
Abstract
Objective:
In this study, we examined whether there was a change in the number of children who had been screened by hip ultrasound, the age of first diagnosis, and the number of invasive and conservative treatments applied due to developmental dysplasia of the hip between 2016 and 2022 among refugees who were in “Temporary Protection Status” in Türkiye?
Methods:
The records were collected via the e-health database of the Turkish Ministry of Health. Over 1 month old were included in the study.
Results:
The number of ultrasonography (USG) that was performed for developmental dysplasia of the hip survey had significantly increased over time. The incidence for 5 years was 6 cases per 100 babies. However, the incidence of developmental dysplasia of the hip needing intervention was 0.4 cases per 1000 babies. In 2016, the most used diagnosis method was X-ray. By contrast, the use of USG has increased from 2016 to 2022. The mean age at the time of diagnosis was significantly high in 2016, 2017, and 2020. The number of invasive treatment modalities including closed reduction under anesthesia, open reduction alone, or open reduction with pelvic and/or femoral osteotomies had significantly decreased from 2016 to 2022. However, the number of abduction orthosis used for treatment also increased significantly.
Conclusions:
Free access to health services is effective in promoting families’ compliance with screening programs for developmental dysplasia of the hip. But is not enough for initial periods of mass migrations. To increase sensitivity to screening programs for possible diseases, further efforts are needed to prevent low compliance in early cases of mass migrations.
Introduction
The 21st century has seen substantial mass migration due to wars, seeking better living standards, and environmental factors like drought. Refugees face challenges accessing basic healthcare due to language barriers, social reactions, and cultural norms.1 –4
The United Nations High Commissioner for Refugees suggests safeguarding refugees through temporary protection to ensure unrestricted access to healthcare services. 5 However, host nations often face challenges in healthcare infrastructure, leading to issues such as overcrowding, resource shortages, prolonged wait times, and reduced participation in screening initiatives. 5 Moreover, understanding the healthcare access challenges faced by refugees in various countries remains limited in the current literature. 5 Since the developmental dysplasia of the hip (DDH) screening program is free and compulsory for immigrants as it is for locals in Türkiye, it can be used to evaluate the adaptation of immigrants to the health system and to understand whether language, sociocultural level, or education level creates barriers for immigrants to access the health system, even if it is free.6,7
In the present study, we assessed the impact of the provision of free health services to refugees with Temporary Protected Status in Türkiye on the management of DDH between 2016 and 2022. Specifically, we examined the changes in the number of children screened using hip ultrasound, the age at first diagnosis, and the number of invasive and conservative treatments employed. We hypothesized that over time, with refugees’ acclimation to the freely accessible healthcare system in Türkiye, there would be an increase in the use of hip ultrasound for screening and a decrease in the reliance on invasive interventional procedures for DDH management. By exploring these trends, we aimed to contribute to a better understanding of the effectiveness of free healthcare access and its impact on healthcare practices among refugee populations.
Materials and methods
The health documentation of infants in public, private, and university-affiliated healthcare establishments was procured through the electronic health database administered by the Türkiye Ministry of Health. 8 The research was executed in compliance with the principles outlined in the Declaration of Helsinki and was sanctioned by the Türkiye Ministry of Health. Ethical clearance was obtained with a provision for retrospective data analysis and adherence to laws safeguarding health information privacy, obviating the need for informed consent (ID: 95741342-020/27112019).
We conducted a computerized search of medical records to identify all refugee children under temporary protection with DDH in Türkiye. The e-health database was systematically queried utilizing International Classification Codes (ICDs) as per the guidelines set forth by the World Health Organization’s 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). Specifically, the ICD codes Q65, Q65.0, Q65.1, Q65.2, Q65.3, Q65.4, Q65.5, Q65.6, Q65.8, Q65.9, and S73.0, which pertain to hip reduction conditions, were employed to identify individuals born between January 2016 and December 2022, and who underwent screening for DDH. The search was performed in March 2023. Then patients undergoing conservative treatment or surgical intervention were extracted, allocated, and pooled using operation-specific procedure codes and treatment-specific codes (https://skrs.saglik.gov.tr/). A biostatistics specialist (ED), meticulously reviewed the entire dataset to ensure the accuracy of data entry and refinement and contribute statistical analyses. After a valid patient pool was created, the patients were divided into two groups according to the diagnostic method used: those diagnosed by DDH screening with ultrasonography and those diagnosed by X-ray, and the following data were extracted for all patients: sex, age, time and date of diagnosis, and treatment modality (any kind of abduction brace or observation (conservative treatment), closed reduction and spica cast under anesthesia, open reduction and spica cast, open reduction and/or pelvic, and femoral osteotomies). To assess diagnostic tools, only patients aged between 1 and 12 months were included. The study only included babies with refugee IDs. We only considered and analyzed the data related to the initial treatment attempts. Patients undergoing secondary or tertiary treatment attempts were not analyzed, as they were not the primary focus of this study.
Statistical analyses
The collected data underwent analysis through SPSS (version 22.0; IBM Corp., Armonk, NY, USA). Temporal trends based on age within years were assessed using Games-Howell and Tukey post hoc tests, while the one-way analysis of variance test was utilized to compare the means of age at the time of diagnosis. Pearson Chi-squared test along with Monte Carlo simulations employing Fisher’s exact test was employed to evaluate changes or trends in the number of performed different examinations, the number of detected DDH patients, and different treatment modalities from 2016 to 2022. For expressing quantitative attributes, the mean ± standard deviation was utilized. For qualitative attributes, figures in terms of numbers (n), frequencies, or ratios were presented. A significance threshold of p < 0.05 was employed to denote statistical significance.
Results
There were 3,419,328 refugees in Türkiye on 13 April 2023. Of the refugees under temporary protection, 49.3% were women of reproductive age (15–49 years). 9 More than 500,000 refugee children were born in Türkiye between 2011 and 2023. 10 However, only those born between 2016 and 2022 were included in the study.
The number of refugees under temporary protection increased from 2,834,441 in 2016 to 3,737,369 in 2021 and decreased to 3,535,898 in 2022 with the obvious effect of the decrease in the intensity of the ongoing war in Syria. However, the number of babies is increasing (Table 1). The number of recorded babies over 1 month old was 10,620 in 2016, while the number was 71,516 in 2022. Moreover, the number of times USG was performed for DDH screening was 635 (5.9%) in 2016 and 18,443 (25.7%) in 2022, showing a significant increase over time (p < 0.005). The number of times DDH was diagnosed between the same dates increased in line with the increasing number of live births. Accordingly, the incidence of DDH significantly increased from 2020 to 2022. From 2016 to 2018, the incidence was 1 per 100 babies and it was 11–13 cases per 100 babies from 2020 to 2022. The mean incidence for 5 years was 6 cases per 100 babies (Table 2). However, the incidence of DDH needing intervention was 0.4 cases per 1000 babies.
Demographics of patients and incidence from 2016 to 2022.
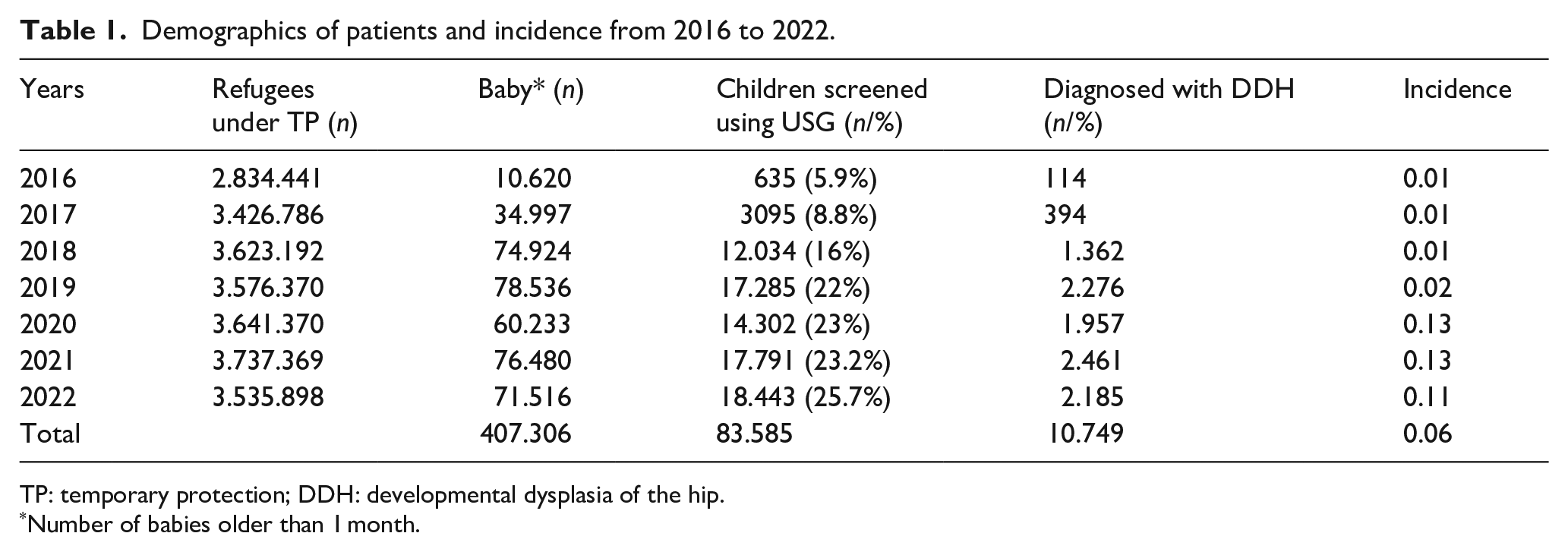
TP: temporary protection; DDH: developmental dysplasia of the hip.
Number of babies older than 1 month.
Characteristics of the treatment modalities.
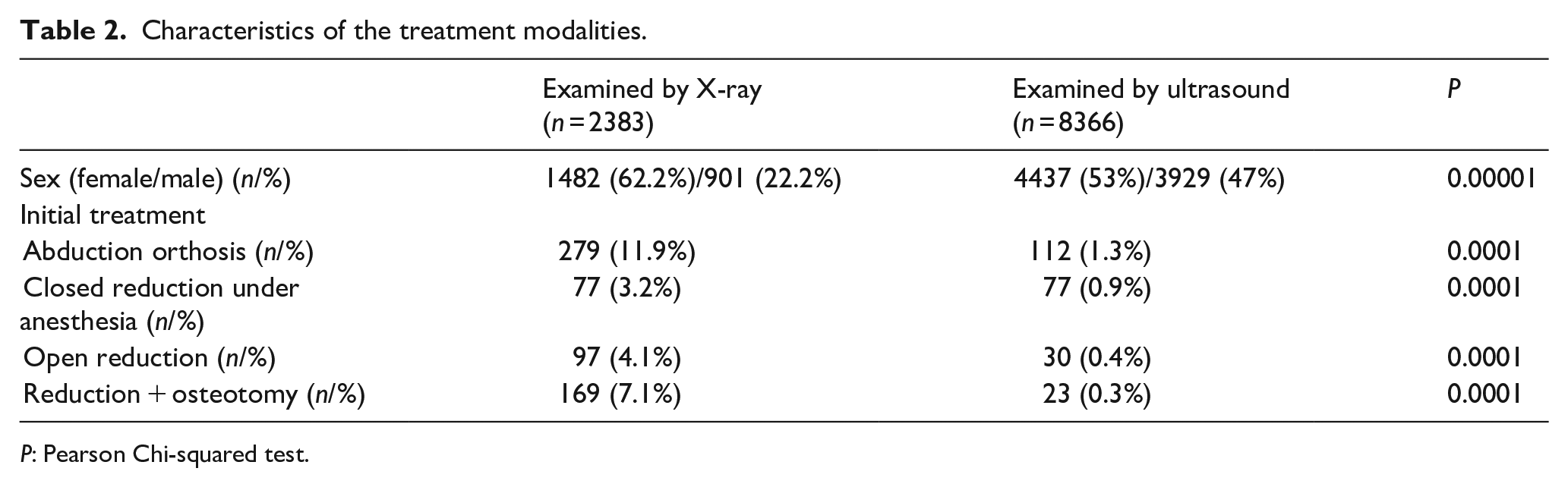
P: Pearson Chi-squared test.
Of the patients diagnosed with DDH, 391 were treated using abduction orthosis (3.6%), 154 (1.4%) were treated using closed reduction under anesthesia, 127 (1.2%) were treated using open reduction, and 192 (1.8%) underwent open reduction and pelvic and/or femoral osteotomy (Table 2).
All the interventions were significantly more frequent in the X-ray group, as expected, because patients who are diagnosed by X-ray with symptoms of DDH are frequently seen by a doctor after 4 months of age and symptomatic DDH usually needs intervention. USG may cause overdiagnosis in patients who do not require any intervention. We do not, however, have any information on the number of patients who had asymptomatic dysplasia needing intervention at older ages. Therefore, we cannot speculate whether overdiagnosis may have prevented the decrease in the number of future interventions or not for refugees (Table 2).
In 2016, the diagnostic method used most was X-ray (52.6%). However, this trend significantly changed over the years, decreasing to 22.2% in 2022. By contrast, the use of USG increased from 47.4% in 2016 to 80% in 2022, as expected. (Table 3). The mean age at the time of diagnosis was significantly high in 2016, 2017, and 2020 (p < 0.005) (Table 3). Only 864 (8%) of the children required an intervention. Of the patients, 9885 (91%) were only observed for dysplasia and did not receive any intervention from 2016 to 2022 (Table 3). As expected, the number of invasive treatment modalities, including closed reduction under anesthesia, open reduction alone, or open reduction with pelvic and/or femoral osteotomies, significantly decreased from 2016 to 2023. However, the number of times abduction orthosis was used for treatment increased significantly (Table 3). Among the babies diagnosed with DDH using ultrasound before reaching 6 months of age, 23 underwent open reduction and osteotomies (mean age at the time of surgery: 21.3 months, range: 15–37 months). These babies did not receive timely treatment despite the initial diagnosis.
Trends in diagnosis and treatment modalities over time.
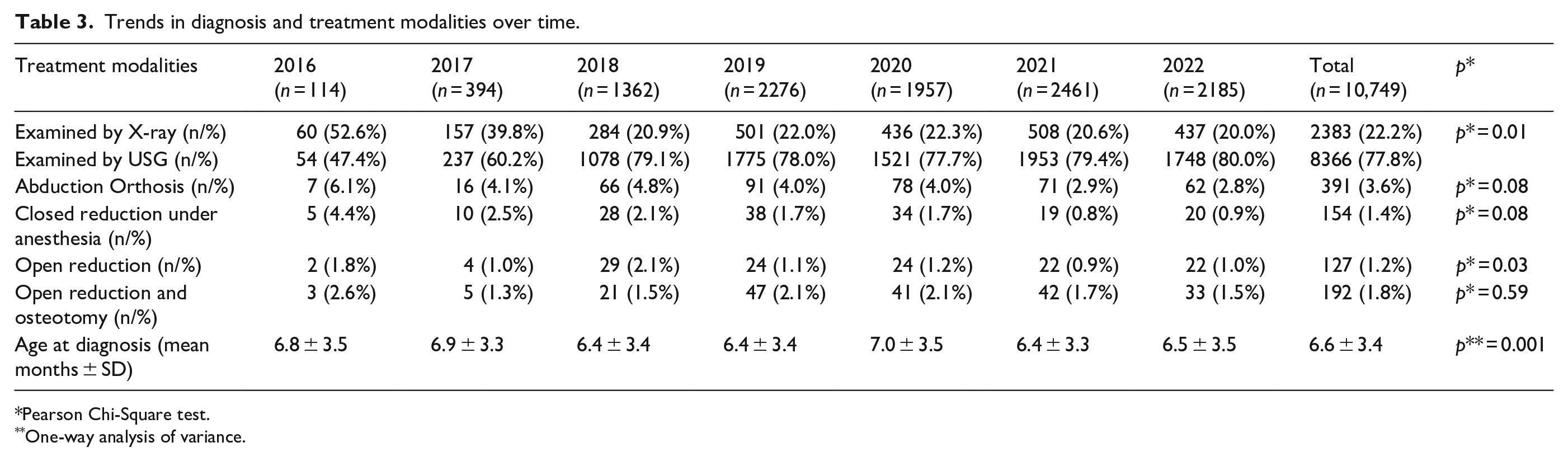
Pearson Chi-Square test.
One-way analysis of variance.
Discussion
In the present study, we evaluated the incidence of DDH among refugees under temporary protection and tried to understand whether free access to healthcare services prevented or delayed the diagnosis of DDH among these individuals between 2016 and 2022. Our results revealed that the number of USG examinations performed for DDH screening significantly increased over time (p < 0.005) and the number of DDH cases diagnosed between the same dates increased in line with the increasing number of newborns. The mean age at the time of diagnosis was significantly high in 2016, 2017, and 2020 (p < 0.005). Accordingly, the incidence of DDH significantly increased with time. All the interventions were significantly more frequent in patients diagnosed by X-ray (p < 0.005). The number of invasive treatment modalities including closed reduction under anesthesia, open reduction alone, or open reduction with pelvic and/or femoral osteotomies significantly decreased from 2016 to 2022. Moreover, the number of abduction orthosis used for treatment also increased significantly, showing increased early diagnosis with the screening program.
In this study, the X-ray and USG are used as markers to indicate early and late admissions to the screening program within the first year of the baby’s life. The incidence of DDH varies among populations and ethnic groups. However, early diagnosis enables early intervention with good results for every ethnicity. 11 The incidence of DDH has been reported to be around 0.17–0.471 per 1000 children in Türkiye.12,13 Unfortunately, the incidence of DDH among the Syrian population in their country of birth has not been studied to date. However, the incidence in neighboring countries having similar ethnicities of Arabs, Kurds, Druze, Jews, and Turkmens in Saudi Arabia, Israel, Iran, and Iraq has been reported to be around 0.31–0.57 per 1000 children. 11 The refugees from Syria are mostly combinations of those ethnic origins. Our study revealed that the number of babies screened for DDH in 2016 was very low, and many were late for their USG. By 2022, both timely and late admissions for screening had increased. Accordingly, the incidence of DDH significantly increased from 2016 to 2022. The increase in incidence could be attributed to several factors: (1) The increased number of USG screenings may have caused overdiagnosis, particularly for Type 2a hips. (2) Babies missed in the screening program in early 2016 and 2017 may have had late or undiagnosed, symptomatic or asymptomatic DDH. This cannot be confirmed or refuted, as these patients were not included in the study to maintain data homogeneity. (3) The increased participation in the screening program may have revealed the true incidence of DDH. We believe a combination of the first and third reasons is likely true. Graf type 2a physiologically immature hips, which require re-evaluation and are defined as DDH. Generally, most of these patients heal with no need for intervention. There is an ongoing debate about whether these hips should be defined as DDH or not. 14 As this was an incidence study partly, we think that these hips also must be defined as DDH because they have the potential to not heal and require intervention. 15 This is supported by the data in Tables 2 and 3, showing a higher number of babies diagnosed with DDH compared to those who underwent intervention. However, the incidence of DDH needing intervention was 0.4 cases per 1000 babies, in accordance with previous studies.
Syrian nationals, as well as stateless individuals and refugees originating from Syria, who have arrived in Turkey, are granted temporary protection under the auspices of the Turkish government.5,16 Refugees under temporary protection have the right to access all public health services completely free of charge. Syrian refugees have completely different cultural codes and education levels. Refugees staying in Türkiye instead of moving to Europe are generally not qualified, have low levels of education, and cannot speak Turkish.17 –19 Recent studies on the quality of primary healthcare services given to refugees revealed several problems due to cultural disparity and the language barrier in Europe and Türkiye.20 –24 In our study, the low rate of admission to healthcare facilities during the first 2–3 years may have had several reasons. Post-traumatic stress disorder, depression, low educational level, anxiety about finding shelter and settling into a new sustainable life, and adaptation to a different culture may have resulted in indifference to screening programs even if access to the service is free. However, the increase in numbers in terms of screening, incidence, and conservative treatment and a decrease in the number of invasive interventions are evidence of adaptation. We think that free access to health services may have further enhanced this adaptation as, after 2–3 years of the shock of facing a new culture, the number of screenings seems to be very high from 2019 to 2022. However, the relatively increased delay in diagnosis in 2020 should be attributed to the COVID-19 pandemic, which affected the whole society rather than only refugees. Various factors, including limited healthcare resources and services, might have hindered the prompt initiation of appropriate treatment. This highlights that unrestricted access to healthcare is not enough; additional efforts are required to facilitate refugees’ access to modern healthcare systems.
Tsagkaris et al., 25 in their paper on screening programs for refugee and immigrant children in Europe, recommend developing long-term strategies since the EU currently lacks a comprehensive plan for early DDH detection in this vulnerable group. It has been shown that solutions for refugees’ health issues that focus solely on responding to emergencies often result in fragmented and chaotic interventions, rather than fostering structural changes within European health systems. 26 The authors concluded that addressing DDH in refugees requires early screening and detection. This involves ensuring all migrant newborns and infants receive routine clinical assessments and follow-up ultrasound imaging, which is cost-effective and radiation-free. Improving access to these screenings in refugee camps and enhancing health literacy among migrant families are essential steps. Despite Turkey’s accommodating approach toward Syrian refugees, the provision of comprehensive healthcare services, and extensive efforts, the admission rate to hospitals for DDH screening in our study was only 25%. Furthermore, the insufficient capacity of healthcare facilities to accommodate the surge in admissions due to the increased demand may also lead to challenges in accessing health services. Although translators were introduced in specific hospitals, their effectiveness remains unassessed in this study. Despite being compulsory and free, the lack of materials and advertisements in refugees’ languages undermines the concept of “compulsory” since there are no penalties for either locals or refugees who do not complete the screening program. These factors collectively contribute to decreased adherence to the screening.18,27 However, we do not have enough data to comment on this issue. Nevertheless, free access to health services has enabled adaptation and encouraged increasing participation in screening programs in the mid-term.
The primary limitation of our study is its retrospective nature, relying on government-based health registry data. This could introduce selection bias, as the data were not originally collected with this specific research question in mind. Furthermore, the data might lack comprehensive details on potential confounding variables, such as overall health status, the sensitivity of the diagnostic tools used, coexisting conditions, and social determinants of health, which may influence the outcomes. The results may also have limited generalizability to other refugee populations or non-refugee groups, due to the unique characteristics of refugees with Temporary Protected Status in Türkiye. External factors, such as political, economic, and societal shifts in Türkiye or the refugees’ countries of origin, might have impacted health-seeking behavior but were not examined in our study. Data misclassification or coding errors in the registry could affect result accuracy, while limited follow-up information may hamper the assessment of long-term outcomes for children diagnosed with DDH. These considerations should be borne in mind when interpreting the study’s results and planning future research in this area.
Conclusions
While free access to health services proves to be effective in promoting compliance with DDH screening programs among families, it is not sufficient during the initial periods of mass migration. To enhance the sensitivity and effectiveness of screening programs for potential conditions like DDH, concerted efforts are needed. It is essential that our healthcare systems adapt and respond to the unique needs of these vulnerable populations to ensure equal access and outcomes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241299318 – Supplemental material for Exploring the impact of developmental dysplasia of the hip on refugees with temporary protected status in Türkiye
Supplemental material, sj-pdf-1-cho-10.1177_18632521241299318 for Exploring the impact of developmental dysplasia of the hip on refugees with temporary protected status in Türkiye by Izzet Bingöl, Murat Taşcı, Niyazi Erdem Yaşar, Naim Ata, M Mahir Ülgü, Şuayip Birinci, Yavuz Sağlam and Mehmet Salih Söylemez in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
All authors made appropriate contributions to the conception and design of the study.
Authors’ contributions
MSS and NEY: Design of the study, statistical analysis, development of checklists, interpretation of data, writing of the article, drafting and revision of the article. IB: Acquisition of data, co-writing of the article. NA, MMÜ, and SB: Contributed to the acquisition and analysis of the data. YS and MT: Contributed to the interpretation of the data and design of the research. All authors critically revised the manuscript, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki and received approval from the Turkish Ministry of Health with a waiver for informed consent for retrospective data analysis and the health information privacy law (ID: 95741342-020/27112019).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.