
Abstract
Background:
Anterior cruciate ligament injury in the child and adolescent patient remains a controversial topic when considering management, especially regarding surgical choices. Treatment variations are seen not just when comparing different countries but also within nations. This arises partly as contemporary treatment is mostly inferred from the adult population who physiologically and in terms of outcomes differ significantly from children. There is an increasing body of evidence for this cohort of patients who have specific challenges and difficulties when determining the optimum treatment.
Methods:
Within this article, we will summarize the current evidence for surgical management of anterior cruciate ligament injury for the pediatric patient.
Results and Conclusions:
There remain many controversies and gaps inthe treatment of Paediatric Anterior cruciate ligament reconstruction and this high risk cohort continues to cause difficulty in identifying the best mode of surgical management.
Level of evidence:
level IV.
Introduction
The prevalence of medium- to high-level sporting activities among the pediatric and adolescent populations is increasing. Children are now more prone to sub-specialize early in sport and partake within a myriad of events, increasing the stress that may exceed their physiological capability.1,2 Studies have reported that the incidence of anterior cruciate ligament (ACL) injuries and surgical treatment in children continues to increase. 3 This, in addition to increasing female participation in sport, increased body mass index, better diagnosis, and higher demands on sporting levels, increases the risk among children of sports-related ACL injuries.
A survey done by in 2019 by both the European Paediatric Orthopaedic Society (EPOS) and the Paediatric Orthopaedic Society of North America (POSNA) found that 60% of the respondents treated pediatric ACL injuries. 4 Another survey by the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) Paediatric Anterior Cruciate Ligament Monitoring Initiative (PAMI) found a growth disturbance rate of 14%, despite most respondents saying that they do not routinely monitor for it. 5
The large variability in practice and techniques in performing this surgery has meant that it is also difficult to draw parallel outcomes from the management of ACL injuries within the pediatric population (Figure 1). The high rates of re-rupture seen in the younger cohort differ significantly from outcomes within the adult population, and the method of surgical management requires careful consideration.
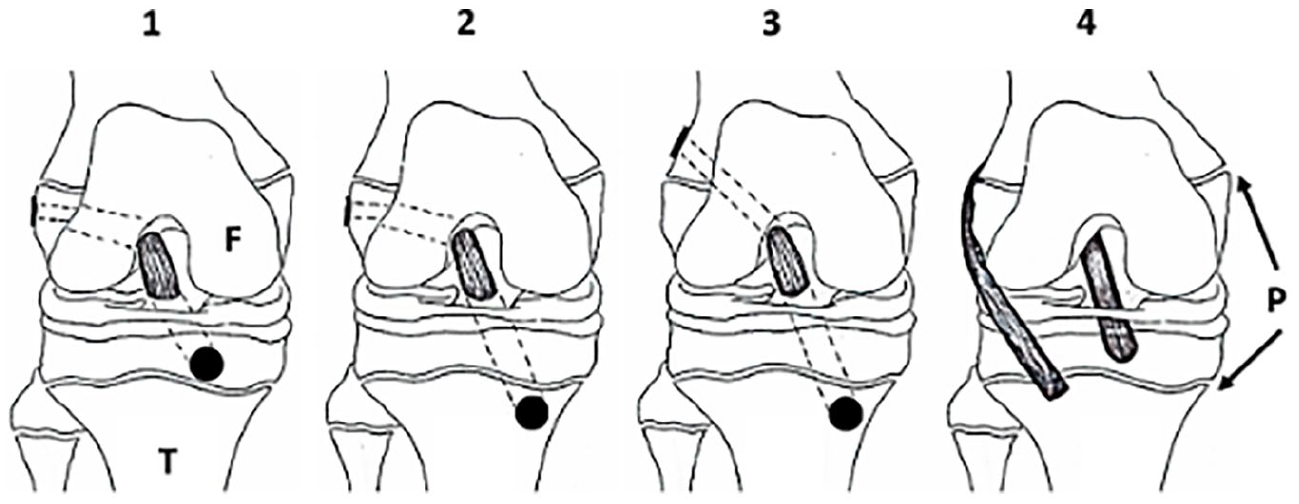
Various techniques for ACL reconstruction in the skeletally immature. Physeal sparing (1), partial transphyseal (2), transphyseal (3), and extraphyseal (4). Dotted lines represent the tunnel path.
We aim to review the current literature available and discuss the current management options in this group of patients.
Skeletal age
As with most conditions within pediatric orthopedics, the management options are dependent on both the chronological and skeletal age of the child. Damage to the physis can lead either to a growth arrest of the entire physis resulting in a limb length discrepancy (LLD) or an angular deformity if only a part of the physis is involved. 6 If identified early deformity can be corrected with relatively simple procedures like guided growth on the ipsilateral side or an epiphysiodesis on the contralateral side. However, should the patient not be followed up to skeletal maturity, such injuries can be missed, leading to potential harm.
Most studies published have used the Tanner staging as a method for identifying the growth potential of the child. 7 This staging classification, based on the secondary sexual characteristics of a child, will often involve quite an intimate examination. There are self-reporting proformas available. 8 The Tanner staging is often done perioperatively, by which time the decision on surgical techniques to be used would have already been made.
An objective measure of skeletal age is a radiograph of the non-dominant hand and wrist as produced by the Greulich and Pyle atlas. 9 This has subsequently been modified by Tanner and Whitehouse et al. (TW3) which can be incorporated into a computer software program to generate an automated report of skeletal age. 10 It is recommended that a long leg alignment radiographic view should be carried out to determine if there are any pre-existing skeletal deformities prior to the index surgery. Identification of an excessive tibial slope may also be important in predicting failure of surgery. 11
The physes at the knee in general contribute around 65% to the overall growth of the lower limb per year. 6 There are a number of methods that can be utilized to assess remaining growth. 12 We would therefore advise that any skeletally immature child undergoing an anterior cruciate ligament reconstruction (ACLR) should have their radiographic bone age measured before deciding on a specific pre-operative plan.
Management of the anterior cruciate ligament injury
The discussion with patients and their families about the most appropriate management option is one that has to occur in full disclosure. 13 Patients need to be offered a full explanation of all the management options and its associated risks and benefits prior to deciding for or against surgery. This should include the option of non-operative treatment.
Non-operative management
Operative treatment has been considered the gold standard for ACL injuries, although there is little evidence comparing surgical and non-surgical treatment for ACL deficiency in children. Furthermore, there are limited long-term outcomes studies in pediatric patients treated non-surgically. Ekås et al. 14 in an 8-year follow-up study of patients with a mean age of 13 years demonstrated satisfactory clinical results with rehabilitation alone. Half of the participants did not require surgical intervention at adulthood; however, the majority exhibited altered muscle strength, limb asymmetry, and most altered their preferred sports to non-pivoting activity. 14 The concern is that ACL-injured patients treated non-operatively experience instability, have a lower return to play, and are more likely to have meniscal tears. These findings are also found with delayed surgery. 15
Patient selection and access to resources are the most important aspects of deciding non-operative versus operative treatment. Low energy, isolated ACL injuries in low-demand patients can be managed non-operatively, in particular in the initial period 16 or until skeletal maturity with surgery conducted at a later date if persistent instability exists. 17 This could be of use when we consider the high rate of re-rupture in children and the need to avoid repeated surgical intervention or revision. The rates of return to non-pivoting sports are acceptable, although the use of a brace for sporting activity is warranted.17,18 It is crucial that there is early access to magnetic resonance imaging (MRI) to exclude associated injury and specialized pediatric physiotherapy with an age-specific approach if non-operative treatment is to be successful. We encourage lifelong patient education, frequent monitoring until skeletal maturity, and ACLR if a trial of non-operative treatment fails.
Extraphyseal ACLR
Extraphyseal ACLR was initially described in 1976 by McIntosh and Darby. This was primarily a non-anatomic extra-articular reconstruction.19,20 Micheli and Kocher modified this technique to apply it in skeletally immature patients. Modifications include an arthroscopic intra-articular component, with an “over-the-top” placement of the iliotibial band (ITB) graft from the superolateral corner of the lateral femoral condyle, into an intra-articular position of the ACL, passing it under the inter-meniscal ligament, and suturing it onto the periosteum of the tibial metaphysis. 21 An accelerated rehabilitation protocol was also suggested.
A study in 2005 by Kocher et al., 22 found that using this technique, only 2 out of 44 patients required revision ACLR, which occurred at 4.7 and 8.3 years post-operatively. A follow-up study by the same group in 2018, reporting on 23-year functional outcomes in this patient group, found a graft rupture rate of 6.6% at an average of 33.5 months. 48% of patients reported noting thigh asymmetry post-operatively, but only 1.6% complained of pain at the ITB harvest site. There were no cases of LLD or alignment issues post-operatively. 23 These results are corroborated by other studies, that report similar graft rupture rates and functional outcomes scores.19,24–26
The advantage of this technique is the low reported rate of growth disturbance due to the absence of bony tunnels through or close to the physis, in particular, very young children where the epiphysis is too small for an all-epiphyseal socket. Even though the intra-articular ligament is non-anatomical, functional scores are high and re-rupture rates are low.
Moreover, a cadaveric study series suggested that ITB reconstruction best restored rotational control compared to all-epiphyseal and transtibial technique. 27 Biomechanically, it may be a better option as long-term motion analysis shows that ITB ACLR restores symmetric and physiologic kinetic and kinematic function in the growing knee.28,29 Although thigh asymmetry is reported, it is rarely problematic.
All-epiphyseal ACLR
The all-epiphyseal technique allows an anatomical ACLR without drilling a tunnel across the physis, mirroring the intra-articular positioning of the ACL. This is most commonly performed with an “all-inside” arthroscopic technique. These can be technically challenging with a steep learning curve as the technique requires an exact graft length during preparation to avoid “bottoming-out” within the graft tunnel.
This technique is most useful for those with significant remaining skeletal growth, where a transphyseal tunnel will cause a significant loss of volume of the physis, such as in pre-pubertal children. Anderson 30 first proposed using an outside-in technique for epiphyseal bone tunnels, and a suspensory fixation on both sides. Cordasco et al. further modified this procedure using a similar technique to drill the epiphyseal tunnels, but utilizing suspensory fixation methods with good functional outcomes. Although no significant growth disturbances were reported, six patients had an LLD of >5 mm, and in two patients, there was overgrowth of more than 15 mm.31,32
Cruz et al. looking at 103 patients, with a mean follow-up time of 21 months, found a graft re-rupture rate of 10.7%. Less than 1% in their group had a post-operative LLD, none of which required further procedures. 33 Wall et al. also studied a group of 27 patients, with all-epiphyseal ACLRs, with a mean age of 11 years, at a follow-up time of 3.6 years. They utilized a technique described by Lykissas et al. 34 using a split tibial epiphyseal tunnel. A total complication rate of 48% was reported, with a 15% graft failure rate, and 7% chance of contralateral ACL tears. The complications reported were meniscal tears and reinjuries, notch impingement, and post-operative skin infections. 35
Comparing all-epiphyseal with transphyseal techniques is difficult as most comparative series consist of different age groups and as a relatively modern technique, most published series are from the beginning of the learning curve. 36
Although outcomes are equivalent to other techniques, it does not prevent growth disturbance. Proximity to the physis may well stimulate vascular changes within the physis causing overgrowth or growth disturbance. 37 Risks are higher in smaller children, especially within the tibia. 38 Three-dimensional intra-operative imaging may help reduce the risk of violation of the growth plate. 39 It is also essential to pre-operatively assess the size of the physis in order to ensure adequate size for drilling of bony tunnels. This is more important in the younger child.
Partial transphyseal ACLR
This technique is advocated for those about to enter their pubertal years. They usually have a growth remaining of between 5 and 7 years and are between the Tanner stages 2–3. Most techniques described have utilized an extraphyseal or all-epiphyseal femoral tunnel and transphyseal tibial tunnel, based primarily on the femur contributing a greater percentage of growth compared to the tibial, although variations have been described. The advantage over the all-epiphyseal techniques is the ability to tension the ligament by hand before fixation.
Andrews et al. reported a study of eight patients, with a mean follow-up time of 4.8 years. They used an extraphyseal over-the-top technique, with 7 mm transphyseal tibial graft tunnel. None of their patients reported an LLD. 25 Lo et al. 26 utilizing a similar technique reported no cases of an LLD, with a mean increase in height in their patient group of 17.5 cm.
Willson et al. performed an all-epiphyseal femoral and transphyseal tibial tunnel in a retrospective case series, 23 patients, with a mean age of 13 years. They reported no angular deformities. Twp patients in their group developed an overgrowth in the ipsilateral limb of between 1 and 2 cm. One patient with a 2-cm LLD required a subsequent pan-genu epiphysiodesis on the contralateral limb. 40
A further study by Chambers et al. utilizing a similar technique looked specifically at the presence of growth disturbance post-operatively. They found in their series of 24 patients that 16.7% developed a growth disturbance, with 66.5% of those with more than 5 years of growth left developing an LLD. 41 Guzzanti et al. also published on a partial transphyseal technique, which is the reverse to the commonly accepted technique. They performed a femoral transphyseal tunnel and an all-epiphyseal tibial tunnel. No patients in either group developed an LLD or angular deformity in this time. 42
Transphyseal ACLR
This is the most conventional technique utilized in ACLR. It is most commonly used for those approaching skeletal maturity. Intra-operative imaging is not required, and it is a simple technique that could be reproduced in all age groups meaning familiarity with a single method of reconstruction.
Kocher et al. 43 assessed 61 knees, with surgery done at a mean age of 14 years. They identified a graft rupture rate of 3% (2/61). Three cases developed arthrofibrosis requiring a mobilization under anesthesia, and no patients sustained an LLD or angular malalignment.
Calvo et al. also reviewed 27 patients, with a mean age of 13 years. Three out of 27 patients developed a graft rupture (11%), with 7% developing persistent instability post-operatively. They did not report any cases of LLD or angular malalignment. 44
There are a few reports regarding growth disturbances in the transphyseal ACLR group. Kohl et al. 45 reported on 15 patients over a follow-up period of 4 years, and only found one patient developed a valgus deformity post-op. Redler et al. 46 also looked at 18 patients, over 3.6 years and reported no cases of graft rupture, LLD, or malalignment. Their results are similar to those by Liddle et al. 47 Shelbourne et al. looked at the safety of transphyseal drilling in the skeletally immature. They had a follow-up of 3.4 years, among 16 patients, 7 in Tanner stage 3 and 9 in Tanner stage 4. They had a mean growth in their cohort of 11.7 cm in boys and 6.6 cm in girls. There were also no reports of LLD or malalignment noted. 48
Therefore, transphyseal ACLRs remain a safe, and probably the most common ACL reconstructive procedure that is currently available to treat ACL injuries in children. In the correct patient group, it leads to a predictable outcome for children. They will need to be followed up to skeletal maturity to ensure that any growth disturbance is documented.
A systematic review by Buckle et al. compared the techniques of extraphyseal/all-epiphyseal versus transphyseal ACLRs. They found in 425 cases that Lysholm and Tegner activity scores were the same between both approaches, although the outcomes for non-surgical treatments were statistically worse. There were no differences noted in terms of LLD, malalignment, graft rupture, or symptomatic instability. 49
The difficulty is the varied methodology and lack of reproducible methods performed to assess for growth disturbance, and it is likely that rates are higher than those published. Faunø et al. 50 in an MRI follow-up study found a quarter of transphyseal ACLR patients had some degree of growth disturbance. Without looking for growth disturbance, it is unlikely it will be identified.
Graft choice
Autograft is the gold standard for ACLR in children and adolescents. The choice of autograft is influenced primarily by patients’ age, anatomical characteristics, and participation in elite sports. 51 Soft tissue such as ITB and hamstring are the most frequently used grafts; 52 however, a few studies compare these techniques in the pediatric population. The use of alternatives such as quadriceps tendon autografts, bone-patella tendon-bone (BTB), tissue typed, and irradiated allografts as well as the role of graft augmentation need further investigation.
The advantages of hamstring grafts include the ease of harvest, no risk to the physis, and no risk of patella fracture. Disadvantages include possible higher re-rupture rates, a reduction in sprint speeds, variations in graft size and inferior graft host integration times when compared to BTB.51,53 Furthermore, recent debate has highlighted the importance of gender-specific graft choice which may have potential implication for rehabilitation. Young females are more likely to have a high quadriceps to hamstring activation imbalance which may have implications for reinjury and revision rates. 54
BTB is a valid option in adolescent ACLR, in particular for Tanner 3–4. The advantages here include a rapid tissue integration time, potential lower re-rupture rates, and the use of ligament rather than tendon for reconstruction.55,56 The disadvantages of BTB autograft include a higher risk of arthrofibrosis when compared to other autograft types,57,58 anterior knee pain, and patella fracture. The main concern, however, is injury to the physis, and therefore, traditional harvest techniques are contraindicated in the skeletally immature. Novel or alternative harvest options for BTB have been described but not proven effective. 59 It cannot be recommended for those with open growth plates.
Quadriceps tendon autograft is rising in popularity in both adults and the skeletally immature.60,61 Quadriceps suitability as a graft is easily assessable on MRI and graft diameters of over 8 mm are achievable in the vast majority of pediatric patients. 59 The literature is lacking in the pediatric population, but the advantages of quadriceps grafts include a lower surgical insult than BTB and hamstring tendon (HT) autografts, lower risk of patella fracture, comparable graft survival, return to pre-injury level of sports, and patient reported outcome measures (PROMs).52,62,63
ITB autograft is another graft used interchangeable with allograft for congenital multi-ligament deficiency reconstruction. Considering a PRISM survey, this technique was the most frequently used technique for ACL injuries in patients aged 8–10 years. 64 ITB may possess an advantage as it requires little surgical insult to harvest which may translate into improved limb asymmetry rates post-operatively and superior kinematics, although thigh asymmetry is seen. 65
The use of irradiated allografts in ACL has been contraindicated for many years due to unacceptable failure rates and its use in the pediatric setting is not proven and is therefore contraindicated as an initial choice. Different outcomes are reported but additional studies are needed to increase the variables such as the type of graft and the indications. Living donor allografts where parental tendon is donated to the child is a developing area and requires further research.66,67 The role of this technique is currently unclear, but it carries significant financial, ethical, and legal considerations.
There is limited debate as to the role in the use of internal bracing/graft augmentation techniques to aid in graft ligamentization, graft-bone integration, graft size manipulation, and tensile strength both in ACLR and ACL repair. These techniques have been examined in the adult population with no consensus on their usefulness but have yet to be assessed in children. 68 The ACL continues to grow in width and length until the terminal stages of skeletal maturity. 69 Therefore, augmentation of the graft with neo-ligament devices may be contraindicated in the skeletally immature due to the concerns regarding the potential tethering of the physis and altered growth. Other frequently cited complications include increased rates of re-operation, implant removal, synovitis, and debris. 70
AEAPs
Anterolateral extra-articular procedures (AEAPs) include anterolateral ligament reconstruction (ALLR) and lateral extra-articular tenodesis (LET), the latter of which may be responsible for the low re-rupture rates seen with extraphyseal reconstruction. The indications, contraindications, techniques and outcomes of AEAPs are evolving but the current literature supports their use in the reduction of graft failure rates and improvements in rotational stability.71,72 Rates of re-rupture are the highest in children and the routine addition of AEAPs has been suggested for the skeletally immature, although the absence of rotational stability is not necessarily the cause of higher failure rates.
Concerns regarding addition of this procedure include the risk of over-constraint and later degenerative joint disease, the lack of definitive diagnostics methods to guide decision-making and a few anatomical studies examining the anterolateral pediatric knee.73,74 One recent cadaveric study has demonstrated that the anterolateral complex is inconsistent, ill-defined, and underdeveloped in children highlighting the need for further research. 75
The current literature favors the addition of an AEAP in patients with two or more risk factors, namely, hyperlaxity, over 10 degrees of recurvatum, evidence of high-grade pivoting injury (meniscus tears, lateral compartment osteochondral trauma, multi-ligament injuries) and involvement in pivoting, collision, or contact sports.71,72,76 Another indication for AEAPs in the pediatric setting may be very young children who have a limited rehabilitation capacity and poor neuromuscular control. 77
Pediatric cadaveric studies have shown some improvements in translation or rotatory instability with AEAPs but clinical outcome data are lacking in the skeletally immature. 28 The adult literature does support the use of AEAPs with which there has been improved graft failure rates regardless of AEAP method, better outcome scores, and patient satisfaction. 74 When comparing ALLR to LET, there may be greater knee constraint, in particular with deep flexion, when using LET, similar rotation stability with both techniques but a superior translation control with ALLR.74,78 It is unclear if these results can be extrapolated to the child or adolescent populations and further clinical research is needed. Other considerations in the skeletally immature include the effects of AEAPs on the post-operative recovery period given the increased surgical morbidity with dual incisions and the possibility of peripheral physeal injury.
ACL repair
The larger blood supply to the pediatric ACL arises in the space separating ACL and posterior cruciate ligament (PCL) and is aided by a well-defined septum separating the anteromedial and posterolateral bundles of the ACL.79,80 Vascularity and cellularity of the ACL are the highest in utero and regress in a similar fashion to the blood supply of the meniscus.79,80 Furthermore, the increased cellularity involves pluripotent vascular stems cells which are abundant in the infantile knee. 81 Given that blood supply to the ACL is predominantly truncal with relatively avascular osseous attachments, ACL avulsions or stump injuries maintain vascularity and indicate an improved potential for healing in the young knee. This supports the investigation of ACL repair as a viable option in children.82,83 Moreover, some studies suggest the possibility of specific biochemical intra-articular profiles in pediatric ACL tears; however, there is insufficient evidence to understand the role of synovial environment in ACL healing.84,85
There are several techniques described, but there is no consensus on patient selection, indications, and contraindications for each. Different authors suggest that ACL tear location and quality of the ACL stump are the most important factors to select the patient and the best technique; however, evidence is lacking. 86 In general, there are two types of repairs: direct repair—proximal osseous avulsions and proximal or distal ligamentous injuries are repaired directly using suture anchors or suspensory techniques86,87 and augmented repair—involving the use of either an internal brace (typically woven non-absorbable terephthalic polythene polyester device), a dynamic intra-ligament stabilization device, or collagen matrix augmentation.88,89
The published results are of mixed outcome and consist of low-level cohort studies. Direct repair of proximal ACL tears shows good clinical and patient reported outcomes at short and midterm follow-up.86,87,90 Augmented techniques which use non-absorbable materials show high rates of re-operation and failure in both adults and the skeletally immature, with re-operation rates in adolescent patients over 10 times higher than ACLR. 87 Conversely, the use of non-absorbable augmentation for an initial period of 3 months, followed by extraction, may be associated with adequate clinical outcomes at 2 years’ post-operatively. 89
The use of biologic augmented repairs termed the Bridge-Enhanced ACL Repair (BEAR) technique, which utilizes absorbable collagen matrix from bovine tissue as scaffold is also being investigated in the adult population. This scaffold is hydrophilic and softens when autologous blood is added to it, making it conformable to the intra-articular notch. The scaffold is passed via the tibial tunnel, with the aid of sutures and a suspensory fixation device on the femur, and engaged onto the lateral femoral cortex. Five to ten milliliters of autologous blood obtained from the patient’s antecubital vein are added to the scaffold. Absorbable sutures placed within the remaining ACL stump, tied over the femoral cortical button, were tightened to bring the tibial ACL stump into the scaffold and toward the direction of the lateral femoral condyle. The tibial end of the suture is tied over a second cortical button on the anterior tibial cortex. When compared to primary hamstring autograft reconstruction, repair was not inferior in terms of clinical outcomes or subjective patient feedback at 2 years. This technique is thought to be beneficial as it prevents the adverse effects of synovial fluid on the inflammatory response, thus allowing healing after a repair. 91
The potential advantages of ACL repair include reduced surgical trauma, avoidance of autograft harvest and complications, and maintaining native ACL tissue and so proprioceptive function. However, there are concerns with the use of augmented repair techniques using non-absorbable materials.70,92 Other potential complications include arthrofibrosis, device breakdown, and chronic immune responses or synovitis. 70 The added difficulty is in identifying tears amenable to repair, as specific MRI sequences are required to identify those suitable, namely, the proximal and distal ruptures. At present, this technique should be limited to prospective studies with close follow-up as opposed to routine practice.
ACL rehabilitation
The success of ACLR is influenced by the child’s physical and physiological state, the magnitude of the initial trauma, the surgical techniques, and time since operation and access to specialist facilities and professionals.93–95 Of these, physiotherapy is arguably the most critical, but evidence-based, consensus guidelines for the rehabilitation of children with ACL deficiency, and post-ACLR is severely lacking. Return to pre-injury level of sports is high in children but so are reinjury rates. 96 There are various features unique to the growing athlete that differentiate them from their adult counterparts and that must be considered. 97 These include a developing neuromuscular system resulting in different landing and pivoting kinetics and kinematics, including greater dynamic valgus than adults.76,93,98 Children require more time to recover strength than adults, more time for neuromuscular retraining, and added time to address the contralateral limb. They require closer guidance and rigid objective targets of recovery which could be achieved through novel and innovative solutions such as with the use of artificial intelligence and virtual reality. 99 It is not only the surgical technique that requires modification from the adult norm.
There is wide variation in rehabilitation practices and post-operative protocols. A more guarded post-operative regimen, and a return to sports no earlier than 9 months post-operatively, has been shown to reduce the risk of re-operation and revision in children. 100 In this context, the International Olympic Committee advised postponing return to pivoting sport for at least 12 months following pediatric ACLR. 101 It may, in fact, take much longer for the injured knee to recover to its pre-injury state, and some have advocated a period of up to 2 years before return to full contact sporting activity. 102 Such time frames may be unrealistic in competitive sports and too guarded of an approach could results in poorer final range of movement, greater limb asymmetry which, in turn, increases the risk of reinjury. 58
Conclusion
Current literature is lacking in high-quality clinical and laboratory research in all areas of pediatric ACL injuries. Skeletal age should be used to guide the technique used, of which the many described methods as of yet do not have clearly defined roles in overall management. Growth disturbance is under-reported. Hamstring and ITB autograft remain the gold standard for ACLR in children, but quadriceps autograft may be a promising alternative. BTB graft should be avoided in the skeletally immature. The use of AEAPs is encouraged in carefully selected pediatric patients, and future research should attempt to identify objective clinical and radiological perimeters to guide the management of anterolateral or rotatory instability. ACL repair is an evolving area with no high-quality data in children to support its use. High-level guidance is needed in the areas of patient selection for non-operative treatment, different methods of ACLR, ACL repair, and AEAP reconstruction. Rehabilitation must consider the child’s skeletal maturity, individual anatomy, lifestyle, and access to specialist rehabilitation services.
Footnotes
Author contributions
C.T., T.A.K., F.A., M.T., and D.W.G. all contributed, in part, to the design, review, and completion of this current concept review.
Compliance with ethical standards
No institutional review board or ethic committee approval was required for this review. No human participants and/or animals for this review. No informed consent was required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.