
Abstract
Chronic patellofemoral instability is common in children and adolescents. While it may follow a single traumatic injury to an otherwise healthy and anatomically normal knee, several predisposing anatomical risk factors are often present. This review assesses the treatment of recurrent patellar dislocation in children and adolescents. A literature review was performed, accompanied by the authors’ current suggested practice. Surgical interventions are often required, and the available procedures depend on the stage of skeletal maturity. Soft-tissue procedures aim to restore medial patellar constraints, with medial patellofemoral ligament reconstruction being the most important treatment across all age groups. Reconstruction of the medial patellotibial ligament and medial quadriceps tendon femoral ligament is a developing technique to enhance medial stability. In skeletally immature children, patella alta may be addressed with tendon shortening, and an increased tibial tuberosity versus trochlear groove distance may warrant medialization procedures such as the Grammont technique. Valgus knee is managed with growth modulation. After physeal closure, treatment options include tibial tuberosity osteotomy with distalization and medialization, as well as femoral varus or rotational osteotomy in severe cases. Trochleoplasty is also an option for adolescents after growth plate fusion. Thorough clinical and imaging evaluation is essential in cases of recurrent lateral patellar dislocation. Treatment is selected based on the likelihood of success with isolated medial patellofemoral ligament reconstruction, success underpinned by the presence of underlying anatomical risk factors and the stage of skeletal maturity for each patient. Level of evidence: Level III.
Keywords
Introduction
Recurrent lateral patellar dislocation (LPD) remains a major challenge in children and adolescents. Up to 30%–40% of children with a single traumatic patellar dislocation will develop chronic patellofemoral instability (PFI).1–3 If there have been three or more patellar dislocations, instability and further dislocations are found in 80%–90% of the cases, regardless of appropriate physical therapy. If untreated, PFI results in impaired function, pain and patellofemoral degeneration. 4
The annual incidence of PFI in children is highest in the 10–17-year age group, with the reported incidence varying between 2.6 and 125/100,000 children.5–8 The incidence of acute LPD is increasing, particularly in older children and adolescents, due to increasing participation in organized sports.9,10 Up to 60%–70% of all acute LPD injuries are sports related. 11 Girls predominate in recurrent LPD; however, acute traumatic patellar dislocations are more common in boys. 8 As compared to adults, children have two-fold higher risk of recurrent dislocations after the first index injury. 12
LPD in children correlates with abnormal bone anatomy in up to 90% of patients.13–15 The most important risk factors are trochlear dysplasia, high-riding patella and increased tibial tuberosity versus trochlear groove (TT-TG) distance, a composite figure, that is, multifactorial in nature encompassing trochlea anomalies, lateralized tibial tubercle and tibiofemoral rotation.11,16–19 Patella dysplasia, general laxity, obesity and genu recurvatum are other potential predisposing factors. In these patients, instability has usually developed during a long period of time, resulting in chronic elongation of the medial patellofemoral ligament (MPFL) rather than acute rupture. 20 Most (70%) are caused by an acute pivoting knee sports injury.9,21,22 Acute MPFL rupture may result in chronic instability and recurrent dislocations. 23
The treatment of recurrent LPD is challenging, due to its multifactorial aetiology. Available treatment methods depend on the age of the patient, while most bone procedures should be waived until bone maturity to avoid growth disturbance. Recurrent LPD has previously been treated dominantly with non-anatomic proximal or distal realignment operations, such as Insall or Madigan type procedures described in the 1970s–1980s, or Roux–Goldthwait-like procedures. These procedures aim to centre the patella into the TG. Due to increased understanding about the multifactorial aetiology of LPD since the 1990s,24,25 a comprehensive evaluation of all risk factors has been important. Reconstruction of MPFL with or without additional procedures has become the mainstay of surgical care.26,27
Aim
Despite high activity in scientific research on this topic, there is still no consensus on treating recurrent LPD in children and adolescents. 28 In this narrative review, the authors provide an updated view of clinical investigation, imaging and treatment of chronic PFI in children and adolescents. Furthermore, recognized paediatric orthopaedic sport surgeons describe their own current preferred practice. Habitual subluxation and fixed patellar dislocations, particularly in syndromic patients (e.g. Ehlers–Danlos, nail-patella syndrome and Down syndrome) are not covered in this review.
Clinical investigation
Children with PFI may suffer from chronic anterior knee pain and subjective feeling of an unstable patella, reporting difficulties in ‘trusting their knee’. Older children can usually describe patellar dislocation, often followed by spontaneous reduction during knee extension. Occasionally, medial dislocation is reported, although often this is the prominence of the medial femoral condyle described with lateral patella dislocation.
Patellar dislocation may not cause knee haemarthrosis in patients with chronic instability, similar to the initial injury. Patella tracking is evaluated during the knee movement from full extension to full flexion, best assessed when seated on the edge of the examination couch. If present, a lateral J-sign identifies the presence of trochlea dysplasia, patella alta or both. A positive patellar apprehension test may be seen, but in chronic instability, it can be difficult to perform. Coronal alignment and limb rotation are measured, including increased knee valgus, increased thigh-foot angle and excessive anterior torsion angle of the femur. Femoral torsion and thigh-foot angle should be measured in the prone position. The findings must be related to the patient’s age, while femoral anterior torsion decreases by age, tibial external torsion increases. General ligamentous laxity is evaluated, including the presence of heel valgus.
From the history, important findings suggesting surgical intervention may be needed include a positive family history of instability, first dislocation with minimal force, young age at onset and multiple episodes.
Imaging
Lateral and anterior–posterior radiographs of the knee and patellar mountain view are widely available investigations and important after primary dislocation. 29 However, in chronic patellar instability magnetic resonance imaging (MRI) is essential in evaluating the MPFL lesion, distal femoral anatomy, TT-TG, patella alta and potential chondral damage of the patella or lateral femoral condyle. 30
To evaluate patella alta, the length of patella (in millimetres) and the distance to the proximal tibia (in millimetres) are measured, 31 while the normal proportion between crude measurements (length in millimetres /distance in millimetres) is <1.2 according to both Caton–Deschamps or Insall–Salvati indexes. 32 Elevated index values >1.2–1.45 correlate with increased risk of LPD in children. 11 High-riding patella can also be described by measuring the length of the articular cartilaginous contact area between the patella and femoral joint surface in full extension. 33
Trochlear dysplasia can be defined as low-grade (Dejour type A) if a TG is present, but the sulcus angle is increased (>145°; Figure 1). If TG is missing or trochlea is convex or there is hypoplasia of whether lateral or medial condyles, trochlear dysplasia is graded as severe (Dejour types B–D). Dejour classification can be determined by radiographs or MRI. However, due to incomplete ossification of the trochlea and femoral condyles in children, particularly among children <10 years of age, the trochlear should be evaluated by MRI rather than radiographs. In addition to Dejour’s classification, the quantitative measures such as lateral trochlear inclination (>17° as cutoff for normal) and trochlear depth index (>3 mm as cutoff for normal femoral TG) are important when considering the treatment. 34 There is no consensus on the best method to evaluate for trochlea dysplasia, despite this being the major factor in recurrent instability.
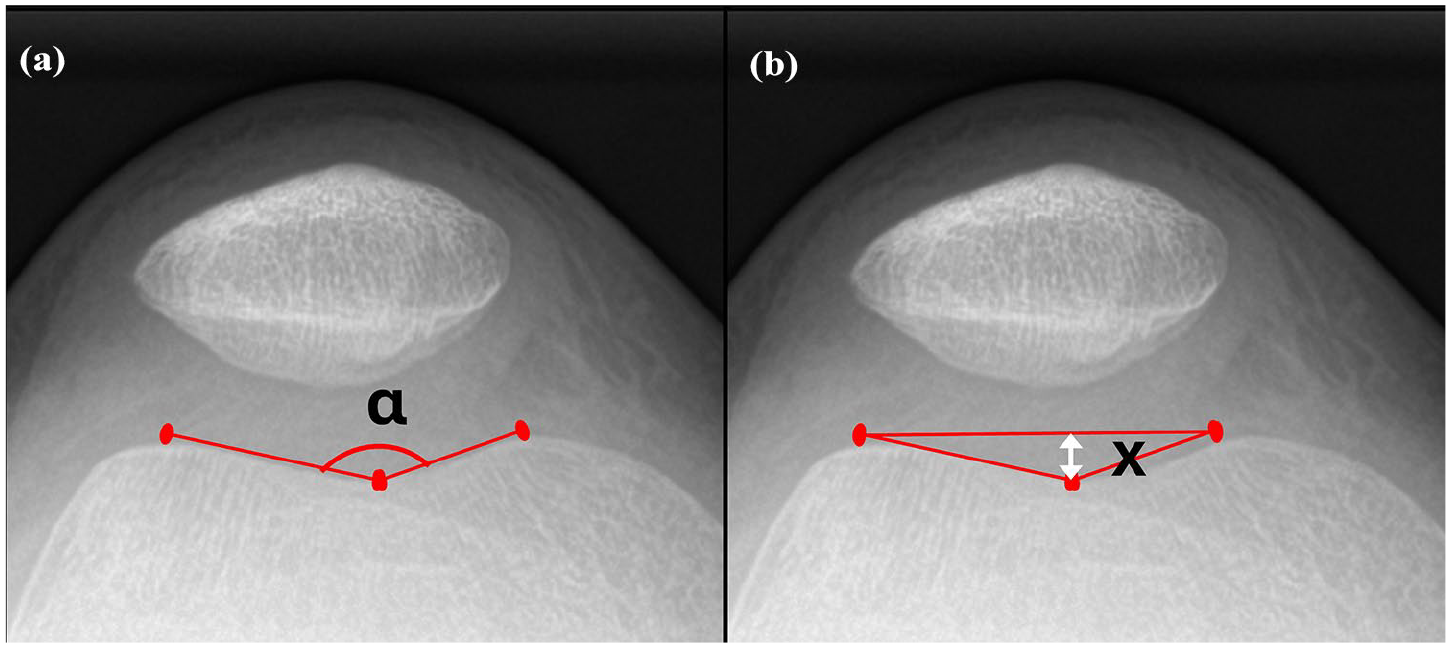
The primary radiographic measurements used to assess the quality of the femoral trochlea are: (a) the sulcus angle (a), defined as the angle between the medial and lateral condylar surfaces on a mountain view radiograph and (b) the sulcus depth (x), measured in millimetres. Normally, a sulcus angle of <145° and a depth of 3 mm or more are considered within normal limits. For a more detailed evaluation – especially in children under 10 years of age – MRI is preferred, as it allows for accurate visualization of the cartilage. MRI: magnetic resonance imaging.
The distance between TT and TG is measured in millimetres. If the sulcus is lacking, the femoral insertion point of posterior crucial ligament (PCL) is used instead of TG (TT-PCL). The potential reasons for increased TT-TG values are tibiofemoral rotation, trochlea medialization, valgus alignment or a truly laterally located TT.35,36 The normal TT-TG is 10–15 mm in the skeletally mature. 31 However, given that TT-TG measurement is a crude and multifactorial measurement, adult reference values are not valid for younger children. The mean TT-TG in children, aged 12–13, with a history of recurrent LPD is 13 mm and on average, 9–10 mm in healthy children in that age. 37 This tells us that the measurement itself is a guide to anatomical factors but should not be used for specific decisions on surgery.
The rotational profile of lower limbs, determined with computed tomography (CT) or MRI, may be important if there is clinical suspicion of rotational malalignment. When interpreting the rotation profile images, it needs to be recognized that the femoral neck angle decreases, and tibial external torsion increases with age. The findings must be related to the skeletal maturity of the patient.
If there is limb malalignment in clinical evaluation, standing full-length alignment plain films are needed. If there is disagreement between clinical phenotype and calendar age of the patient, bone age imaging is performed. Bone age is preferably determined from hand radiographs, instead of iliac bone (Risser classification), due to better accuracy and less ionizing radiation needed. Be aware that positioning of the limbs for mechanical axis views needs to be performed with caution, as apparent valgus may be misinterpreted by positioning of the patellae facing forwards. Often, torsional problems will also co-exist. 38
Treatment
Based on symptoms, clinical and imaging findings and bone maturity, an individual treatment strategy is made for every child. 39 With skeletal immaturity and growth remaining, most bone procedures should be delayed, meaning that the surgical options are more limited. The preferred management by the authors is presented in Figure 2.
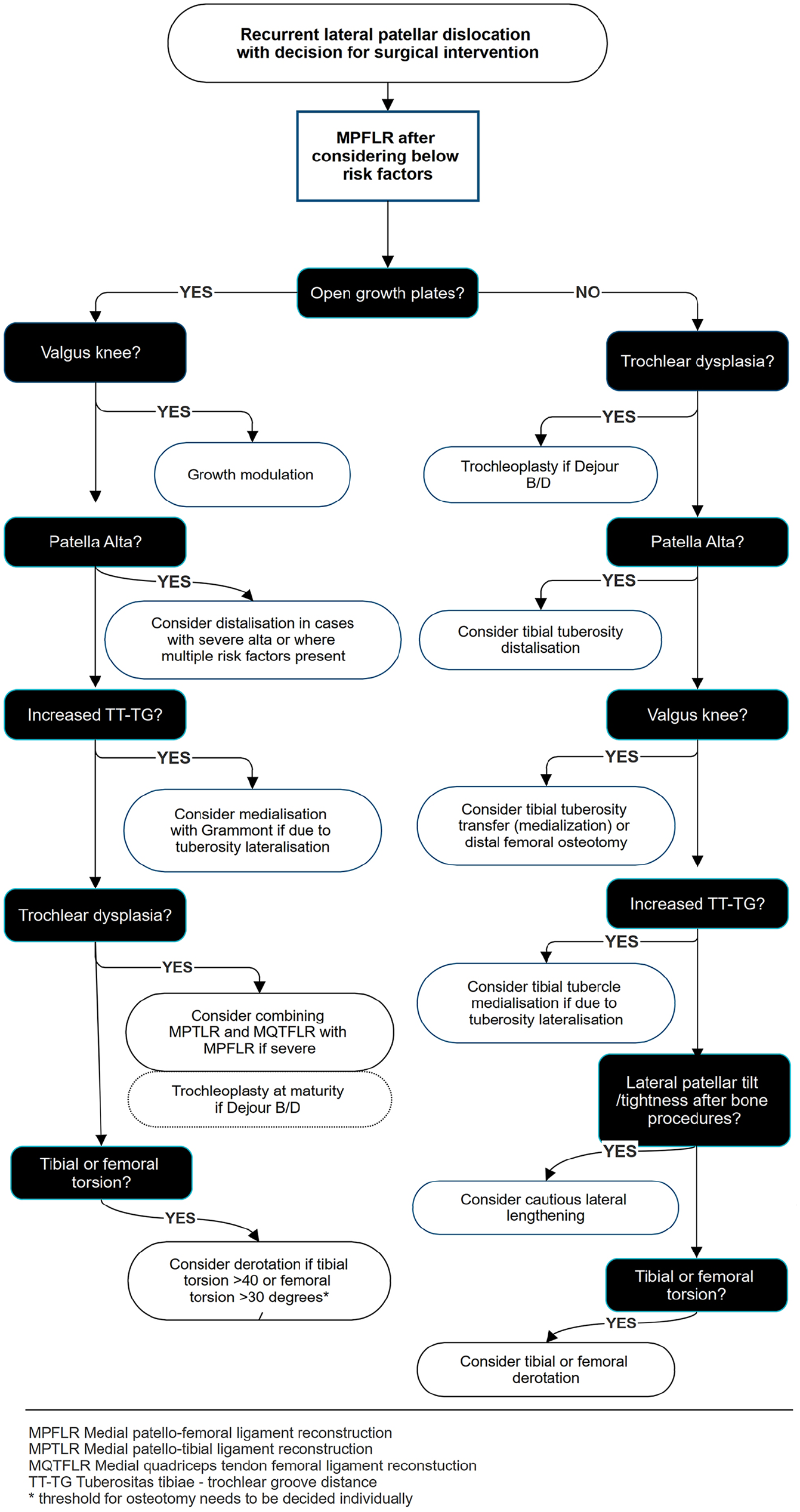
Algorithm of treatment considerations in recurrent patellofemoral instability in children and adolescents suggested by the authors. Available procedures depend on whether growth plates are open or closed. MPFLR is the method of choice, but the need for additional surgeries will be considered by a specialist. Optional procedures are performed concomitantly with MPFLR or in a planned, stepwise manner. MPFLR: medial patellofemoral ligament reconstruction.
Reconstruction of the MPFL
The main surgical treatment of chronic patellar instability is reconstruction of the insufficient MPFL (medial patellofemoral ligament reconstruction, MPFLR; Figure 3). MPFLR is available both for skeletally immature and mature children.1,40,41 MPFLR has been suggested to be an effective intervention, even as an isolated procedure, regardless of the potential anatomic risk factors.42,43 As opposed to MPFL repair, there is evidence of good results of MPFLR in preventing later dislocations.44,45 Many published outcomes have short follow up, with longer cohort studies suggesting failure rates at 5 years may be much higher. 46

Reconstruction of the medial patellofemoral ligament begins with deciding the type of graft, but hamstring tendon autograft, preferably the gracilis tendon, is the usual choice. The first incision is made two finger-widths distally from the joint level (a). Gracilis is harvested (b) and prepared for grafting. Using perioperative fluoroscopy, correct placement for both patella and femoral attachments is determined (c, d) distal to the femoral growth plate and slightly anterior to the posterior femoral cortical line. The graft is set to lay between the joint capsule and retinaculum (e), keeping the joint intact. There are several methods of fixing the graft to the patella; tenodesis using an interference screw (f) is biomechanically strong fixation, but only one cortex should be drilled to avoid surgery-based fracture. Femoral origin of the graft is fixed using a tenodesis screw, respectively (g), and that allows fine-tuning of tightness of the graft with a pull-through suture.
MPFLR can be performed as a day-surgery procedure, using a hamstring tendon or quadriceps tendon autograft, allograft or fascia lata. There is surging interest in the use of suture tape, although evidence is at present very limited in children and there is a risk of significant over-constraint. 47 Gracilis tendon is the favoured autograft by many.39,42,48,49 Due to heterogenous populations in published outcomes and no high evidence studies it is difficult to advise on ideal graft choice.
There are also multiple technical variations of MPFLR described, with the results seemingly good regardless. 18 When fixing to the patella, one cortex drilling instead of two cortices is recommended to prevent surgery-related fractures. Anchor fixation or subperiosteal fixation of the graft by using sutures is a safe option, particularly in younger children with a small patella. The graft is set between the retinaculum and the capsule, keeping the joint capsule intact. Patellar fixation is more consistent anatomically in the upper third of the patella. 48
The presence of the growth plate for fixation of the femoral MPFL insertion raises concern for growth disturbance. It is essential in a high-risk population that fixation is carried out successfully. Cadaveric studies suggest a variable position in relation to the physis for the femoral footprint, 49 but in the author’s experience is nearly always distal, and actually closer to the physis in older adolescents (Figure 4). Radiographic identification is advised of femoral fixation, combined with trials of isometry. A ligament tight in extension is too proximal in the femur, tight in flexion – too distal. Fixation can be carried out with suture anchor or tunnels. With tunnels, the drill can be angled anteriorly and distally to avoid the physis, femoral notch and articular surface. 50
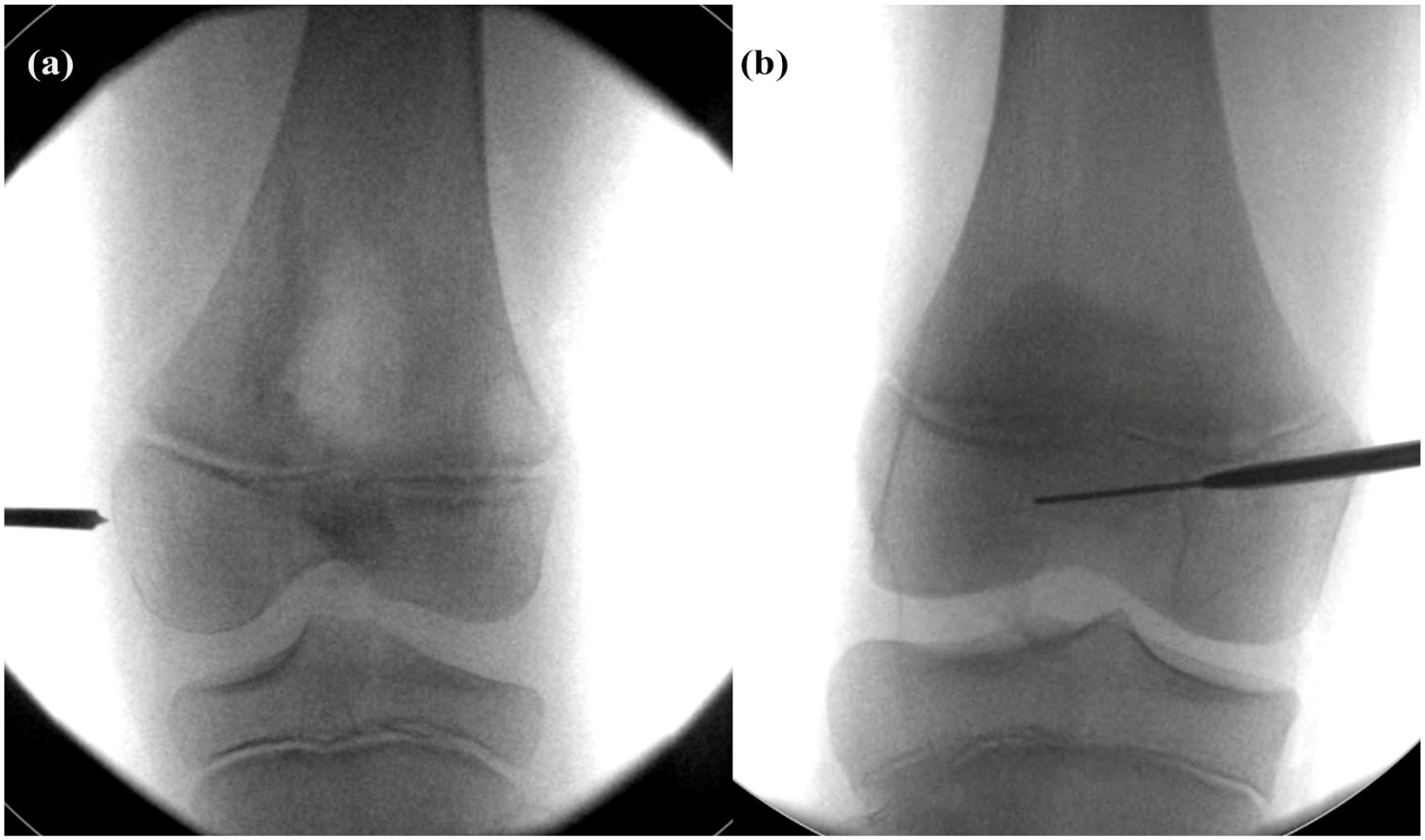
MPFL femoral insertion in (a) 7-year old and (b) 12-year-old patient identifying differing distance from the physis to the point of graft insertion. MPFL: medial patellofemoral ligament.
Contemporary reconstruction of the medial patellotibial ligament and medial quadriceps tendon femoral ligament
Where the risk of failure of isolated MPFLR is thought to be high due to factors such as trochlea dysplasia, improving the quality of medial constraint in children is increasingly performed. The addition of a medial patellotibial ligament (MPTL) to MPFLR has potential advantages in controlling instability in flexion and the first 10 degrees of extension, potentially preventing excess forces on the MPFL graft due to these risk factors and preventing patella tilt and rotation. In fact, non-anatomical reconstruction of both these structures has been performed with good outcomes without true understanding of the native role of the MPTL in adults. 51 In children, fixation into the tibia can be carried out within the epiphysis (Figure 5). The medial quadriceps tendon femoral ligament (MQTFL) is a part of the MPFL, that is, now understood to play a more dynamic role in patella stability. As early as 2019 good outcomes from combined reconstruction of the MPFL and MQTFL have been reported. 52 All three ligaments can be reconstructed simultaneously. 53 How this fits into management of the paediatric cohort are not characterized by any comparative studies, although it is felt by the authors to have a role in cases where trochlea morphology is very abnormal with associated high risk of failure, without other risk factors for failure that can be modified (Figure 6).
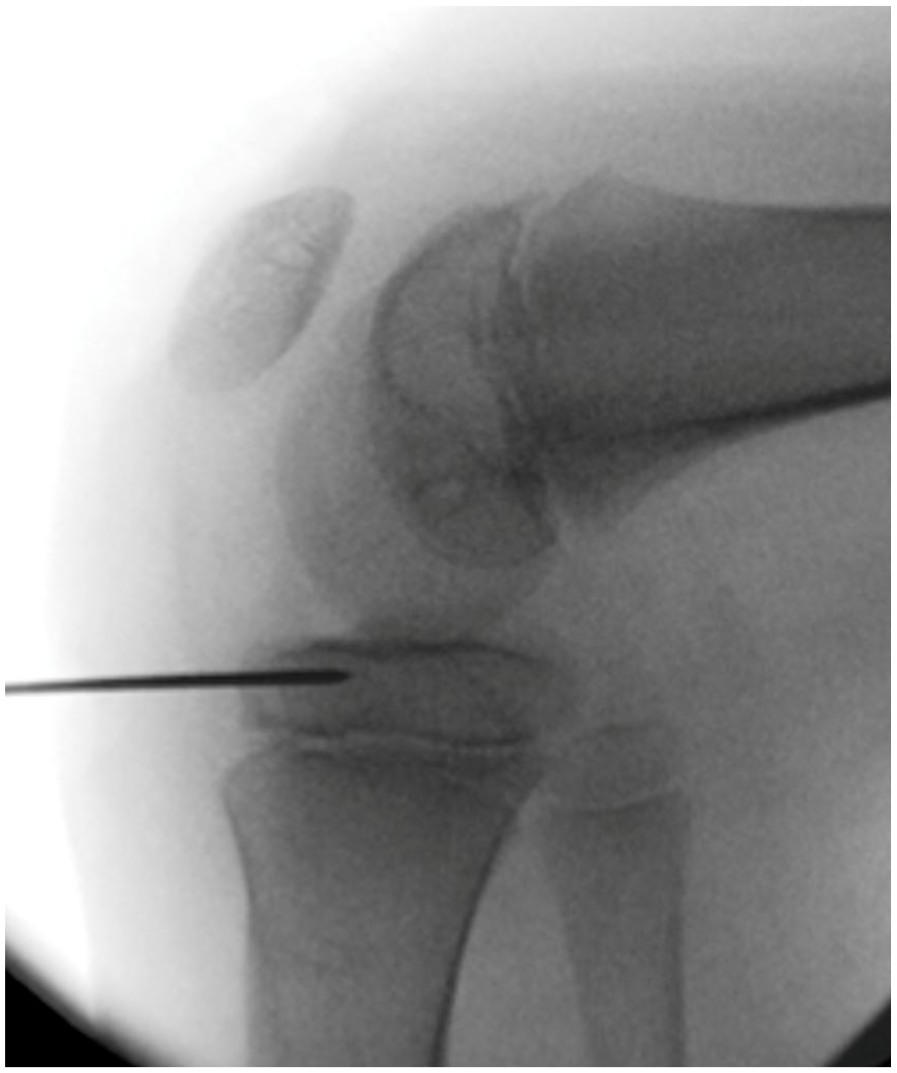
MPTL tibial insertion. A strip of medial patella tendon is fixed in the epiphysis with a suture anchor in 90 degrees of flexion at a 30° angle to the remaining patella tendon. Here a guidewire used for suture anchor fixation identifies safe placement above the tibial physis. MPTL: medial patellotibial ligament.
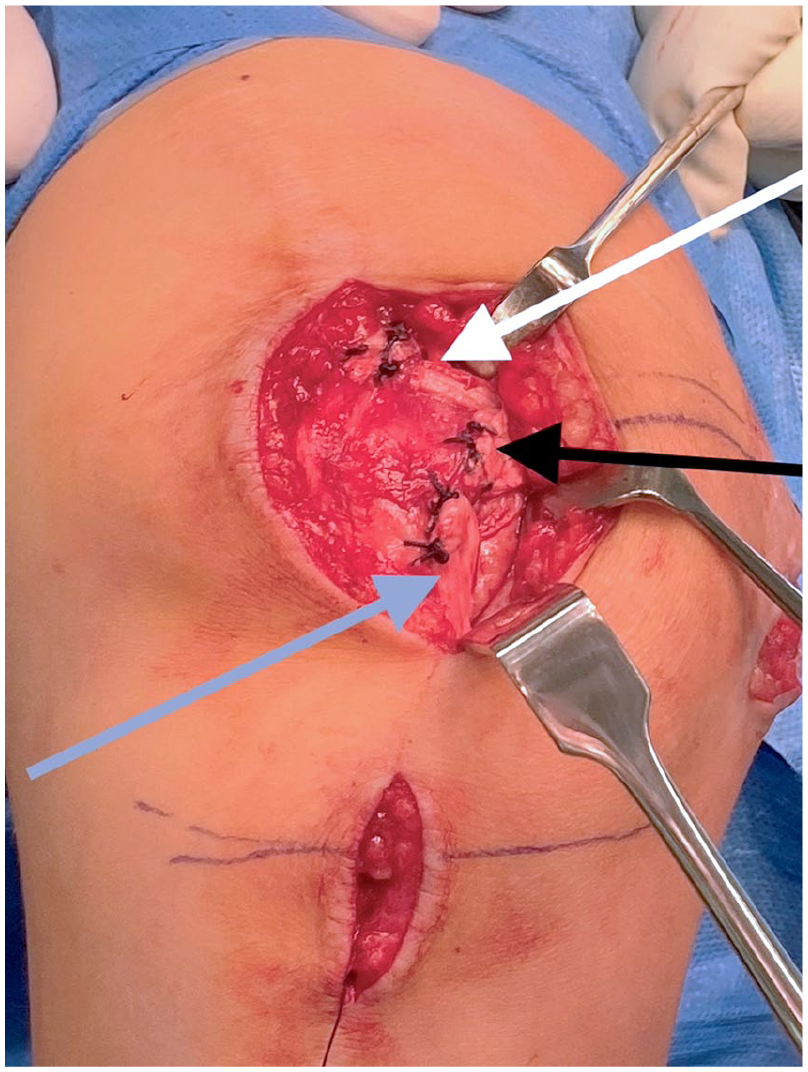
Combined reconstruction of the MPFL, MPTL and MQTFL in a 5 years old performed with a single allograft. Grey arrow identifies femoral and tibial MPTL fixation, white arrow MQTFL and black arrow MPFL fixation. MPFL: medial patellofemoral ligament; MPTL: medial patellotibial ligament; MQTFL: medial quadriceps tendon femoral ligament.
The role of lateral retinaculum release
Previously, lateral release had been standard surgery in the setting of treating patellar instability; however, no advantage is achieved when it is added to MPFL. 54 There is a high risk of iatrogenic medial instability of the patella. Lateral release may only be appropriate in selected, complex cases with high lateralizing force of the retinaculum, for example, as a consequence of changed bony anatomy after tibial tubercle transfer and trochleoplasty. 55
Dealing with other anatomical risk factors
Valgus alignment is a known risk factor for recurrent instability. Growth modulation by performing temporary hemiepiphyseodesis with a bridging plate or screws is an important option for growing patients 56 (Figure 7). Growth modulation can be performed alone or in connection with other procedures at the same time or later. The preference of the authors is to perform this concurrently. In the younger patient, recurrence is common, and ideally, the mechanical axis should be corrected to just medial to the medial tibial spine. In the skeletally mature, osteotomies are needed and commonly performed in the distal femur. Osteotomy allows concurrent correction of torsion if indicated and can be performed as a lateral opening wedge or medial closing wedge osteotomy. It is important to carefully assess the deformity parameters to identify where the valgus originates; diaphyseal deformities are not uncommon (Figure 8).
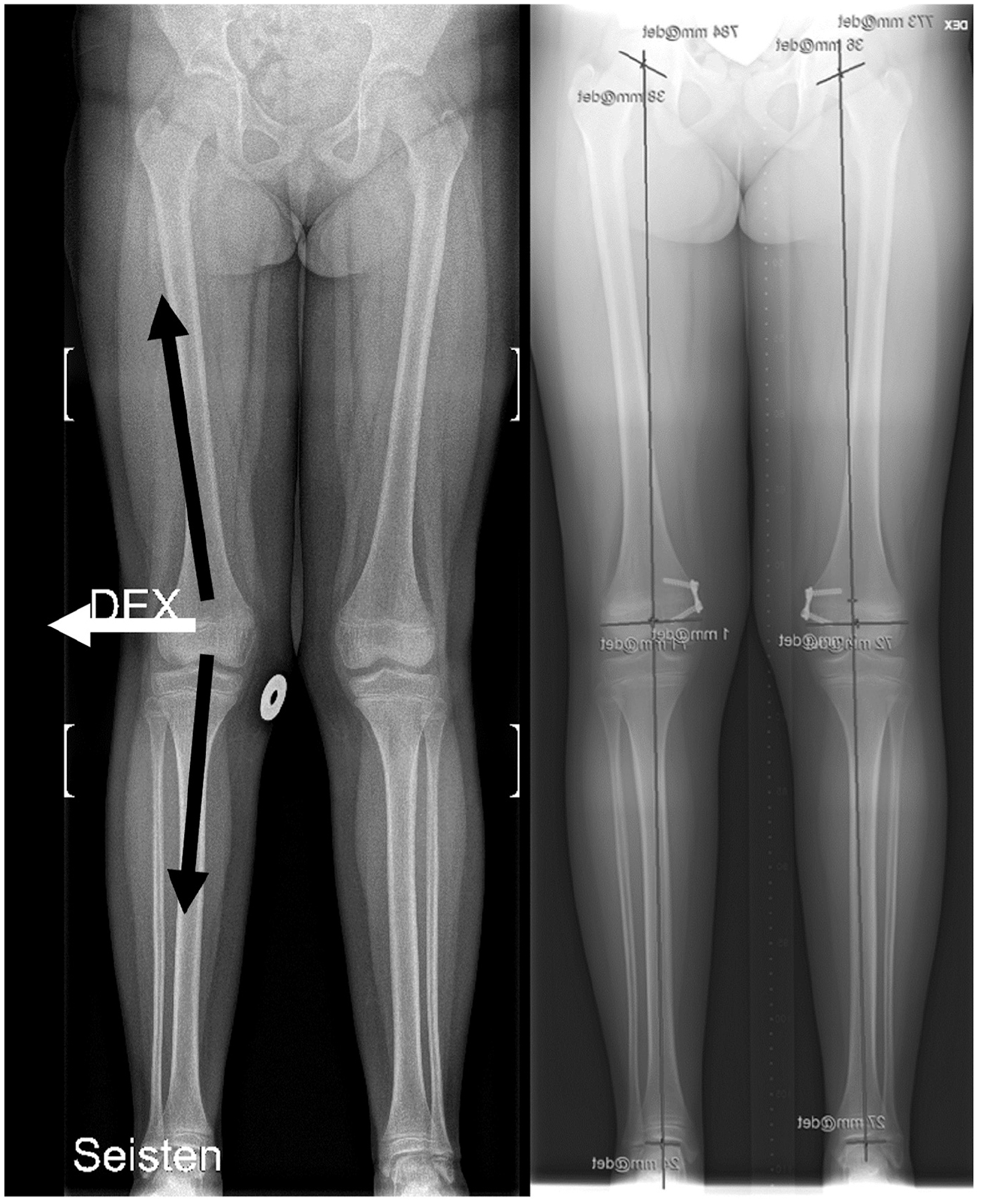
Valgus knee alignment may result in a laterally dislocating force (white arrow) to patella by quadriceps femoris muscle, accompanied by patellar tendon (black arrows; the left figure). Growth modulation by making temporary hemiepiphyseodesis was performed for this patient to treat lateral patellofemoral instability, to overcome lateralizing muscle force (the right figure).
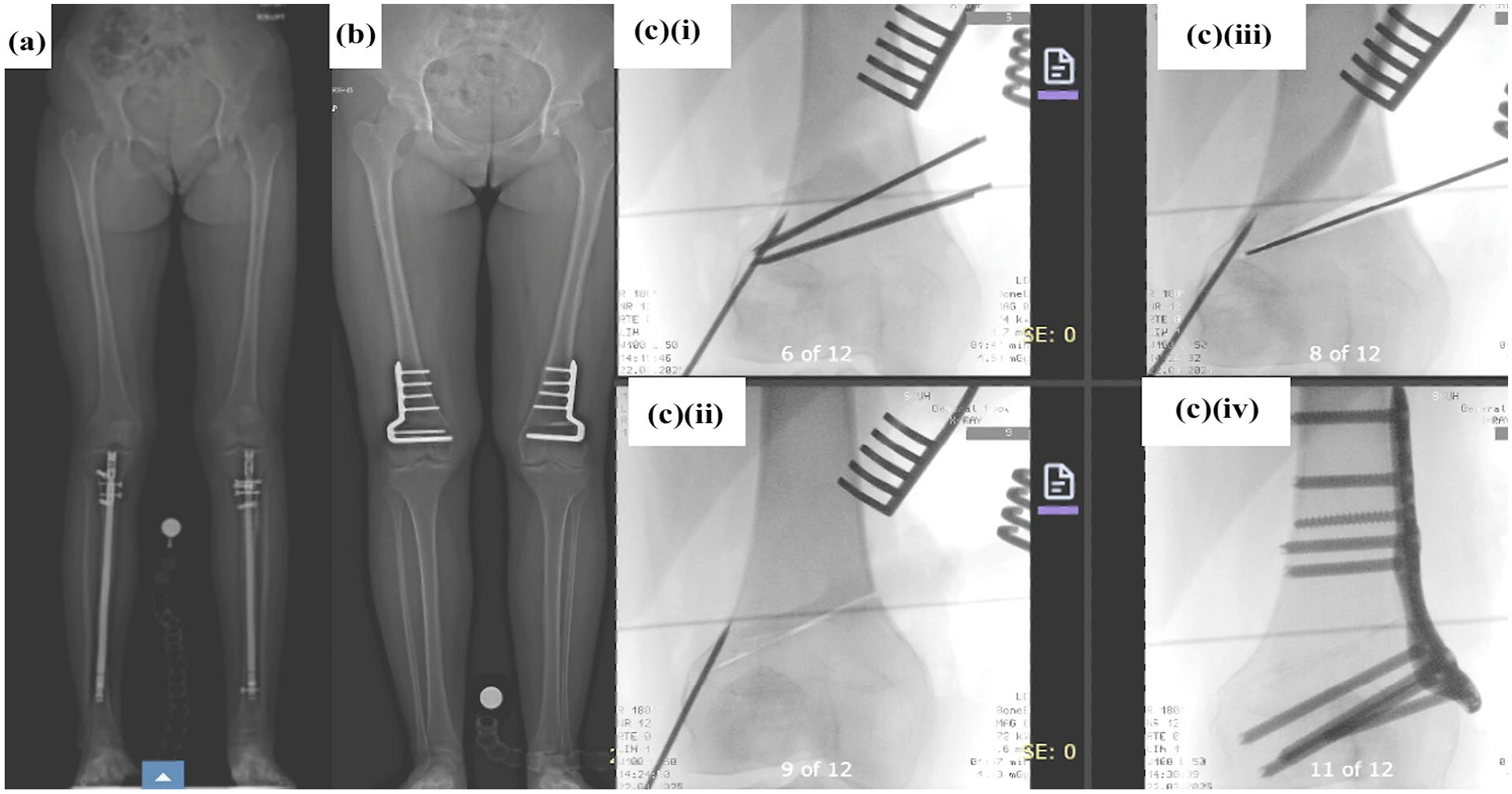
Techniques of coronal correction in three (a–c) separate cases: (a) tibial diaphyseal deformity corrected with intramedullary nailing and combined MPFL/distalizing tibial tubercle osteotomy, (b) distal femoral opening wedge osteotomy with MPFL; (ci–civ) medial closing wedge osteotomy. MPFL: medial patellofemoral ligament.
Trochlear dysplasia is without doubt the most significant factor in the failure of MPFL reconstruction in children with recurrent instability. Although there are limited case series in older adolescents with open growth plates treated with trochleoplasty, this technique should be isolated to treatment in the skeletally mature or those at the cusp of skeletal maturity 57 (Figure 9). In adults, reassuring outcomes at long-term follow-up are now published,58,59 but this is still a surgical procedure that requires considerable expertise and is infrequently considered for the older adolescent. It should be considered for those with Dejour type B or D trochlea morphology. At present, comparative studies are not available for a young cohort to determine the exact role of the younger patient. Concerns exist regarding the creation of an incongruent joint where the patella articular surface does not match the newly contoured trochlea; it is a case of balancing the risk of this incongruency and possible increased risk of flexion loss and early osteoarthritis with an unstable patellofemoral joint.
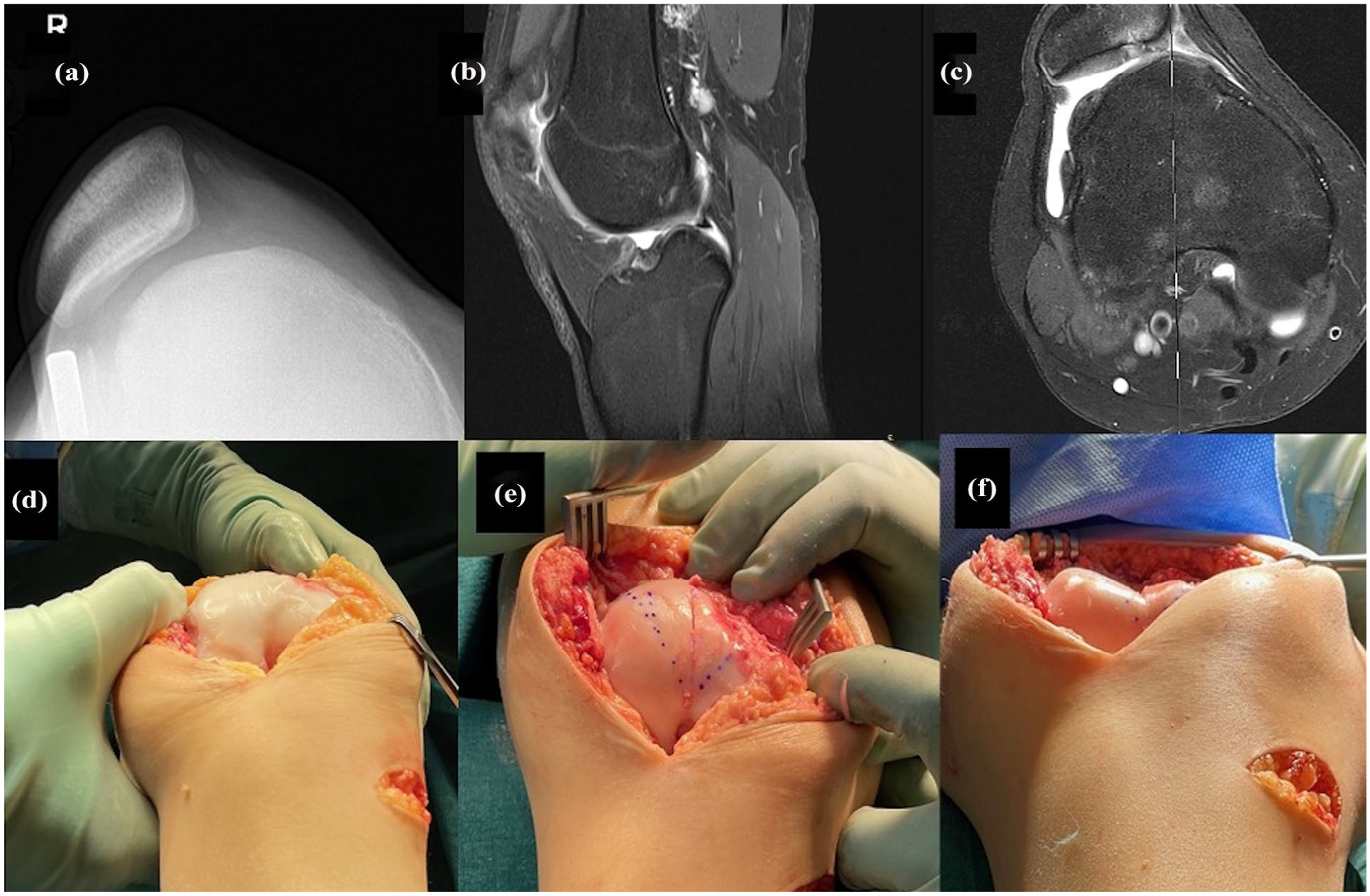
A 13-year-old girl with multiple patella dislocations (a). There was no femoral trochlear sulcus found at all; instead, (b) a trochlear spur was found in sagittal view in MRI and convex trochlear area (c). Because the growth was finished, arthrotomy (d) was performed and deformed distal femoris was evident (d). Deepening sulcus trochleoplasty was performed (e) and it resulted in good sulcus angle postoperatively (f). MRI: magnetic resonance imaging.
Patella alta can be treated in the skeletally immature. A high-riding patella causes failed engagement in the trochlea, which itself is often abnormal increasing the incidence of recurrent instability. Imbrication of the patellar tendon among the patients whose proximal tibia physis is still active can be performed.60–62 In the procedure, the patellar tendon is partly split, keeping its continuity. After making an anterior flap, plication of the deeper intact part of the tendon shortens the patellar tendon, pulling the patella downward, respectively (Figure 10). The modified Grammont procedure can also be used to both medialize and distalize the patella tendon and in combination with MPFLR. 63 There are concerns that in those with considerable remaining growth, alta can recur, often in those with trochlea dysplasia, but despite this, concerns of growth disturbance with appropriate surgical technique are not seen.
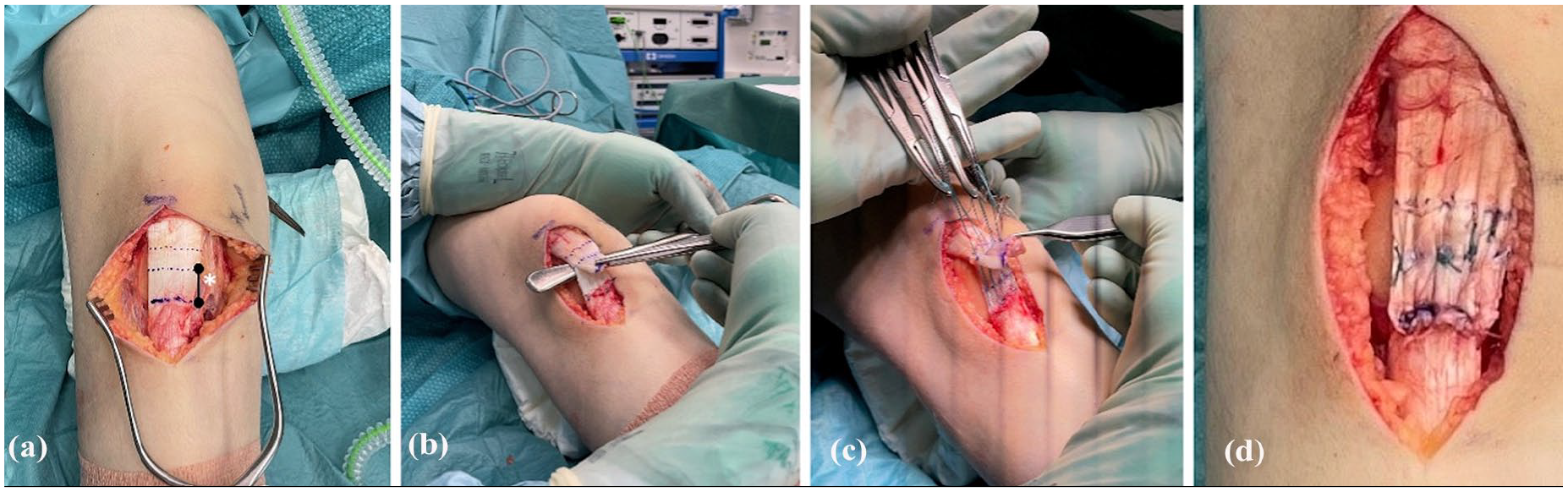
The figure demonstrates a patient with open physes who had recurrent patellar dislocations and high-riding patella. Patellar tendon shortening was performed. (a) The planned shortening is marked to patellar tendon (the black line pointed by white star presents the length of shortening). The superficial part of the tendon is cut between the shortening part of the tendon (b). Finally, the plication sutures are made to achieve the aimed shortening of the tendon (c) and after plication, there is strong fixation of shortened patellar tendon (d).
In the skeletally mature patella tendon distalization can be achieved by tibial tuberosity osteotomy (TTO). 64 After performing bony cuts, it is displaced to a new location and fixed using cannulated or solid screws, with or without an anti-glide plate (Figure 11). To decrease the contact pressure of patellofemoral, PF joint, anteriorization can be combined with distalization, according to the technique reported by Fulkerson in 1983, which was modified from Maquet’s procedure.65,66

The lower origin of patellar tendon in the tibial tuberosity can be displaced both distally (for patella alta) and medially (for lateralizing quadriceps force due to tibiofemoral rotation or valgus knee) at skeletal maturity. The tendon-bone block of ~5 cm of size is fixed to the new location by two cannulated screws and in this case combined with MPFL reconstruction. MPFL: medial patellofemoral ligament.
A patient with a high TT-TG may benefit from medialization of the TT or patella tendon. The Elmslie–Trillat procedure is a traditional distal realignment procedure, focussed to neutralize lateralizing forces to patella.67–69 It is important to identify why the TT-TG is raised, often it is a number of factors and true lateralization of the tubercle is present in less than a third of cases. Medialization should be considered as a rotational periarticular osteotomy. As understanding of the abnormalities of tibiofemoral joint rotation in recurrent instability improves, the role of medialization is likely to become more bespoke. 70
Torsional malalignment of the femur and tibia in recurrent instability remains an area, that is, controversial, lacking in evidence for treatment and associated with a rapidly evolving complexity of understanding. Decision making where abnormal torsion is identified is therefore difficult; there is no ‘magic number’ for what degree of torsion requires correction in the paediatric population, or the adult population. In children, torsion changes with growth and we have many methods of measurement on both CT and MRI with differences seen in ethnic groups. Further complexity arises in terms of understanding where the torsion occurs and the role of rotation of the soft tissues and how this is affected by bony rotational malalignment.
An example of this is external tibial torsion; the TT-TG distance should be considered before a decision on diaphyseal osteotomy, as the torsion may be sub- or supra-tubercular, meaning a distal diaphyseal osteotomy may not correct the abnormality. 71 This is an area that requires a much better understanding. The preference of the authors is to always assess for malalignment clinically, assess the gait pattern carefully and consider tibial de-rotation distally if above 40° and the associated presence of other anatomical risk factors such as severe trochlea dysplasia.
Femoral torsion is associated with trochlea dysplasia in ways that are not fully understood. 72 Femoral de-rotation can be considered where associated coronal correction is required. 73 There is limited data in adult populations suggesting good outcomes from correction, although in the paediatric population, evidence is very limited.74,75
Non-surgical treatment
Physical therapy is crucial in chronic PFI and all cases should be referred for treatment. Although some patients will have improvement in symptoms, it is rarely curative for recurrent instability. It also plays an important role in ensuring early recovery after surgical intervention. Although selective recruitment of the vastus medialis is not possible, quadriceps strengthening and preventing contractures of the hamstrings and calf complex are beneficial, as is working on core stability. 76 If a patient with PFI has a flexible, overpronated foot, the use of arch supports will reduce knee valgus forces. 77
The use of patellar orthoses with a lateral side support is rarely indicated and infrequently beneficial to patients.
Discussion
Recurrent patellar lateral dislocation is a significant problem in children and adolescents, causing not only pain and physical restriction but also affecting normal daily and sporting activities. There is agreement about the multifactorial aetiology of PFI. MPFL still remains the mainstay of surgical intervention and is a good surgical option for recurrent instability. At present, it is unclear if the treatment of associated anatomical factors results in better outcomes due to the lack of comparative studies with appropriate risk stratification. While most patients have a combination of two or more concomitant predisposing deformities, which may increase the risk of recurrent dislocation, there is no established practice for patients with multiple concomitant risk factors. 68 Not every paediatric patient needs to be treated ‘all in’ by treating all anatomical abnormalities. MPFLR is the procedure of choice, but when making a decision about surgery, the treating clinician should carefully assess for each anatomical risk factor, basing their decision to treat on the likelihood of success of just restoring enhanced medial constraint.
Conclusion
The main treatment for recurrent LPD before bone maturity is MPFLR with or without growth modulation. MPFLR with or without femoral osteotomy, TTO/patella tendon transfer, de-rotational or coronal corrective osteotomies and trochleoplasty are potential treatments to consider after growth plate fusion. Deciding between the procedures requires a deep understanding of the issue and experience in treating this group of patients, with many gaps in our knowledge.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251367295 – Supplemental material for Treatment choices for recurrent patellar instability in children and adolescents
Supplemental material, sj-pdf-1-cho-10.1177_18632521251367295 for Treatment choices for recurrent patellar instability in children and adolescents by Jaakko Sinikumpu and Nicolas Nicolaou in Journal of Children's Orthopaedics
Footnotes
Author contributions
Both authors have contributed to all parts of this research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Authors are full members (JS and NN) and chair (NN) of the European Pediatric Orthopaedic Society (EPOS) sports study group. Both authors are members of the editorial board of JCO.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical considerations
An ethical statement is not applicable to this review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.