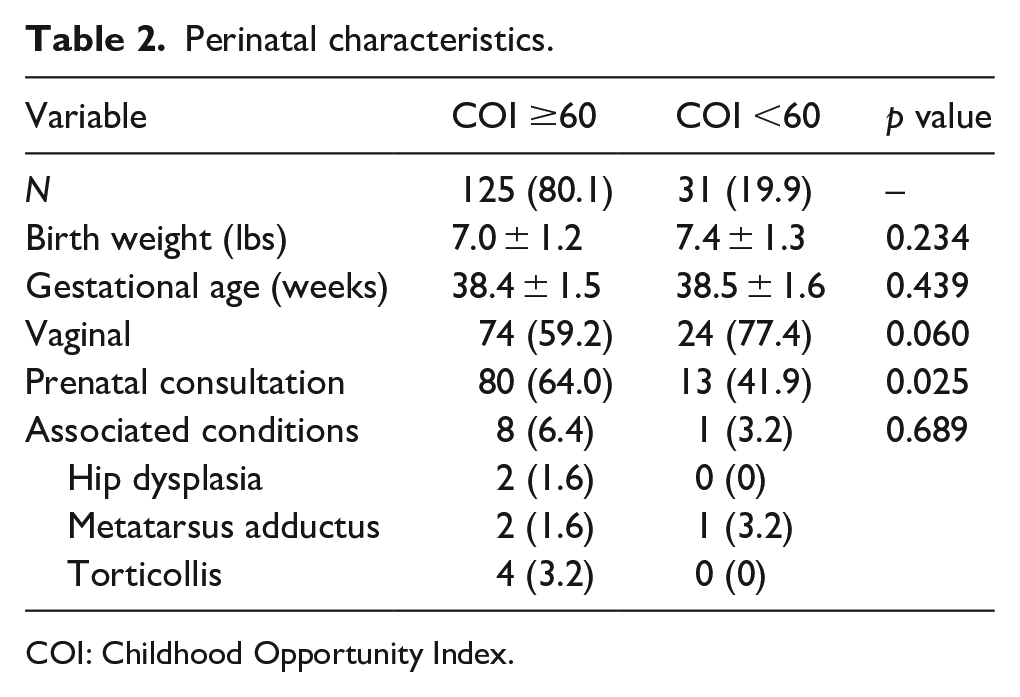
COI: Childhood Opportunity Index.
Clubfoot and treatment characteristics.
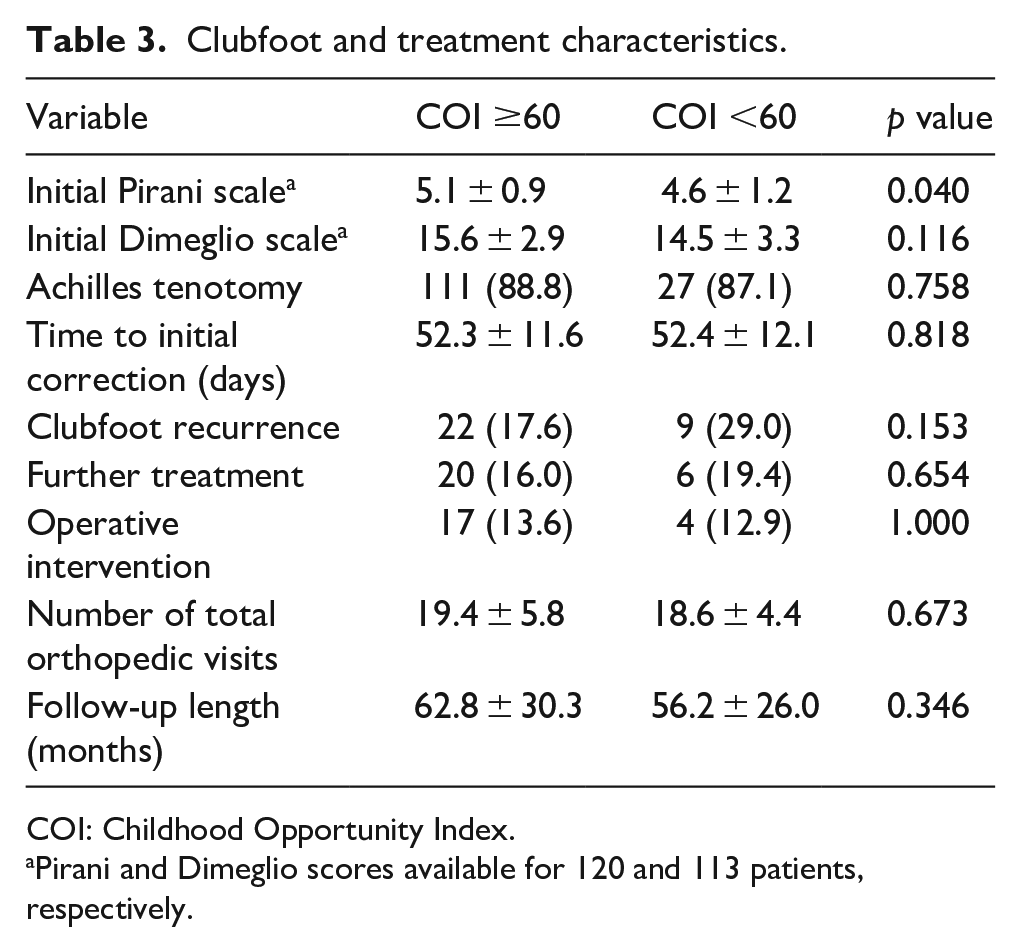
COI: Childhood Opportunity Index.
Pirani and Dimeglio scores available for 120 and 113 patients, respectively.
The highest-level further treatment assessed across the total study population included repeat casting (n = 5, 3.2%), isolated revision Achilles tenotomy or gastrocsoleus lengthening (n = 6, 3.8%), tibialis anterior transfer for dynamic supination (n = 11, 7.1%), and/or a more complex clubfoot reconstruction involving bony osteotomies and/or a posteromedial release (n = 4, 2.6%). Aside from clubfoot recurrence, there was only one complication across both groups—one patient with a high COI developed a heel ulcer that necessitated a 3-day break from casting.
Several significant differences were observed when cohorts were separated by public versus private insurance status (Table 4). Publicly insured patients had an older mean age at presentation (28 ± 31 versus 10 ± 9 days, p < 0.01) and were less likely to be White (40% versus 70%, p = 0.02). National COI scores, in addition to all sub-scores, were lower for the public insurance cohort (p < 0.05). Privately insured patients were also more likely to undergo a prenatal consultation with an orthopedic surgeon (65% versus 13%, p < 0.01). There were no differences in recurrence or need for further treatment between the publicly and privately insured cohorts. In multivariable analysis (Table 5), being Black/Hispanic (OR 6.42, 95% CI 1.16–35.41, p = 0.03) was associated with clubfoot recurrence. Prenatal orthopedic evaluation served a protective role (OR 0.28, 95% CI 0.09–0.86, p = 0.03) against clubfoot recurrence.
Clubfoot and treatment characteristics for public and private insurance status.
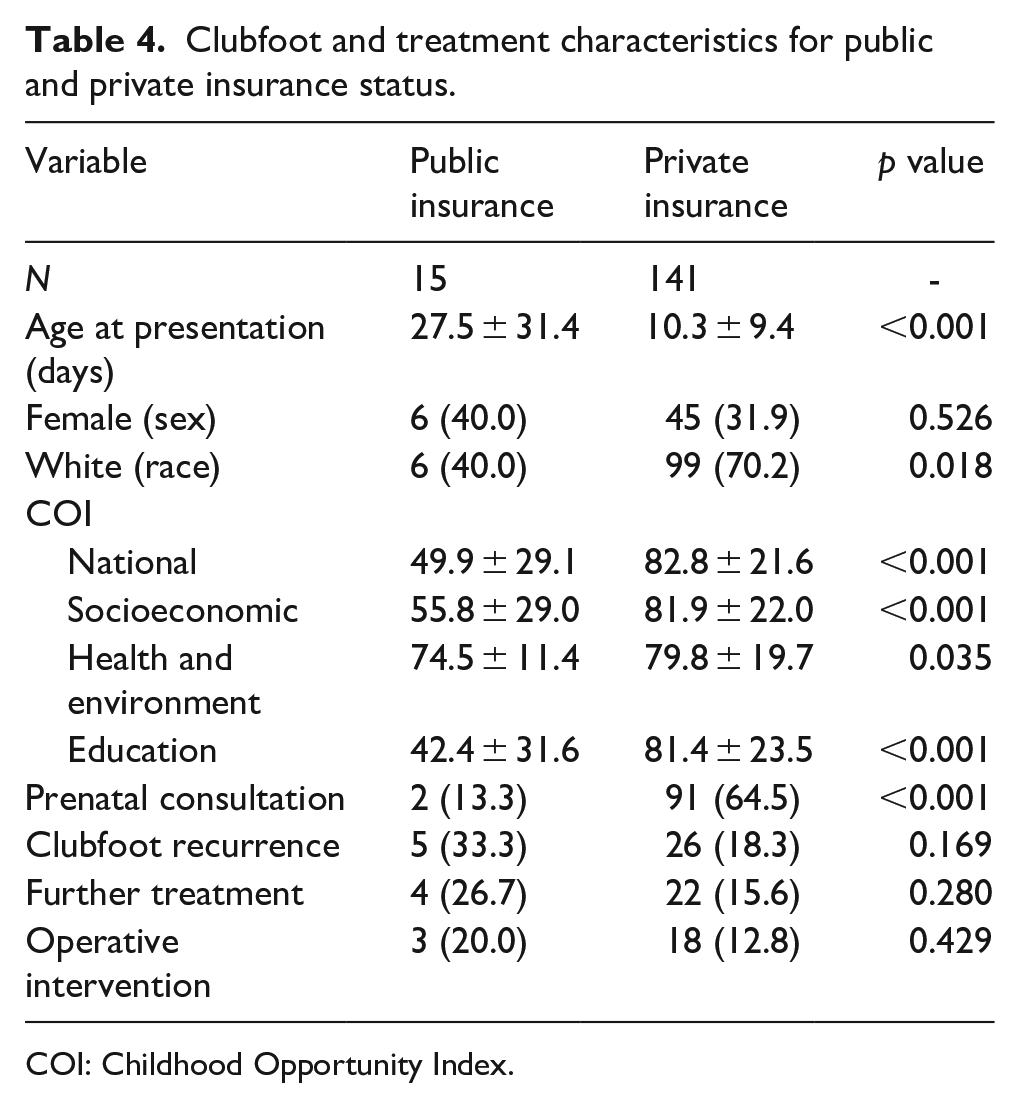
COI: Childhood Opportunity Index.
Multivariable prediction of clubfoot recurrence.
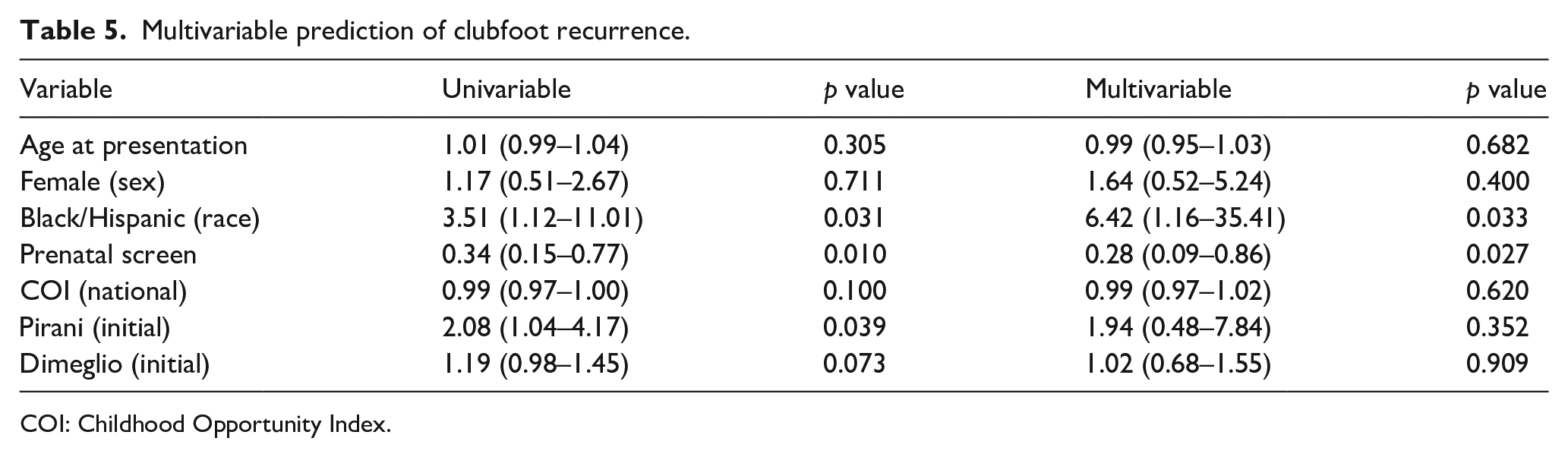
COI: Childhood Opportunity Index.
Discussion
This study aimed to determine the association between COI and treatment disparities for patients with idiopathic clubfoot. Patients in the low COI cohort presented a week later and had fewer prenatal orthopedic consultations than patients in the high COI cohort. Contrary to our original hypotheses, the rates of Achilles tenotomy, time to correction, recurrence, and further operative procedures were similar in the two groups. Publicly insured patients presented at older ages by a mean of 17 days and had fewer prenatal consultations with an orthopedic surgeon. It is important to note that while our findings of a delayed presentation in the low COI and publicly insured cohorts reached statistical significance, a delay of 7–17 days does not represent a clinically significant difference. Moreover, despite differences in initial presentation, treatment outcomes were similar in our low versus high COI and publicly versus privately insured cohorts, confirming the efficacy of the Ponseti method for clubfoot. By contrast, decreased prenatal orthopedic consultations and Black/Hispanic race in the low COI and publicly insured cohorts may potentially have downstream effects on the maintenance of clubfoot correction based on multivariable analysis.
To allow for adequate time to process the diagnosis, parents prefer to obtain a clubfoot diagnosis prenatally when identified on screening ultrasonography, 25 despite this knowledge being associated with increased incidence of depression and anxiety.26,27 Concerns exist regarding the accuracy sonography,28,29 but literature has demonstrated improving false positive rates of 7%–19% with advancements in screening technologies. 30 Following the diagnosis, parents may seek further counseling with an orthopedic clubfoot specialist, 31 which allows parents to develop a stronger understanding of the deformity, available treatment options and expected outcomes. This enables families to formulate financial plans for medical care and derive valuable psychosocial benefits which include decreased anxiety, enhanced emotional preparedness, and improved parental confidence in managing their child’s condition. 32 Our study demonstrates that patients in the low COI and publicly insured groups experienced fewer prenatal consultations with an orthopedic specialist and that completion of prenatal consultation served a protective role against clubfoot recurrence in multivariable analysis. To the authors’ knowledge, the association between adverse SDOH and lack of prenatal counseling with an orthopedic surgeon previously has not been identified. It is also possible that the benefits of prenatal consultation with an orthopedic surgeon persist years into treatment. Though not conclusive greater understanding of Ponseti serial casting and the potential for recurrence with inadequate treatment for low COI families may improve brace acquisition and subsequent brace compliance, as is seen in other lower extremity conditions, such as cerebral palsy and short Achilles tendon. 33 Therefore, the negative impact of an absent prenatal orthopedic consultation may carry psychosocial effects for patients and families in low COI areas.
This study’s findings of a delay to clubfoot treatment is an additional example of the interaction between adverse SDOH and access to orthopedic specialty care.19,34 Financial barriers such as public insurance may create disparities in access to appointments due to financially unfavorable reimbursement rates.35,36 Of 40 orthopedic clinics in Illinois, Bisgaier and Rhodes found that 98% of orthopedic clinics offered appointments to pediatric patients who reported private insurance compared to 20% of patients who were publicly insured. 36 Improving care for patients with public insurance requires a stronger understanding of the potential benefits of potential policy changes, such as targeted incentives to specialists or medical centers located in under-resourced neighborhoods and improvements to reimbursement structure. Publicly insured patients in this study presented >2 weeks later, which corroborates findings observed in other pediatric orthopedic conditions, such as adolescent idiopathic scoliosis and anterior cruciate ligament injuries.26,37,38 Several studies have demonstrated similar associations between public or no insurance and adverse outcomes in clubfoot treatment, including difficulties with brace acquisition and increased clubfoot recurrence.21,33,39 Notably in this study evaluating earlier barriers to treatment and treatment characteristics, there were no differences in recurrence or other treatment outcomes for publicly insured patients. These findings suggest that, at our institution, the effects of public insurance are concentrated on the initial portions of clubfoot management (i.e. delayed presentation). However, a delay in presentation of up to 17 days does not manifest in clinically significant endpoints.
It is also important to note that single-factor representations like insurance status may not fully capture the true impact of SDOH owing to confounding obstacles such as limited appointment access which may inflate the age at presentation. Multifactorial composite measures such as COI may provide a more holistic representation of the effects of adverse SDOH. These includes reflection of low educational attainment, lack of educational resources, limited transportation options, high rates of single-parent homes, and poverty/unemployment, all of which may affect the time to presentation for idiopathic clubfoot. Although the low COI (<60) cohort in this study presented, on average, 7 days later, there were no differences in treatment or outcomes, suggesting that a 1-week delay in presentation has no clinical significance. This is consistent with small cohort studies that report either no difference14,40 or weak correlations41–43 with outcomes in clubfoot sorted by age at presentation. Additionally, clubfoot management differs substantially among providers—particularly internationally—as some providers deliberately delay presentation to the clinic up to 1 month for various reasons, such as allowing the infant to bond with family at home. 40 The results of this study are reassuring, as a controlled delay in presentation does not result in worse clinical outcomes if the appropriate treatment is initiated regardless of SES.
When grouped by race, Black/Hispanic race was associated with a nearly seven-fold increased odds of recurrence. Race in the United States continues to be a key predictor of adverse outcomes in pediatric orthopedics possibly affecting factors including access to timely care, trust between the patient and physician, affordability, and transportation barriers.37,44–46 These impediments to optimal care may have downstream effects on key risk factors for clubfoot recurrence (i.e. non-compliance or early discontinuation of orthotics). These results reflect prior studies observing that lower parental education level and a higher Social Deprivation Index (i.e. greater deprivation) were associated with greater recurrence of idiopathic clubfoot.39,47 Conversely, Akinyoola et al. found no significant associations between Area Deprivation Index—an older composite measure of social deprivation—and clubfoot recurrence after Ponseti casting. 48 Such discrepancies may be attributed to the various indicators that are incorporated in the COI version 3.0 metric, which outperforms single-factor and other composite indices of social deprivation. Additionally, these findings may be a testament to our institutional protocols or, more generally, to the success of serial Ponseti casting as the gold standard treatment for idiopathic clubfoot. Interestingly, the high COI cohort presented with slightly higher Pirani scores, which may be clinically insignificant or a reflection of a skewed distribution of more severe presentations that seek care at our hospital. Despite obstacles to initial presentation, under-resourced patients at our institution, as measured by low COI or public insurance, derive similarly successful treatment outcomes to their more resourced counterparts.
This study has limitations. First, given its retrospective nature, there were uncaptured variables that affect the ability to obtain care. These include distance to the hospital and means of transportation that could not be recorded and/or controlled. Second, the low sample of patients with adverse SDOH in this study may present a sampling or selection bias due to the relative affluence of our urban population. This may limit the generalizability of these findings and is instead more reflective of our local referral patterns. Other rural, less densely populated, and lower COI regions may present different obstacles to clubfoot treatment. Similarly, although the Ponseti method has been established as the gold standard for treating clubfoot, there exists variations across providers and institutional protocols, which may limit the generalizability of these findings. Third, COI is an indicator of current socioeconomic factors and is not reflective of historical neighborhood deprivation and changes over time. Fourth, we excluded patients who presented to care after the age of 6 months, leading to skewed exclusion of low COI patients who may present at even older ages and experience greater difficulties with treatment and/or recurrence. Fifth, the exclusion of patients who were lost to follow before reaching 2 years old may limit our findings. These patients could alter the distribution of COI, possibly contributing to the underrepresentation of patients in the low COI group and subsequently skewing the results. Lastly, 2-year minimum follow-up may have precluded full assessment of clubfoot recurrence including dynamic supination that tends to present at older ages, though the mean follow-up for the entire study was >5 years. Previous studies have reported a mean initial age at first recurrence of 24–30 months old with a reported range of 17–39 months.15,49,50 Despite the possible omission of early recurrence, we implemented a 2-year minimum cut off to maximize the rigor of the study and analysis of long-term outcomes. Although our findings suggest that patients with adverse SDOH, as measured by low COI or public insurance, have similar treatment outcomes at our institution, future studies could incorporate a more diverse COI population with longer follow-up to evaluate brace compliance and associated impacts of stopping brace treatment too early.
Conclusion
Patients with idiopathic clubfoot and low COI/public insurance experienced delayed presentation to care and fewer prenatal orthopedic consultations. However, low COI and public insurance status were not associated with adverse treatment outcomes. Clubfoot specialists remain a critical component of the multidisciplinary prenatal team, as orthopedic consultations served as a protective factor against recurrence. These findings contribute to the existing literature by highlighting discrepancies in the care for patients with adverse SDOH.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251367969 – Supplemental material for Lower Child Opportunity Index and public insurance are associated with decreased prenatal orthopedic evaluation and minor treatment delays for idiopathic clubfoot
Supplemental material, sj-pdf-1-cho-10.1177_18632521251367969 for Lower Child Opportunity Index and public insurance are associated with decreased prenatal orthopedic evaluation and minor treatment delays for idiopathic clubfoot by Joshua T Bram, Patrick P Nian, Christopher J Williams, Olivia C Tracey, David M Scher, John S Blanco, Emily R Dodwell and Shevaun M Doyle in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
None.
Author contributions
JTB: conceptualization, formal analysis, methodology, software, writing—review and editing. PPN: data curation, formal analysis, investigation, methodology, writing—original draft. CJW: data curation, writing—review and editing. OCT: conceptualization, project administration, writing—review and editing. DMS: project administration, methodology, resources, writing—review and editing. JSB: project administration, methodology, resources, writing—review and editing. ERD: project administration, methodology, resources, writing—review and editing. SMD: conceptualization, project administration, resources, supervision, writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study was approved by the Institutional Review Board (IRB) at Hospital for Special Surgery (2023-0453). Informed consent was not applicable in this retrospective chart review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.